
Abstract
Patients with functional gastrointestinal disorders frequently report migraine. We aimed to determine the prevalence of idiopathic upper abdominal symptoms in patients with migraine and compare it with a control population of healthy blood donors. We assessed abdominal symptoms using the Bowel Disease Questionnaire in a series of 488 consecutive blood donors without migraine and 99 patients with migraine. Upper abdominal symptoms were reported by 38% [95% confidence interval (CI) 32, 44] of blood donors compared with 81% (67, 91, P < 0.001) of migraine patients. Of the blood donors, 23% (18, 28) reported frequent dyspepsia compared with 60% (44, 74, P < 0.001) of the migraine patients. Migraine was associated with frequent upper abdominal symptoms (odds ratio 2.7, 95% CI 1.2, 6.1) after adjusting for age, gender, smoking and consumption of analgesics and alcohol. Upper abdominal symptoms are significantly more frequent in patients with migraine compared with healthy controls. The association between migraine and idiopathic upper abdominal symptoms may suggest common pathophysio-logical mechanisms.
Introduction
Headache, migraine and symptoms of upper gastrointestinal distress are among the most frequent complaints seen by physicians. Various gastrointestinal conditions have been linked with migraine, although it is uncertain if these symptoms represent manifestations of the migraine attack. Comorbidity between migraine and other gastrointestinal disorders, such as hiatal hernia, colitis or abdominal pain, have been reported among migraineurs (1). Abdominal migraine is well recognized in children (2) but, in spite of anecdotal reports (3), migraine is not established to be associated with abdominal pain in adults (4).
Migraine and headache are frequently reported by patients with gastrointestinal symptoms (5–7), but in contrast, data on the prevalence of dyspeptic symptoms in migraine patients are lacking. We therefore aimed to evaluate the prevalence of idiopathic dyspeptic symptoms in patients with migraine and compared it with a control population of healthy blood donors without migraine.
Patients and methods
During a 6-week period in 1998, 99 consecutive migraine patients with or without aura from the headache clinic of the Department of Neurology, University Hospital, Essen were included in the study. After giving informed consent, all migraine patients underwent a physical examination and an evaluation by an experienced neurologist. The diagnosis of migraine was based upon the 1988 International Headache Society criteria (8). We compared the migraine patients with a group of 488 apparently healthy subjects without reports of migraine or headache, who were eligible for a blood donation at the same institution and who gave permission to participate in the study.
Assessment of abdominal symptoms
We used the German version of the Bowel Disease Questionnaire (9), which was previously validated and has been shown to have adequate content as well as predictive and construct validity for the measurement of gastrointestinal tract symptoms (6, 9). Standardized criteria were utilized for the categorization of symptoms based on previous studies (10). Briefly, subjects who reported pain centred in the upper abdomen during the previous year were classified as having dyspepsia; those with pain more than six times during the last year were considered to have frequent dyspepsia (11).
Other potential risk factors for gastrointestinal symptoms, including smoking, high alcohol consumption (defined as more than six alcoholic beverages per week) and use of analgesics (aspirin, other non-steroidal anti-inflammatory drugs, or paracetamol) were also ascertained on the questionnaire.
Statistical analysis
We compared the prevalence among migraineurs with healthy blood donors using non-parametric test statistics (12). We used logistic regression to calculate the prevalence odds ratio (OR) and the 95% confidence interval (CI) of the association between migraine and dyspeptic symptoms, adjusting for age, gender, alcohol consumption and intake of any analgesics. All P-values were two-tailed; an α level of <0.05 was considered statistically significant.
Results
A total of 198 (33.7%) of the blood donors and 75 (75.8%) of the migraine patients were female. The mean age in the blood donor group (34.1 ± 0.5) and in the migraine group (41.5 ± 1.22), as well as analgesic intake differed significantly. Smoking status and alcohol consumption did not differ between the groups.
The frequency of several abdominal symptoms in the group of healthy blood donors and the group of migraine patients is summarized in Table 1. The overall prevalence of upper abdominal pain during the last 12 months was 44.1% (95% CI 38.6, 49.7). A total of 81 migraine patients (80.9%) reported upper abdominal symptoms compared with 183 healthy blood donors (37.5%). The reported prevalence of abdominal pain and frequent abdominal pain in the control group leveled off over the age of 50, whereas the prevalence among migraineurs remained high, as shown in Fig. 1.
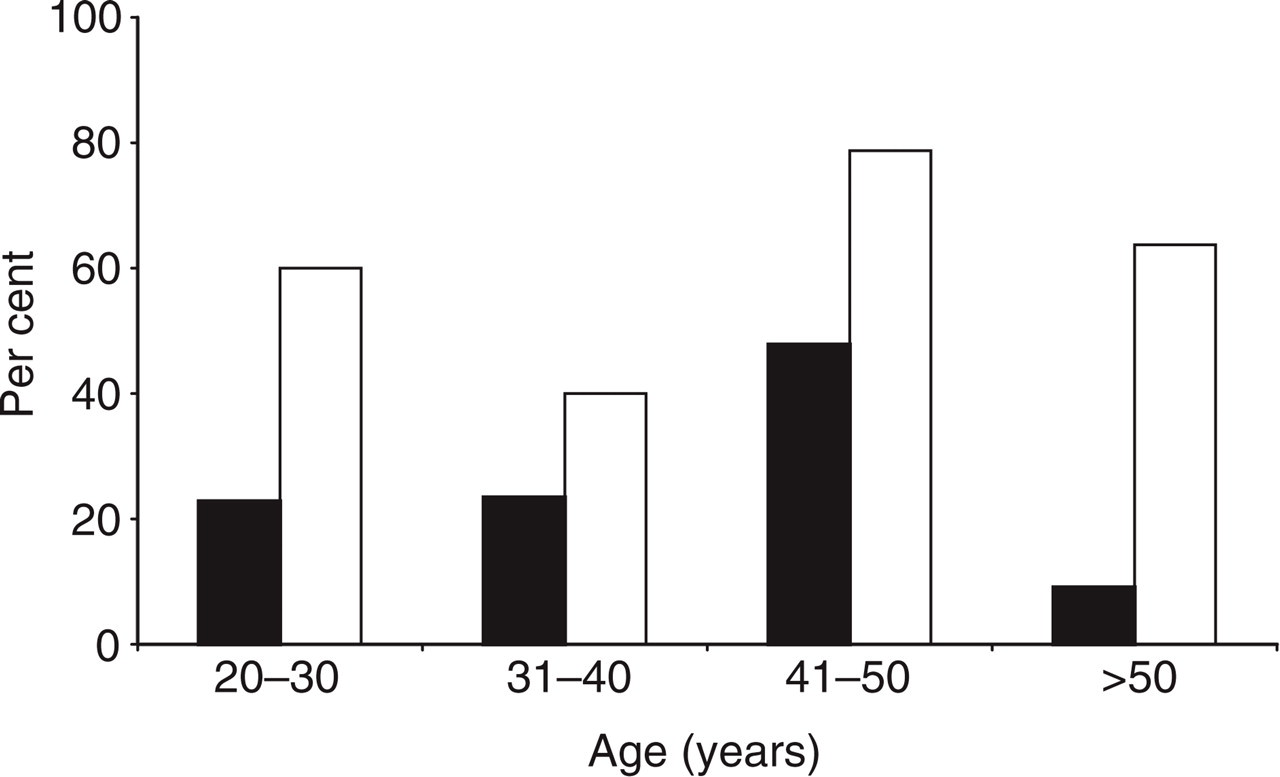
Frequency of idiopathic dyspepsia in healthy blood donors (▪) and migraine patients (□) in different age groups.
Frequency of gastrointestinal symptoms in healthy blood donors and patients with migraine

After adjusting for the potential confounders age, gender, smoking, alcohol consumption and analgesic use, the prevalence odds of idiopathic upper abdominal symptoms in migraine patients was 170% increased compared with healthy blood donors (OR 2.7, 95% CI 1.2, 6.1; P < 0.001).
All migraine patients and controls who consumed analgesics reported use between 0.5 g/week and 1.5 g/day. Interestingly, there was no association between the dose of analgesic and the severity of gastrointestinal symptoms. We evaluated the prevalence of dyspepsia in healthy blood donors and migraine patients stratified by aspirin intake. In both groups, aspirin users and non-users, the prevalence of dyspepsia was substantially increased among migraineurs when compared with controls (Fig. 2). The difference was statistically significant in the non-aspirin group (P < 0.001) and marginally significant in the aspirin group (P = 0.079). The result was similar for other analgesic types (data not shown).

Frequency of idiopathic dyspepsia in migraine patients (□) and healthy controls (▪) according to aspirin intake.
Discussion
In the present study we have shown that the prevalence of idiopathic upper abdominal symptoms is increased in a population of migraine patients compared with a population of healthy blood donors. Although the groups differed in age, gender and analgesic intake, the odds ratio for dyspepsia was still twofold increased in migraineurs compared with healthy blood donors, when we adjusted for these and other potential confounders. Our data further did not indicate that the higher prevalence of dyspepsia was induced or modified by analgesic intake.
Our study has several strengths, including neurologist-confirmed migraine diagnosis, a large number of healthy controls, and the use of a standardized and validated questionnaire to ascertain gastrointestinal symptoms.
Several limitations should be considered. The result of our study may have limited generalizability. Individuals in our control group may have been healthier compared with the general population and thus may have had lower prevalence of dyspepsia. However, compared with other studies that have used the Bowel Disease Questionnaire (5, 6, 10, 13), the prevalence of dyspepsia in our control group was rather high (37.5%). In addition, another study did not find differences in the prevalence of dyspepsia and other gastrointestinal complaints in this particular control group compared with random population-based samples (6). Thus, while blood donors may not be completely representative of persons in the general community, we believe that the results are generalizable with regard to the prevalence of dyspepsia. The migraine patients were a selected population, and we cannot exclude referral bias. However, we believe that referral of migraine patients was independent of gastrointestinal symptoms and that this potential bias does not fully explain the substantial qualitative difference in the prevalence of dyspepsia between the groups. Further, despite multivariable adjustments, confounding remains a potential alternative explanation of our findings. Finally, because of the limited sample size, we were unable to evaluate the prevalence of dyspepsia stratified by different migraine characteristics including migraine severity. As all patients were recruited at the out-patient clinic of a tertiary referral centre, it is reasonable to assume that our population was biased towards more severe patients.
The 1-year prevalence of dyspepsia in different populations varies between 7% and 41% (5, 6, 10, 13). This variability might partly be due to variations in symptom ascertainment. The prevalence of dyspepsia in studies that also used the Bowel Disease Questionnaire ranged from 25.8% (10) to 29.3% (6).
The obvious lack of an association between the dose of aspirin or other analgesics and severity of dyspepsia could be explained by insufficient statistical power. While the dose of a non-steroidal anti-inflammatory drug might be linked to the severity of mucosal lesions, the severity of the lesion does not determine symptoms. However, in a recent study (14), gastric mechanosensory function (i.e. the sensory threshold for the perception of gastric distensions) was linked to symptoms. Thus, it might be speculated that differences in the mechanosensory thresholds play a role in the manifestation of concomitant gastrointestinal symptoms.
The association between migraine and dyspepsia is largely unknown and there is an ongoing debate about the underlying pathophysiology. It has been shown that abnormal visceral mechanosensory and vagal function play a role at least in subgroups of dyspeptic patients (15–17). A disturbance of visceral nerves is also involved in the pathophysiology of migraine (18, 19). In addition, the involvement of several neuropeptides has been discussed for both migraine (20–23) and dyspepsia (24–26). In particular, the neuropeptide calcitonin gene-related peptide (CGRP) has been consistently shown to be increased during the migraine attack (21–23). Receptive relaxation of the gastrointestinal tract is mediated by vagal motor fibres. CGRP is an important neurotransmitter of the inhibitory sensory neuron, and it has been hypothesized that disorders of reservoir functions may result in symptoms of functional dyspepsia (27). Indeed, results from animal studies suggested the involvement of CGRP in the number of abdominal contractions (24) and that CGRP plays a role in visceral afferent nerve sensitization of gastrointestinal origin (25). In humans, however, the association between CGRP and dyspepsia is less clear (26).
There is some evidence that Helicobacter pylori infection is more frequent in patients with functional dyspepsia compared with asymptomatic healthy controls (28) and that H. pylori infection rates are increased in migraine patients (29). In contrast, other studies do not support H. pylori as an important risk factor for functional dyspepsia (6, 30) or migraine (31) or find little evidence to support the use of H. pylori eradication therapy in patients with non-ulcer dyspepsia (32).
In summary, we found increased prevalence of idiopathic dyspepsia in patients with migraine compared with healthy control individuals. Several similarities in the pathophysiology of both migraine and idiopathic dyspepsia may indicate a common underlying cause.