
Abstract
Aim
The aim of this article is to analyze the epidemiological and clinical features of migraine in a pediatric headache center.
Methods
A retrospective study was performed over six years. Hospital record databases were screened for the diagnosis of migraine with aura (MA) or without aura (MO), based on the ICHD-II criteria. Statistical analysis: Fisher’s test or Mann-Whitney U test, significance at p < 0.05.
Results
Migraine was diagnosed in 495 children (29.7% MA, 70.3% MO). The majority of diagnoses were made between ages 9 and 14 years. After stratification for age into five groups, we observed an increase of diagnoses in females, with a peak after the age of 15 years, and an increase of MA. In both groups, the attacks were usually severe, infrequent (<1–3/month) lasting <2 hours, and associated with nausea/vomiting, photophobia, phonophobia (more frequent in MO). Osmophobia was reported in 24.7% of the patients with MO. Dizziness was more frequent in patients with MA. Visual auras were the most common occurrence (87.1%). Confusional state was observed in 10.88% of the patients. A positive family history of headache was observed in >88% of the patients.
Conclusion
We describe the characteristics of pediatric migraine based on the ICHD-II criteria, showing a likely significant loss of diagnoses using the ICHD-III beta. The incidence of migraine increases with age. MO occurs more commonly and shows more frequent attacks and a higher prevalence of associated symptoms, in particular osmophobia. Although males are prevalent in the entire sample, the proportion of females is higher among patients with MA in all of the age groups. Phenotype and sexual prevalence of migraine acquire adult characteristics and become more frequent in females from the onset of puberty.
Introduction
Primary headaches, especially migraine and tension-type headache, are the most frequent cause of headache in children and adolescents, although secondary ones and unusual causes should be considered as well (1). The study of migraine in the pediatric population is critical because of its burden on children and their families and the diagnostic and therapeutic difficulties determined by varying phenotype and possible differential diagnoses (2). Indeed, migraine is increasingly recognized as a debilitating disorder whose early recognition is a primary endpoint for pediatricians.
In recent decades, several definitions of pediatric migraine have been proposed based on its peculiarities in childhood (2). The currently accepted classification system for migraine, which was published by the International Headache Society in 2013, is known as the International Classification of Headache Disorders (ICHD-III beta) (3). Such criteria distinguish migraine without aura (MO) and migraine with aura (MA); other variants, such as episodic syndromes that may be associated with migraine (previously known as periodic syndromes of childhood) and likely migraine, have also been defined by the ICHD-III beta, as well as chronic migraine.
Migraine is considered to be a heterogeneous disorder: attacks may vary in terms of the intensity of pain, duration, pattern of associated features and frequency (4,5). The overall prevalence ranges from 3% in children aged 3–7 years to 23% in teenagers (6); however, epidemiological studies are challenging. The wide prevalence is primarily due to methodological differences and difficult diagnoses in early ages. Therefore, demographic characteristics of patients, profiles of attacks, symptoms as well as personal and familial history and physical and neurological examinations constitute the basis for correct and timely diagnoses.
The aim of our study was to analyze the epidemiological and clinical features of pediatric MA and MO in a cohort of patients evaluated at our pediatric headache center over a six-year period.
Methods
A retrospective case-only study was performed over six years, between January 2006 and August 2012. All of the children initially screened for episodic MA or MO at our Pediatric Headache Centre (Regina Margherita Children’s Hospital, Turin, Italy) were enrolled in the study. Migraine was diagnosed according to the International Headache Society’s International Classification of Headache Disorders, second edition (7) because the ICHD-III beta was published after our patients had been referred to our center.
The exclusion criteria were as follows: the presence of any disorder related to headache (intracranial tumors, inflammatory diseases, nerve trunk pain, any disorder of facial cranial structures, cranial neuralgias and recent head injuries), chronic daily headache, cluster headache, chronic migraine or any other form of headache or migraine different from episodic MO or MA, as well as chronic systemic diseases or insufficient data in the database.
The medical record databases of our center were screened for information relative to the demographic profile of children (age, sex, and ethnicity), clinical features of migraine, associated symptoms, and personal and familial medical history. Headache diaries were used for evaluating the duration, severity and intensity of pain. The duration of migraine episodes was considered and was divided into brief (≤2 hours) or long (>2 hours) periods. Headache severity was categorized as mild, moderate or severe. The average number of attacks per month was registered and the frequency was defined as infrequent (one to three attacks/month), moderately frequent (four attacks/month) and frequent (>4 attacks/month). Associated symptoms included nausea and vomiting, photophobia, phonophobia, osmophobia, dizziness and vertigo. In patients with MA, aura symptoms were evaluated. A detailed personal medical history was obtained for all of the patients, with particular attention to medication use, hypertension, overweight/obesity and diabetes. A family history of idiopathic headache was recorded. Finally, comorbidity with ocular refraction defects, allergy and asthma were analyzed. All of the enrolled participants had undergone physical and neurological evaluations during their initial visit at our center.
The study was performed according to the international regulatory guidelines and current codes of Good Epidemiological Practice. Because patient care was not altered by inclusion in the study, the approval of the ethics committee was not necessary.
Statistical analysis
Statistical analysis was performed using SAS software for Windows, version 9.2 (SAS Institute Inc, Cary, NC, USA).
The data are described as the mean ± standard deviation (SD) values or medians and interquartile ranges (IQRs) for continuous variables, and absolute and relative frequencies for categorical variables.
The chi-squared test or Fisher’s exact test was used to evaluate proportions, as appropriate. The nonparametric Mann-Whitney U test was performed to evaluate comparisons within quantitative variables.
Two multivariate logistic models were built to evaluate the relationships between aura and several personal variables (model 1) and personal and clinical variables (model 2). Individuals with missing values for at least one of the variables included in the models were excluded from the analyses.
A p < 0.05 was considered to be statistically significant, and all of the p values were based on two-tailed tests.
Results
The study population consisted of 495 children (median (IQR) age, 10 (3) years; range, 3–18 years). A total of 147 patients (29.7%) suffered from MA, whereas 348 patients (70.3%) had MO. Twenty-seven additional patients examined in the same period experienced just one episode of MA: according to ICHD-II (7), they could not receive a definitive diagnosis; hence, they were excluded from the present study.
Characteristics of the study population.

M: male; F: female; IQR: interquartile range; MA: migraine with aura; MO: migraine without aura.
Characteristics of the study population after stratification into five age groups (≤5 years, 6–8 years, 9–11 years, 12–14 years and 15–18 years).
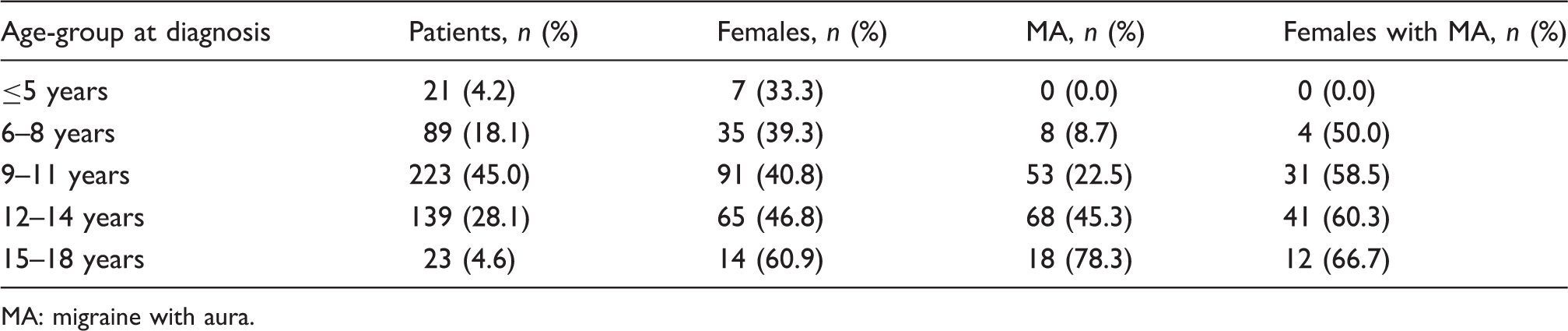
MA: migraine with aura.
A significant difference between the patients with MA and MO was found relative to sex (p < 0.001) and age at the time of diagnosis (p < 0.001). The children with MA were older than those with MO (median age (IQR): 12.00 (2) and 9.00 (3), respectively; range, 6–18 years and 3–16 years, respectively) and more frequently were females (males/females, 59/88 and 224/124, respectively).
In all of the participants, the physical and neurological examinations on the initial visit at our center proved to be negative and the clinical presentation of migraine was unchanged between the first appearance and the time of consultation.
Migraine features in patients with MA and MO.

Fisher’s exact test. MA: migraine with aura; MO: migraine without aura.
Multivariate logistic regression for MA vs MO.

Variables included in models are: sex, age at diagnosis, and ethnicity (model 1) and sex, age at diagnosis, ethnicity, number of attacks/month, severity, duration, photophobia, phonophobia, osmophobia, nausea/vomiting, and vertigo and dizziness (model 2).
MA: migraine with aura; MO: migraine without aura; CI: confidence interval.
Among the children with MA, the auras were usually visual (87.1%), followed by sensory (38.5%) and language (15.6%) auras; 10.9% of the patients presented with a confusional state. The various combinations of aura symptoms are reported in Figure 1.
Venn diagram showing the distribution of aura symptoms. Two patients presenting an exclusively confusional state are not shown in the diagram; 21 more patients have been excluded from the diagram because of missing data about their symptoms.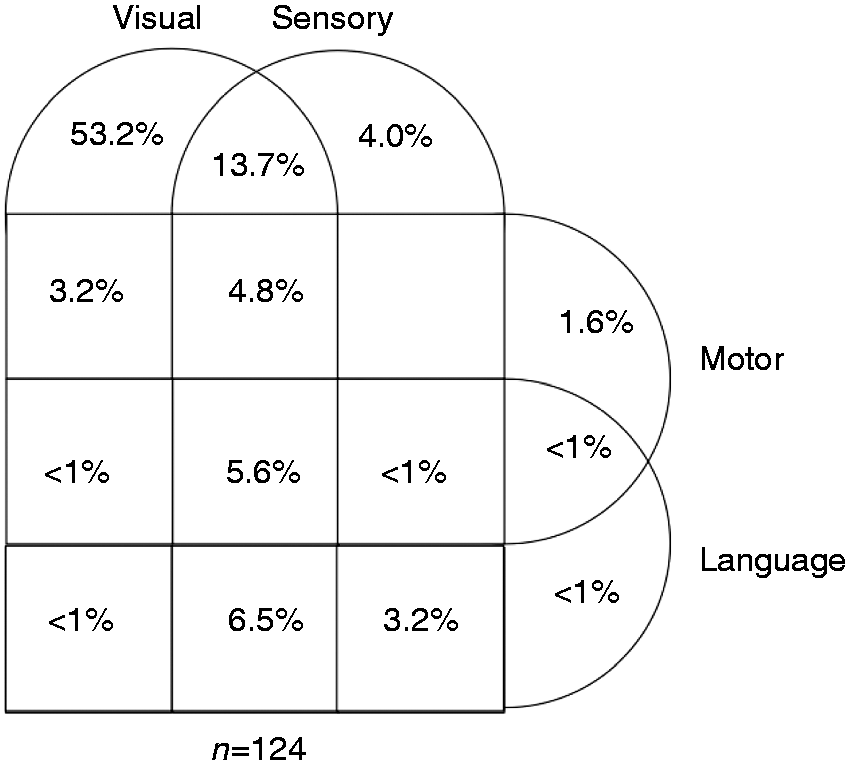
Among all ages, 37.4% of the children with MA and 43.1% of the children with MO had a previous medical history. Allergy and asthma were significantly more common in children with MO (p = 0.001). Cardiac diseases were less frequently reported. A total of 130 individuals (88.4%) with MA and 323 individuals (92.8%) with MO had a familial history of migraine, most commonly in a first-degree relative.
Ocular refractive disorders were observed in 19.0% of the patients with MA and 21.0% of the patients with MO.
Finally, we evaluated the incidence of risk factors for cardiovascular disease. Nobody reported any intake of alcohol or oral contraceptives. Hypertension was diagnosed in one patient with MA and in four patients with MO. Only one child belonging to the MA group smoked; six children with MA and 13 children with MO were obese or overweight. One diagnosis of diabetes was performed in the MA group and three in the MO group. Although the majority of children in both groups usually did not take any medication, the proportion of patients in any type of therapy (for any condition other than migraine) was significantly higher in the MA group (p = 0.001).
Discussion
This retrospective study on children referred to our headache center in Northern Italy presented novel findings on epidemiological and clinical features of migraine in pediatric patients.
Distribution by gender and age
In the entire sample, the proportion of males was higher than females. However, stratifying the population by age and in particular considering the different distribution in pre- and peri-pubertal (<12 years) and pubertal-adolescent (≥12 years) patients, we observed an increased frequency of females in the second group, in accordance with the major epidemiological studies available. Additionally, the higher the age, the higher were the proportion of females and the frequency of MA. Generally, no gender difference is reported in childhood. The same distribution in both sexes or a greater distribution in males is described, depending on the studies. Migraine becomes more common in females during adolescence (8). Indeed, a positive trend for the prevalence of migraine is reported from preschool up to school age, with a sharp increase in pubertal children and adolescents (9). We have confirmed this observation in our study because the majority of the diagnoses were made between the ages of 9 years and 14 years.
MA and MO distribution
Approximately 30% of our patients suffered from MA, confirming the data reported in other studies (10). We were impressed by the high percentage of adolescents with MA in our population, presumably because our facility is the reference center for patients with pediatric headache and migraine in our region. In fact, aura symptoms usually frighten both children and their families and present concerns for the general practitioner, who refer adolescents with MA to our center more frequently than patients with MO.
Migraine features
The attacks were generally less frequent and shorter in the pediatric population than in adults, although they may occasionally emerge upon awakening in the morning and fade with sleep. Usually, the younger the child, the more optimal the response to analgesic therapy. Comparing the two groups, our children with MA were older and more frequently female compared to those with MO. The patients with MA typically had fewer attacks/month (infrequent disease) with a higher reported intensity but shorter duration (often lasting less than two hours). This observation is interesting because, according to the ICHD-III beta, the minimum duration of a single attack requested to diagnose migraine has been arisen from one to two hours (3); thus, based on the new criteria, the majority of our patients with either MA or MO diagnosed according to the ICHD-II and experiencing attacks <2 hours would be missed.
The majority of patients with MO reported <3 attacks/month; however, there was an increasing number of individuals suffering from more frequent attacks; the higher the number of attacks, the lower the likelihood of suffering from MA.
In both groups, the most frequent symptoms were nausea and vomiting, and photophobia and phonophobia, whose prevalence was higher in patients with MO, as has previously been reported (10). Osmophobia occurred more frequently in patients with MO, affecting approximately 25% of the participants, whereas dizziness and vertigo occurred more frequently in the MA group. In particular, osmophobia has been considered to be a significant symptom only in recent years. A multicenter Italian study has underscored its importance in diagnosis (11,12) and it has been included among the primary accompanying symptoms of migraine in the ICHD-III beta although it is less frequently reported than photophobia and phonophobia (3). Additionally, dizziness and vertigo are common accompanying symptoms (13). Vertigo is also described as an independent entity (benign paroxysmal vertigo) among the episodic syndromes that may be associated with migraine, previously known as childhood periodic syndromes. When associated with migraine, it can both precede and be concomitant to the attack. In our experience, dizziness was more frequently reported than vertigo.
In our study, aura was usually visual; sensory disturbances (including numbness and paresthesia of the face, tongue and upper limb with pins-and-needles sensation), speech difficulty and confusion were not infrequent, as had previously been described both in children and adults (14–16). Acute hypotonia of an arm or, less frequently, a leg is extremely rare and should be more properly described as “weakness” than true paresis, which is otherwise typical of hemiplegic migraine.
Comorbidities
In our sample, 8.84% of the patients with MA and 16.38% of the patients with MO reported a history of allergy and asthma, whereas epilepsy was observed only in one patient with MA and in three patients with MO. Comorbidities, such as neurological disorders, including epilepsy, and inflammatory conditions, such as allergies and asthma, have been recently observed in pediatric migraineurs (17,18); however, a direct correlation with migraine can hardly be determined based on the available evidence. In particular, data regarding the likely cause-effect relationship between allergic factors and migraine are still controversial and, to date, no study has confirmed this hypothesis.
Family history
Finally, in our study, more than 88% of the children with MA or MO had a positive family history, compared to 60% to 77.5% reported in the literature (19); in nearly all of the cases, at least one first-degree relative with headache was described. These data confirmed that familial headache is a predisposing factor for the development of such a disorder in childhood and suggested the implication not only of biological susceptibility but also of environmental factors.
Limitations of the study
A limitation of the study is the difficulty in collecting precise information regarding the clinical characteristics of migraine, particularly the duration of the attacks and aura features. The younger the patients, the less precise is their perception of time, particularly when they are in pain. Moreover, what they suffer from is often referred and filtered by their parents, which could have in part affected our results. This common and predictable bias in pediatric studies makes our results comparable to those reported by other authors. We suggest that these aspects should be considered in the validation of the ICHD-III beta, particularly in the duration of attacks, to avoid a likely significant loss of diagnoses.
A second limitation is that our data come only from initial visits at our center. Often, children show an evolution of migraine features progressively as they grow up, which is in part due to their capacity to better describe their symptoms as they get older. Occasionally, the diagnosis can be confirmed based on the ICHD criteria after the first symptom presented and not at the initial visit. It could be interesting to re-analyze with additional studies the eventual modifications of diagnosis in the same children some months after the initial visit.
Conclusions
In conclusion, our study described the characteristics of MA and MO in the pediatric population based on the ICHD-II criteria and demonstrated a likely significant loss of migraine diagnosis using the ICHD-III beta criteria. Migraine can affect people throughout childhood; however, its incidence increases as the individuals grow older. MO is more common, shows more frequent attacks and higher prevalence of associated symptoms, with osmophobia affecting nearly 25% of the patients. Although males are prevalent in the entire sample, the proportion of females is higher among MA patients in all of the age groups. Phenotype and sexual prevalence of migraine change with age, acquiring adult characteristics and becoming more frequent in females from the onset of puberty. Additional studies using a larger pediatric population are warranted to confirm our observation.
All of the research material related to our paper is available by contacting the corresponding author.
Clinical implications
The majority of patients with either migraine with aura (MA) or without aura (MO) diagnosed according to the International Classification of Headache Disorders, second edition (ICHD-II) in our study had attacks that lasted <2 hours and would be missed using the ICHD third edition beta (ICHD-III beta) criteria. Osmophobia was reported in nearly 25% of the children with MO, suggesting that its role could be reconsidered in the definition and classification of migraine. Males were prevalent in our sample; however, the proportion of females was higher among the patients with MA in all age groups; we also observed an increased number of adolescents among patients with MA.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.