
Abstract
Background
Spinal manipulation may reduce migraine frequency, but effects of multimodal chiropractic care on migraine frequency have not been evaluated.
Methods
We conducted a pilot randomized controlled trial comparing multimodal chiropractic care + enhanced usual care (MCC+) versus enhanced usual care alone (EUC) among adult women with episodic migraine. EUC was comprised of usual medical care and migraine education literature. MCC+ participants received 10 sessions of chiropractic care over 14 weeks. Primary aims evaluated feasibility of recruitment, retention, protocol adherence, and safety. Change in migraine days was a secondary aim.
Results
Of 422 patients screened, 61 were randomized over 20 months. Fifty-seven (93%) completed daily migraine logs during the intervention, 51 (84%) completed final follow-up, and 45 (74%) completed all assessments. Twenty-four of 29 MCC+ participants (83%) attended > 75% of the chiropractic sessions. Ninety-eight non-serious adverse events were reported by 26 participants (43%) with 39 events among 11 EUC participants and 59 events among 15 MCC+ participants. MCC+ participants experienced greater reductions in migraine days (−2.9 days for MCC+ vs. −1.0 days for EUC, difference = −1.9; 95% confidence interval: −3.5, −0.4).
Conclusions
Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of MCC+ for migraine.
Trial Registration
This study is registered at Clinicaltrials.gov (NCT03177616).
Introduction
Although medications are often used as first-line treatments for migraine, some patients experience intolerable side effects and may have increased risk for migraine chronification (1,2). As a result, individuals with migraine often express interest in holistic or integrative approaches over medication alone as part of a long-term management strategy (3). Integrative treatment approaches that address pathophysiologic processes involved in migraine attacks and/or reduce migraine symptoms have potential to reduce migraine frequency and severity.
Over 75% of migraine patients report associated neck pain and many note musculoskeletal complaints such as neck stiffness, muscle tension, or problems with jaw function (4–6). Emerging models of migraine pathophysiology suggest migraine-associated neck pain can be caused by triggering the trigeminocervical neural complex (7,8). Neck pain itself may also facilitate the onset of migraine attacks (9,10). Treatment options that address musculoskeletal complaints may represent viable therapeutic options for individuals with migraine.
A recent meta-analysis of clinical trials evaluating spinal manipulation reported small potential reductions in migraine frequency and pain intensity (11). However, the studies included in this meta-analysis did not evaluate multimodal chiropractic care, which includes spinal manipulation as well as joint mobilization, soft tissue release techniques, posture correction, relaxation techniques, education, and stretching (12,13). Other studies have suggested that massage therapy, physiotherapy, relaxation, manual trigger point therapy, and mindfulness may also be promising treatment approaches for migraine (14–16). Therefore, a multimodal chiropractic care approach, differentially applied based on individual characteristics, may result in larger reductions in migraine frequency and severity. However, no clinical trials have evaluated the ability of multimodal chiropractic care to reduce migraine frequency and severity.
The goal of this study was to conduct a pilot randomized controlled trial (RCT) evaluating multimodal chiropractic care + enhanced usual care (EUC) versus EUC alone for adult women with episodic migraine. Our primary aims were to assess feasibility of participant recruitment, retention and adherence to the protocol, and adverse events. As secondary outcomes, we explored changes in migraine frequency, severity, duration, and medication use between treatment groups.
Methods
Study population
The design of the Integrative Migraine Pain Alleviation through Chiropractic Therapy (IMPACT) study has been described in detail previously (17). The study was conducted at the Osher Clinical Center at Brigham and Women’s Hospital (Boston, MA). Participants were recruited through the Partners HealthCare system as well as online and newspaper postings. Inclusion criteria were: Female gender, age 20–55 years, diagnosis of episodic migraine with or without aura, ≥ 1 year of migraine, and experiencing 4–13 days with migraine during the run-in period. Exclusion criteria were: Having received chiropractic care in the past 3 months, any major systemic illness or unstable medical or psychiatric condition, history of stroke, carotid artery dissection, or vertebral artery dissection, head or neck trauma within the past year, diagnosis of medication overuse headache, new use of prophylactic medication for migraine headaches within the last three months, currently taking prophylactic migraine medications other than propranolol and topiramate, failure to complete daily migraine logs during the run-in period, having received Botox treatment for migraine in the past 6 months, self-reported current alcohol or substance abuse, and diagnosis of Ehler-Danlos syndrome. All participants were screened by the study neurologist (CB) to confirm their migraine diagnosis according to ICHD-3 criteria (18).
All participants signed a written informed consent document. This study was approved by the Brigham and Women’s Hospital Institutional Review Board and was prospectively registered (ClinicalTrials.gov identifier NCT03177616).
Study design
Our study consisted of a 4-week run-in period, followed by a 14-week intervention period, and then a 4-week post-intervention period. After a phone screen, potential participants attended an in-person screening visit with the study neurologist (CB). Eligible participants who provided informed consent then participated in a 4-week run-in period to confirm eligibility with respect to migraine frequency and compliance with completing daily migraine logs. After the run-in period, participants attended another study visit in which migraine logs were reviewed. Participants who completed their logs and recorded 4–13 migraine days during run-in completed additional baseline assessments and were randomized. Randomization was stratified by use of prophylactic migraine medication (no prophylactic medication use or prophylactic medication use) and by migraine frequency during the run-in period (4–7 migraines/month or 8–13 migraines/month). Randomization was performed using a computer generated random permuted block scheme with random block sizes and 1:1 allocation to multimodal chiropractic care intervention + EUC or EUC alone within each stratum. A study investigator (PMR) generated the allocation scheme and a study research assistant assigned the participant to the intervention. Study participants, research assistants, and chiropractors administering the intervention were not blinded to treatment assignment. Since this pilot study was not designed to test for efficacy, our goal was to randomize 60 participants to allow us to obtain estimates of recruitment and retention rates in preparation for a fully powered trial (19).
Throughout the study, participants completed daily migraine logs assessing migraine attacks including severity and duration of attacks and medication use. At randomization and the end of the intervention and post-intervention periods, participants completed questionnaires assessing migraine-related disability, health-related quality of life and psychosocial well-being.
Interventions
EUC was comprised of usual medical care as prescribed by the participants’ physicians as well as migraine education literature, which included information published by the American Headache Society on migraine pathophysiology, symptoms, and triggers, treatment approaches, and associations between migraine and sleep, sex, and cardiovascular disease (20–33). Individuals in the EUC group received bi-weekly phone calls from the study research assistant to minimize between-group differences in contact with the study team. EUC participants were also given the option of 10 courtesy chiropractic sessions following completion of the study to enhance recruitment and retention. Individuals assigned to chiropractic care + EUC received up to 10 sessions of chiropractic care over a 14-week period at the Osher Clinical Center by one of two chiropractors. The chiropractic care protocol has been described in detail previously (17). Briefly, the first chiropractic care visit included a physical examination assessing cervico-thoracic spine posture, ranges of motion, presence of myofascial trigger points, cervical and temporomandibular joint movement restrictions with a focus on myofascial contributions to cranial-facial pain, tenderness, hypersensitivity, muscle hypertonicity, and general muscular imbalances. Results of this examination were used to classify participants into diagnostic categories, each of which had pre-specified treatment approaches (Supplemental Table 1). The protocol was not rigidly standardized and instead could be customized to the patient’s clinical needs and preferences. Participants could opt out of any component of care, including spinal manipulation. All treatments applied in this study were within the scope of chiropractic practice in the Commonwealth of Massachusetts and included: posture correction and spinal stabilization exercises, soft tissue relaxation/release techniques, spinal manipulation and joint mobilization, relaxation techniques, education, stretches, and ergonomic modifications. Treatments provided were recorded in the participant’s medical record. After the end of the 14-week intervention phase, participants completed a 4-week post-intervention phase in which they did not receive chiropractic treatments or phone calls and only completed daily migraine logs.
Outcomes
In this pilot study, our primary outcomes evaluated feasibility of participant recruitment, retention and adherence to the protocol, and assessment of adverse events. Specifically, we aimed to demonstrate that 60 patients could be successfully recruited within 12 months, more than 85% would complete baseline and outcome assessments, and more than 85% of those in the chiropractic care + EUC group would attend 75% of the chiropractic care visits. We also hypothesized that there would be few and only minor adverse events reported related to the intervention. As part of our secondary aims, we also assessed changes in number of migraine days (our main clinical outcome (34)), migraine severity (1 to 10 scale), migraine duration (< 4 hours, 4–12 hours, or 13–24 hours), and number of acute migraine medications used. Means of these outcomes were calculated for the run-in period (baseline), weeks 11–14 of the intervention period (“initial follow-up”) and during the 4-week post-intervention phase (“final follow-up”) to use in the analysis. We also calculated the responder rate, defined as participants who had a ≥ 50% reduction in days with migraine from the run-in period to either the initial follow-up or final follow-up (34). Additional secondary outcomes included the evaluation of Migraine Disability Assessment (MIDAS) (35,36), Headache Impact Test (HIT-6) (37–39), and Migraine-Specific Quality of Life (40,41) domains.
All participants were given instructions at the start of the study to report any adverse event (AE) to study staff within 24 hours. Examples of AEs included acute events (e.g. a fall), chronic issues that worsen (e.g. chronic pain), side effects of treatment received (e.g. soreness), any painful or uncomfortable events that took place during or related to study visits, or any other changes that participants noticed about their health and/or safety during the study. Study staff also called participants in the chiropractic care + EUC group once a month and participants in the EUC alone group every 2 weeks to inquire about the occurrence of AEs.
Statistical methods and analysis
Using the number of participants in a given treatment group as our denominator, we calculated the treatment-specific frequency of completion of outcome assessments. For each participant in the chiropractic care + EUC group, we calculated the proportion of attended treatment visits and determined the percentage of individuals who completed at least 75% of them. We tabulated AEs for each treatment group by organ system and classified each AE with its degree of relatedness to the intervention (unrelated, possibly related, related).
We estimated the effect of treatment assignment on number of migraine days in each outcome assessment (run-in, initial follow-up, final follow-up) using a linear mixed-effects model imposing a shared baseline assumption and assuming an unstructured covariance structure (42). All models were performed using an intention-to-treat analysis and adjusted for age at randomization (centered at mean age) and strata. Estimates are reported as adjusted means and adjusted difference in means with 95% confidence intervals for the changes from run-in to both follow-up periods. An equivalent model and analytic approach were used for our other secondary outcomes. We also estimated effects on our primary clinical outcome by number of migraine days during run-in (4–7 versus 8–13 migraine days).
For our primary clinical outcome of migraine days, we calculated the proportion of participants experiencing a ≥ 50% reduction in the number of migraine days between baseline and the initial or final follow-up and estimated effects with logistic regression adjusting for age.
Analyses were conducted using SAS (version 9.4; SAS institute Inc., Cary, NC).
Results
The study flow is described in Figure 1. Of the 422 individuals who completed the phone screen, 84 provided consent and entered the 4-week run-in period. Seventy individuals attended the final screening visit and 61 were randomized (29 to chiropractic care + EUC and 32 to EUC alone). The recruitment period lasted 20 months (13 July 2017 through 28 March 2019).
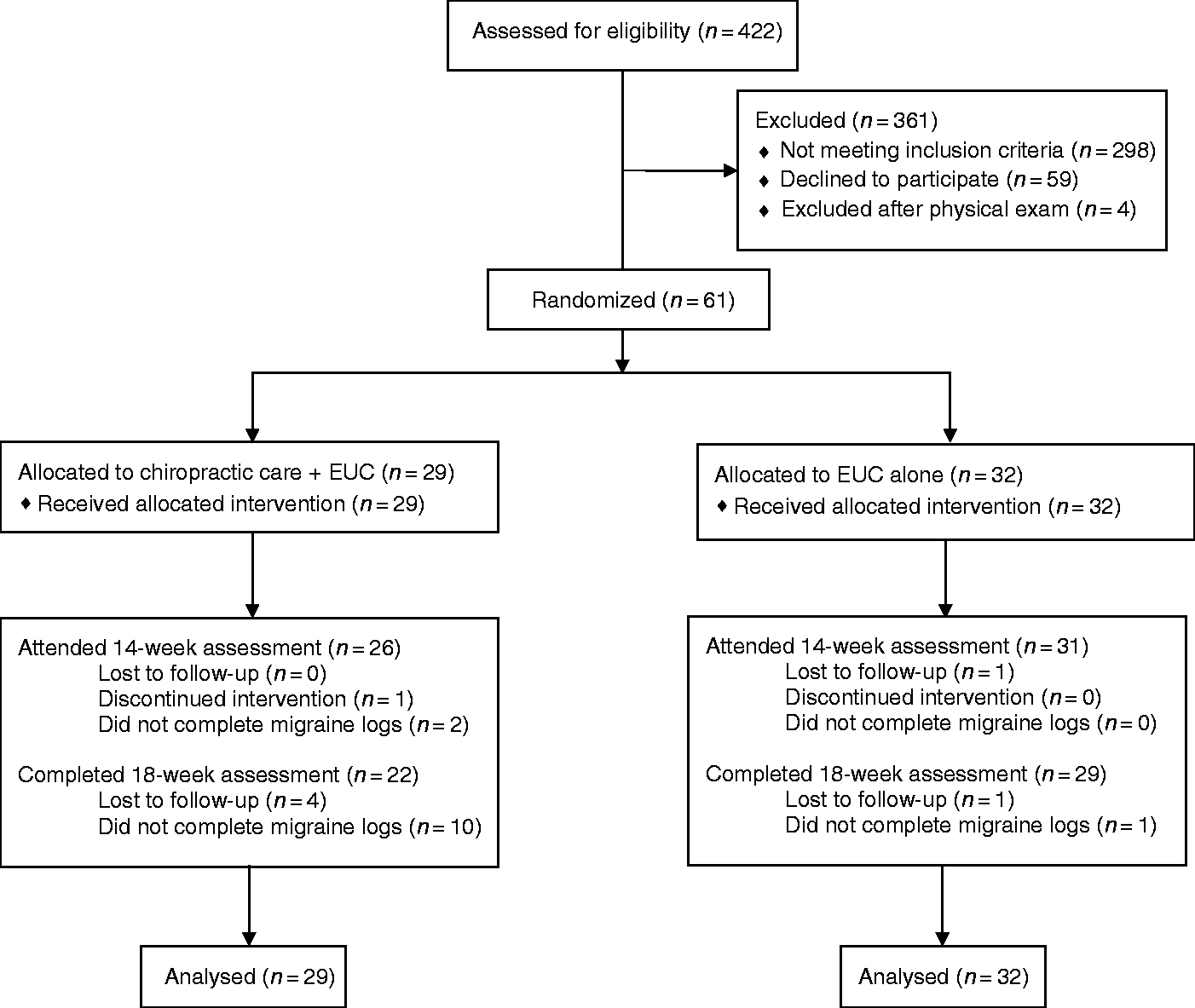
Study flow diagram.
Mean age of the women included in this study was 36.4 years (range: 21–55 years) and mean migraine frequency during run-in was 7.6 migraine days (standard deviation (SD) = 2.2). Six women were taking prophylactic medications. Baseline characteristics were similar between the two treatment groups (Table 1).
Baseline characteristics of the study participants by randomized treatment assignment (n = 61).

Note: Migraine duration was assessed in the following categories: < 4 hours (coded as 2 hours), 4–12 hours (coded as 8 hours), and 13–24 hours (coded as 18 hours)
EUC: enhanced usual care; IQR: interquartile range.
Of the 61 participants randomized, 59 (97%) attended the 14-week follow-up visit, and 51 (84%) returned the 18-week follow-up questionnaires. Fifty-seven participants (93%) completed the 14-week migraine logs (26 in the chiropractic care + EUC group and 31 in the EUC only group), and 51 (84%) completed the 18-week migraine logs (22 in the chiropractic care + EUC group and 29 in the EUC only group) (Figure 1). Forty-five participants (74%) completed all baseline and outcome assessments.
Each participant in the chiropractic care + EUC group was eligible to receive 10 sessions for a total of 290 possible sessions, of which 264 were attended (91%). Of the 29 individuals in the chiropractic care + EUC group, 24 individuals (83%) attended at least 75% of the chiropractic sessions. Additional information about the frequency of treatment modalities used across all visits is provided in Supplemental Table 2.
No serious AEs were reported. We observed 98 non-serious AEs (39 events among 11 participants in the EUC group and 59 events among 15 participants in the chiropractic care + EUC group). In the chiropractic care + EUC group, 15 events among four participants were possibly related to the intervention and five events among five participants were related to the intervention. These events usually involved musculoskeletal stiffness or migraine. No possibly related or related AEs were reported in the EUC alone group. Table 2 summarizes the overall number of AEs and the most common types of AEs according to their MedDRA system organ class and preferred term. The percentages of individuals reporting the various types of AEs was similar across the two treatment groups, with the exception that those in the chiropractic care + EUC group were more likely to report musculoskeletal stiffness (21% of participants) compared to those in the EUC alone group (6% of participants).
Adverse events by randomized treatment assignment according MedDRA system organ class and preferred term.

Our regression model estimated the change within and between treatment groups at both follow-up periods (Table 3). Those in the chiropractic care + EUC group experienced a greater change in number of days with migraine from run-in to the initial follow-up (weeks 11–14) (mean change = −2.90, 95% CI: −4.04, −1.76) compared to those in the EUC alone group (mean change = −0.98; 95% CI: −2.03, 0.06) (between-group difference in mean change = −1.92; 95% CI: −3.46, −0.37). This effect persisted at final follow-up. Compared to EUC alone, chiropractic care + EUC resulted in greater reductions in migraine severity (between group difference in mean change = −0.85; 95% CI: −1.77, 0.06), number of acute medications used (between-group difference in mean change = −1.36; 95% CI: −3.48, 0.76), and migraine duration (between group difference in mean change = −1.48; 95% CI: −3.44, 0.48) from baseline to initial follow-up. Effects were slightly attenuated at final follow-up with the exception of migraine duration, where there was no effect of chiropractic care + EUC compared to EUC alone.
Effect of randomized treatment assignment on change within groups and change between groups from run-in to both follow-up time periods (n = 61).
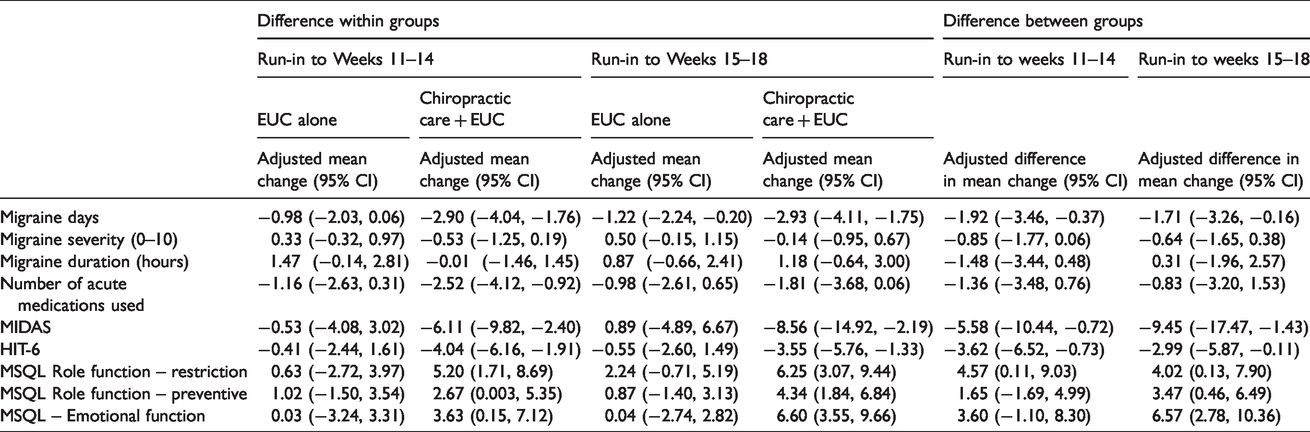
For our additional secondary outcomes, those in the chiropractic care + EUC group had larger decreases in their scores on the MIDAS from run-in to week 14 (between-group difference in mean change = −5.58 (95% CI: −10.44, −0.72)) and HIT-6 (between group difference in mean change = −3.62 (95% CI: −6.52, −0.73)) than those in the EUC alone group (Table 3). Patients in the chiropractic care + EUC group also experienced larger improvements in MQSL scores from run-in to week 14 than those in the EUC alone group although the magnitude of the between-group differences was small (Table 3).
For our primary clinical outcome of migraine days, we observed slightly larger effects of chiropractic care + EUC compared to EUC alone among those reporting four to seven migraine days during run-in (between group difference in change = −2.04 (95% CI: −4.24, 0.14)) than among those reporting eight to 13 migraine days during run-in (between group difference in change = −1.78 (95% CI: −4.04, 0.47)).
At the initial follow-up, 10 women in the chiropractic care + EUC group and seven women in the EUC alone group were considered responders. Chiropractic care + EUC was associated with a twofold increase in the odds of being a responder, although confidence intervals were wide (OR = 2.17, 95% CI: 0.68, 6.95). Similar results were seen at the final follow-up (11 responders in the chiropractic care + EUC group and eight responders in the EUC alone group; OR = 2.59, 95% CI: 0.80, 8.36).
Discussion
In this pilot study, pre-specific feasibility criteria were not met, but the deficits were remediable. Recruitment was slower than planned. The most common recruitment sources were self-referrals of individuals who learned about the study from a searchable database of ongoing studies within the Partners HealthCare system and referrals from the study neurologist. This suggests that future trials can enhance recruitment by additional advertising of the study and by partnering with additional healthcare providers. Most loss to follow-up occurred during the final follow-up period after the end of the intervention. Compliance with completion of migraine logs, the presumptive primary outcome of a future trial, was 94% at initial follow-up and 84% at final follow-up, although only 74% of participants completed all outcome assessments. Future trials could enhance retention and compliance with data collection by focusing outcome assessment to fewer questionnaires and using electronic data collection methods that alert participants if they skip questions. Compliance with treatment was slightly lower than expected (83% of those in the chiropractic care + EUC group attended at least 75% of the chiropractic visits versus our goal of 85%). Future trials in this population could enhance treatment compliance by increasing the numbers and locations of providers, which would increase the ease of scheduling appointments.
For our primary clinical outcome of change in migraine days, we observed a mean decrease of ∼3 migraine days per month for those randomized to the chiropractic care + EUC compared to a mean decrease of ∼1 migraine day per month for those randomized to EUC alone. This difference in mean change between the two groups may be clinically meaningful since it is comparable to the effect size seen for topiramate, propranolol, or erenumab compared to placebo, which is a decrease of about 2 days per month (43–45). However, larger-scale studies are needed to determine the efficacy of chiropractic care for migraine. We observed some evidence of clinically meaningful changes in HIT-6 scores, MSQL role function-restriction, and potentially MIDAS scores for those randomized to chiropractic care + EUC (46–48). However, effects of chiropractic care + EUC on migraine severity, migraine duration, number of medications used, and MQSL role function – preventive and emotional function were not clinically meaningful (48).
Some evidence suggests that spinal manipulation may result in modest reductions in migraine frequency and pain intensity; however, most studies are small and have significant methodological limitations (11). In this pilot, we addressed methodologic limitations of some prior studies by describing and using a rigorous randomization approach, reporting on compliance and attrition, and specifying primary clinical outcomes. Although we did not use a “sham” control like some prior studies, we did provide participants in the comparison group with educational materials and contacted them bi-weekly to lessen between-group differences in personal contact with the study team.
An important limitation to prior studies is that they only evaluated one component of chiropractic care – spinal manipulation (49–54). In clinical practice in the US, chiropractic care is typically delivered in a multimodal manner and we hypothesized that this multimodal approach may result in larger beneficial effects than spinal manipulation alone. Our preliminary findings support the promise of this approach. Chiropractic evaluation sought to identify one or more of three diagnostic classifications: myofascial pain syndrome; postural or mechanical spinal disorders; and temporomandibular dysfunction. Treatment was individually tailored to address major elements of the diagnostic categories. The chiropractic care protocol used in the study was validated by a diverse team of chiropractic experts using a Delphi method (17) to ensure that it was evidence-based and representative of clinical management within the scope of chiropractic practice across the US. The protocol targeted diagnosis and treatment of musculoskeletal symptoms and sequelae, but was flexible enough to account for variability in presentation and patient preferences (17).
Another important aspect of this study was monitoring of AEs in both the EUC alone and chiropractic care + EUC groups. Reporting and monitoring of AEs in non-pharmacological intervention studies is often inconsistent but is essential to understanding the risk-benefit balance of these interventions. In this study, participants were instructed to contact study staff if they experienced any AEs. In addition, during phone calls, participants in both groups were asked open-ended questions about change in symptoms as well as directed questions about the presence of symptoms listed on the informed consent form. All reported AEs were non-serious and usually involved musculoskeletal stiffness or changes in migraine symptoms (i.e. nausea). Prior literature suggests that the type and number of AEs (e.g. local soreness) observed in this study are consistent with other trials using similar treatments and with what is currently known about manual therapies, postural correction exercises, stretching, and home exercise treatments (55–57).
These results are similar to a prior study on spinal manipulation among migraineurs (50). However, overall sample sizes of both this and our study are small and may not have sufficient numbers to detect rare AEs. For example, some studies have reported associations between chiropractic care and cervical artery dissection, a rare but serious event (58–64). However, the causal nature of this relationship has not been established and is questioned by other studies, which have reported associations between cervical artery dissection and primary care practitioner visits (65–68) and biomechanical studies which demonstrated that cervical manipulation causes significantly less arterial strain than normal range of motion (68–70). Regardless, all participants were informed of potential AEs including cervical artery dissection during the informed consent process and during discussions with the chiropractor on types of cervical manipulation (17).
Although this study has strengths, including evaluation of an expert-validated multimodal chiropractic care protocol, rigorous assessment of AEs, use of migraine logs to assess outcomes, and randomized treatment assignment, some important limitations should be noted. Since this was a pilot study, we were unable to test for efficacy and estimates of AEs are preliminary. Also, we were unable to blind participants to their treatment assignment, which is a typical limitation in trials of manual therapy. This lack of blinding may have resulted in more patients in the chiropractic care + EUC group reporting larger benefits of treatment than those in the EUC group. Participants in the EUC group also received less patient contact than those in the chiropractic care + EUC group and it is plausible that some differences in clinical outcome measures could be driven by differences in patient contact.
Although results from this study suggest chiropractic care may serve a role in migraine management, several unanswered questions remain. Given the proposed links between migraine and neck pain, future studies should explore interactions between chiropractic care, neck pain, and migraine days. Future research should also explore different “doses” of chiropractic care (i.e. additional treatments or different treatment frequency) given recent observations of an inverse linear relationship between spinal manipulation treatments and cerviogenic headache days (71). These studies would inform the design of a large-scale efficacy trial of multimodal chiropractic care for migraine.
Clinical implications
Spinal manipulation may reduce migraine frequency, but effects of multimodal chiropractic care on migraine frequency has not been evaluated. We conducted a pilot randomized controlled trial comparing multimodal chiropractic care plus enhanced usual care versus enhanced usual care alone among adult women with episodic migraine. Pre-specified feasibility criteria were not met, but deficits were remediable. Preliminary data support a definitive trial of multimodal chiropractic care for migraine.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420963844 - Supplemental material for Multimodal chiropractic care for migraine: A pilot randomized controlled trial
Supplemental material, sj-pdf-1-cep-10.1177_0333102420963844 for Multimodal chiropractic care for migraine: A pilot randomized controlled trial by Pamela M Rist, Carolyn Bernstein, Matthew Kowalski, Kamila Osypiuk, Julie P Connor, Robert Vining, Cynthia R Long, Eric A Macklin and Peter M Wayne in Cephalalgia
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PMR reports no conflicts of interest to disclose. CB has served as a consultant for Amgen and Percept. MK has received Board of Directors fees from NCMIC, Inc. and sits on the advisory board of the NCMIC Foundation. KO, JPC, RV and CRL report no conflicts of interest to disclose.
EAM served as a DSMB member for Novartis Pharmaceuticals and Shire Human Genetic Therapies, served on an advisory committee for Biogen, consulted for Cerevance, Intrance, Inventram, Lavin Consulting, and Myolex, and his institution received grants on his behalf from Amylyx Pharmaceuticals, GlaxoSmithKline, and Mitsubishi Tanabe Pharmaceuticals. PMW has received funding from the NCMIC Foundation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by a grant from the Osher Center for Integrative Medicine; the NCMIC foundation; Inter-Institutional Network for Chiropractic Research (IINCR) through Palmer College Foundation; the Crimson Lion Foundation, Jeannie and Jonathan S Lavine, Trustees; and National Institutes of Health grants K24AT009282 and K01HL128791.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.