
Abstract
To evaluate whether NC could be demonstrated preoperatively, high-resolution magnetic resonance angiography (MRA) was performed in 287 consecutive patients with TN and persistent idiopathic facial pain (PIFP) on a 0.5-T and a 1-T MR unit. Depending on the clinical symptoms, the TN cases were divided into typical TN and trigeminal neuralgia with non-neuralgic interparoxysmal pain (TNWIP) groups. Microvascular decompression (MVD) was performed in 103 of the MRA-positive cases. The patients were followed up postoperatively for from 1 to 10 years. The clinical symptoms were compared with the imaging results. The value of MRA was assessed on the basis of the clinical symptoms and surgical findings. The outcome of MVD was graded as excellent, good or poor. The clinical symptoms were compared with the type of vascular compression and the outcome of MVD. The MRA image was positive in 161 (56%) of the 287 cases. There were significant differences between the clinical groups: 66.5% of the typical TN group, 47.5% of the TNWIP group and 3.4% of the PIFP group were positive. The quality of the MR unit significantly determined the ratio of positive/negative MRA results. The surgical findings corresponded with the MRA images. Six patients from the MRA-negative group were operated on for selective rhizotomy and no NC was found. Venous compression of the trigeminal nerve was observed in a significantly higher proportion in the background of TNWIP than in that of typical TN on MRA imaging (24.1% and 0.8%, respectively) and also during MVD (31.2% and 1.2%, respectively). Four years following the MVD, 69% of the patients gave an excellent, 23% a good and 8% a poor result. The rate of some kind of recurrence of pain was 20% in the typical TN and 44% in TNWIP group. The rate of recurrence was 57% when pure venous compression was present. The only patient who was operated on from the PIFP group did not react to the MVD. The clinical symptoms and preoperative MRA performed by at least a 1-T MR unit furnish considerable information, which can play a role in the planning of the treatment of TN.
Introduction
In the treatment of classical trigeminal neuralgia (TN), neurovascular decompression operations are performed on the basis of the observations made by Dandy (1) and published in the American Journal of Surgery in 1934. The first microvascular decompression (MVD) was carried out by Gardner in 1966 (2), and the work of Jannetta (3–5) led to this procedure becoming an accepted mode of treatment for TN.
In Hungary, the first MVD was accomplished by Mérei with the active assistance of Jannetta in 1973. From that time on up to 1989, only a few MVDs were effected in the country, until our team started to use this method regularly to treat TN (6). In the first 6 years, only computed tomography (CT) and later magnetic resonance imaging (MRI) were available to rule out the symptomatic TN cases, but the need to demonstrate the neurovascular compression (NC) preoperatively emerged when we found no vessels in contact with the nerve in approximately 20% of the cases at operation.
Since 1994, we have had the opportunity to investigate our patients with TN with three-dimensional time-of-flight MR angiography (3D TOF MRA). The method allows us to evaluate preoperatively the relationship between the trigeminal nerve and the vascular structures. Since then, a positive result of 3D TOF MRA has been mandatory in the indication of MVD.
Our aims in the present study were to assess:
the relation between three facial pain groups (typical TN and TN with non-neuralgic interparoxysmal pain (TNWIP) and persistent idiopathic facial pain (PIFP)) and the MRA findings;
the value of MRA as indicated by the clinical symptoms and surgical findings; and
the correlation between the clinical symptoms, type of vascular compression and the outcome of MVD.
Patients and methods
3D TOF MRA was performed in 287 patients with typical TN (n = 197, 68.6%), TNWIP (n = 61, 21.2%) or PIFP (n = 29, 10.1%). Symptomatic TN cases where a causative lesion, other than vascular compression (e.g. tumour, arteriovenous malformation, multiple sclerosis, etc.), had been demonstrated by special investigations (CT, MRI) were excluded. The three clinical groups were created in accordance with the International Classification of Headache Disorders. The ‘classical TN’ group was divided into two subgroups. The third group involved PIFP, previously known as atypical facial pain. The characteristics of the three clinical groups are as follows (7):
Typical TN: paroxysmal attacks of pain lasting from a fraction of a second to 2 min, affecting one or more divisions of the trigeminal nerve. The pain is intense, sharp, superficial or stabbing and/or precipitated from trigger areas or by trigger factors. Attacks are stereotyped in the individual patients. There is no clinically evident neurology deficit. TN is not attributed to another disorder. The pain never crosses to the opposite side, but it may rarely occur bilaterally. Following a painful paroxysm, there is usually a refractory period during which pain cannot be triggered. The TN is usually responsive, at least initially, to pharmacotherapy.
TNWIP (also known as atypical TN): the same as above, but there is a dull background pain.
PIFP: pain in the face, present daily and persisting for all or most of the day. Pain is confined at onset to a limited area on one side of the face, and is deep and poorly localized. Pain is not associated with sensory loss or other physical signs.
The 3D TOF MRA investigations were made on two different MR units: a 0.5-T Elscint Gyrex VD1x and a 1-T Signa Horizon LX. On the 0.5-T equipment, the examination data were: echo time 9 ms, repetition time 33–38 ms, flip angle 25, slice thickness 1–1.5 mm, volume thickness 30–50 mm. Maximum intensity projections (MIP) in three standard planes (coronal, sagittal and axial) were focused on the nerve root entry zone of both trigeminal nerves. The thin-slice (1 voxel thick) reconstructed images were used to clarify the fine anatomical relationship of the nerve and the vessels. On the 1-T equipment, the following parameters were used: echo time minimal, repetition time 33 ms, flip angle 20, slice thickness 1 mm, volume thickness 70 mm. In postprocessing procedures, MIP, volume rendering and (sometimes) virtual endoscopy were carried out. All measurements were repeated (on both the 0.5-T and the 1-T equipment) after the intravenous administration of gadolinium (0.1 mmol/kg) to visualize the veins. The MRA performed without contrast material visualizes the arteries, while with contrast material the veins can also be seen. In a further method, the anatomical situation can be assessed on the thick slices during postprocession and arteries can be distinguished from veins according to their course.
NC was predicted if distortion (either longitudinal bending or cross-sectional deformation or both) of a nerve, caused by a vessel, was observed in the MRA images, or there was no visible gap between the trigeminal nerve and the vessel (close contact). The whole cisternal part of the trigeminal nerve was evaluated. NC was diagnosed if these findings were detected in either the source images or the reconstructed images (8–12).
In this study, 172 patients were investigated with the 0.5-T MR unit and 115 patients with the 1-T MR unit.
MVD was considered only in those cases where NC was detected in the MR angiogram in accordance with the symptoms and the medical treatment failed. Usually, patients were treated with carbamazepine up to 1000 mg daily or with clonazepam up to 8 mg daily, and recently with gabapentin up to 1800 mg daily as basic treatment. If the monotherapy was not satisfactory, phenytoin up to 300 mg daily and/or Baclofen up to 30 mg daily was given. When this pharmacotherapy was not enough to control the paroxysms or there was some side-effect or intolerance to the treatment (even at a low dose), it was classified as failed medical treatment. In a few cases, patients refused to take any medication or after a few weeks tired of taking tablets regularly and asked for surgical treatment. MVD was offered if the patient was judged to be suitable for general anaesthesia and accepted posterior cranial fossa exploration.
All patients who met the criteria were enrolled in the surgical study between January 1994 and December 2003. MVD was performed in 103 cases in 101 patients (two patients had bilateral TN and MVD).
The MVD was performed according to Jannetta (5), and a piece of gelatin foam (Gelfoam, Spongostan) was interpositioned between the vessels and nerves. In some venous compression cases, the veins were coagulated and dissected. Most of the operations were performed by two surgeons, but a few patients of other surgeons’ were also included in the study.
From the MRA-negative group, six patients who had previously been treated by glycerol rhizotomy several times, but in whom the period up to the recurrent pain became progressively shorter, were operated on by selective trigeminal rhizotomy.
Data collection
The clinical symptoms, MRA findings and surgical observations were recorded. The surgical outcome was assessed 1 week, 6 months, and 1, 2, 4, 6, 8 and 10 years postoperatively. Patients were encouraged to present to be followed up clinically at any time when they felt any deterioration. The first two follow-ups were clinical, whereas the later ones involved letter questionnaires. The outcome regarding the facial pain was graded into six groups: 1, without pain; 2, almost without pain; 3, significantly less pain; 4, moderately less pain; 5, no change; 6, worse.
The patients additionally had to respond to questions concerning whether they took any medication and whether they would suggest MVD to relatives or friends if they had TN. The classification of the results is shown in Table 1.
Outcome measures
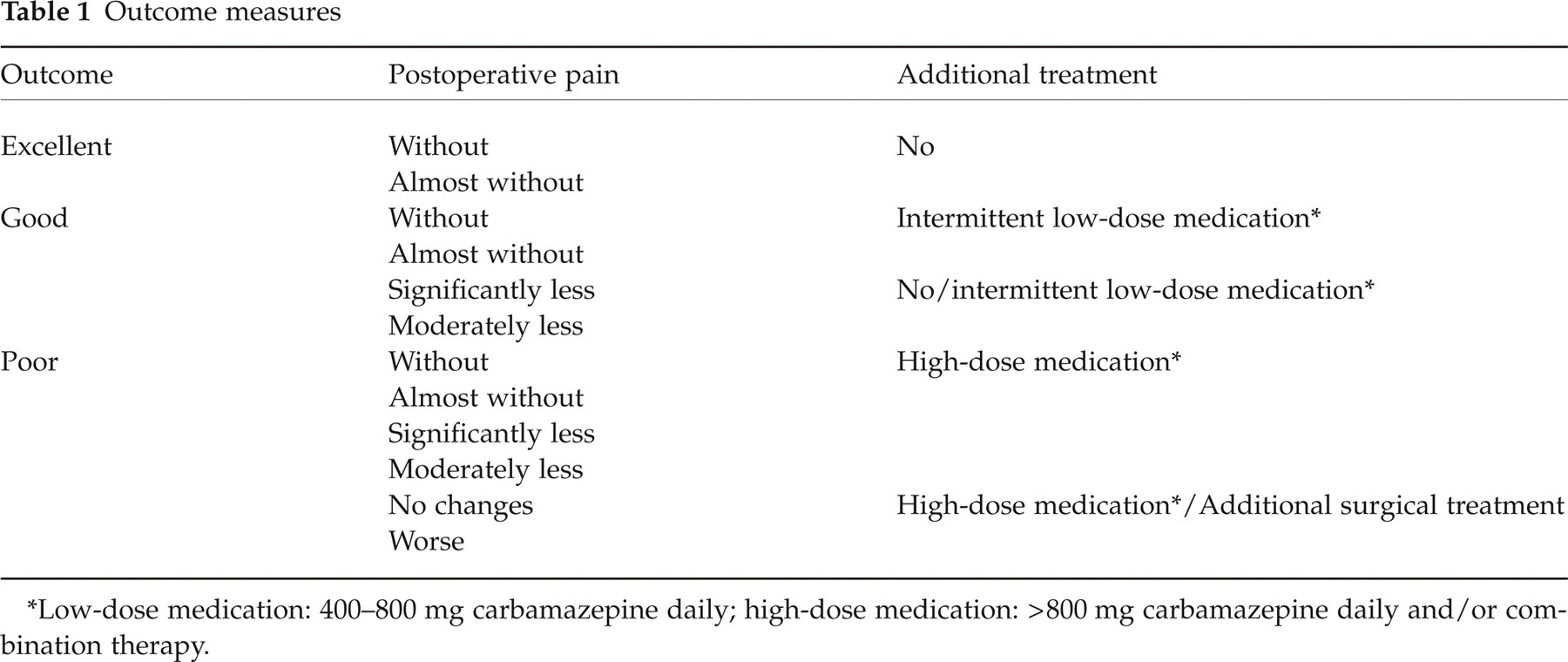
Low-dose medication: 400–800 mg carbamazepine daily; high-dose medication: >800 mg carbamazepine daily and/or combination therapy.
The recurrence was classified as moderate, which corresponds to the criteria of a good outcome, or as severe, which corresponds to the criteria of a poor outcome.
For the purposes of the analysis, patients who underwent bilateral MVD were counted twice (once for each side).
Statistics
The results were analysed by χ2 tests, using SPSS 11.0 software (SPSS Inc., Chicago, IL, USA). In the cases of 2 × 2 crosstabs, Fischer's exact test (FET) (two-sided) was applied. For the analysis of successful outcomes, Kaplan–Meier analysis was performed. Differences were considered statistically significant when P < 0.05.
Results
Clinical symptoms and 3D TOF MRA images
From among the 287 patients with facial pain who underwent 3D TOF MRA, the result was positive in 161 cases (56%) and negative in 122 cases (44%). In the MRA-positive group, there were 131 typical TN cases (81.3%), 29 TNWIP cases (18%) and one PIFP case (0.6%). In the TN cases (both typical TN and TNWIP), there were positive MRA results on the asymptomatic side in 27 cases (10.4%). The sensitivity of MRA performed on TN patients was 62%, while the specificity was 90%, with the contralateral (asymptomatic) side taken as reference.
The distribution of the 3D TOF MRA results with respect to the clinical symptoms revealed a significantly higher positive rate in the typical TN group than in the TNWIP group (66.5% vs. 47.5%, FET, P < 0.01). In the PIFP group, there was only one (3.4%) MRA-positive case (Table 2).
Distribution of the magnetic resonance angiography (MRA) results in the three clinical groups

TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
There was a great difference between the proportions of the MRA-positive and -negative cases, depending on which MR unit was used in the diagnostic procedure (Table 3).
Sensitivities of the different magnetic resonance (MR) units in the three clinical groups
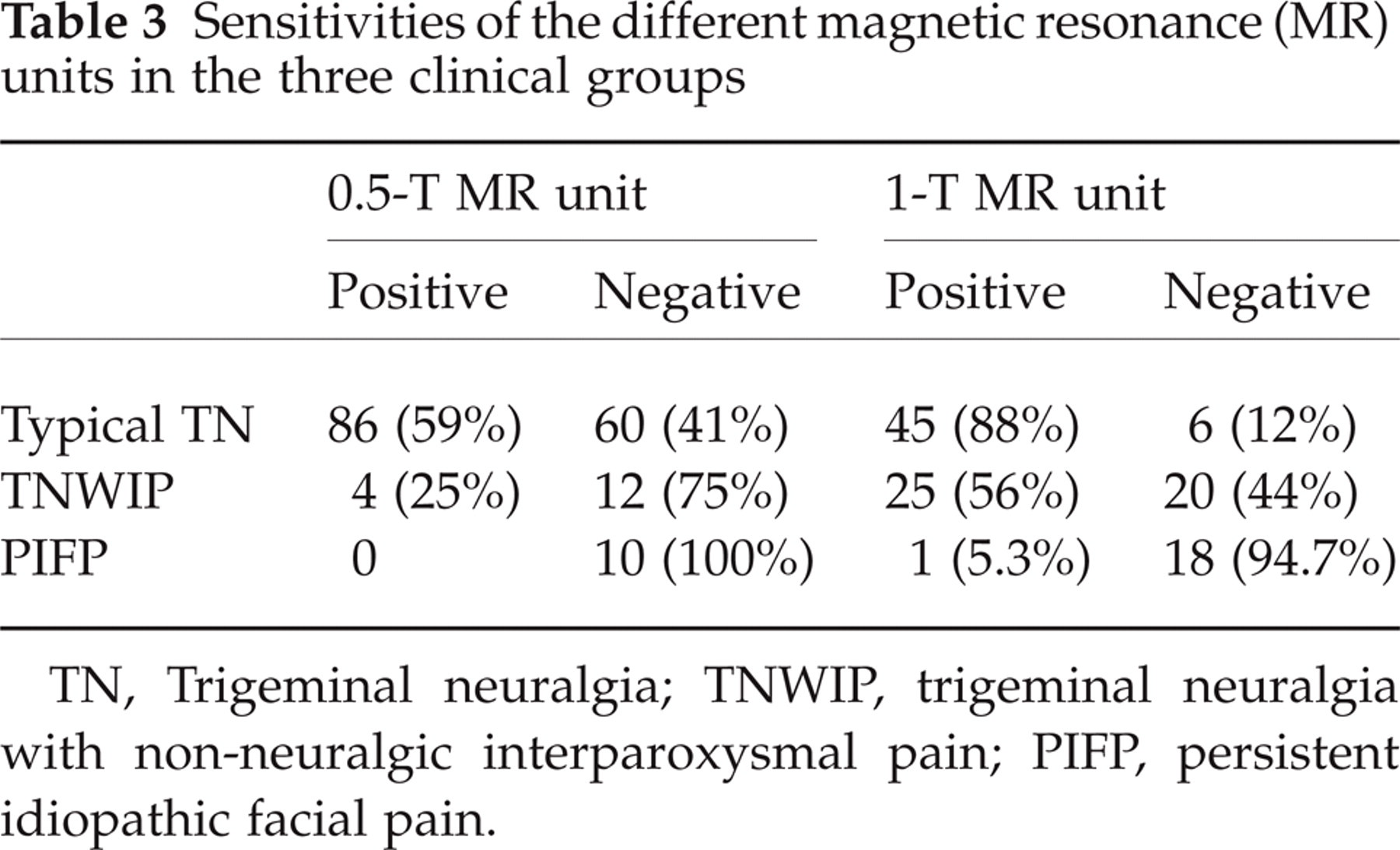
TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
The types of NC seen on MRA in the three clinical groups are listed in Table 4. In the typical TN group, the rate of arterial compression was much higher (90%) than that in the TNWIP group (51.7%), whereas venous compression was seen more frequently in the TNWIP group (24.1%) than in the typical TN group (0.8%) (FET, P < 0.001).
Types of neurovascular compression (NC) seen on magnetic resonance angiography in the clinical groups
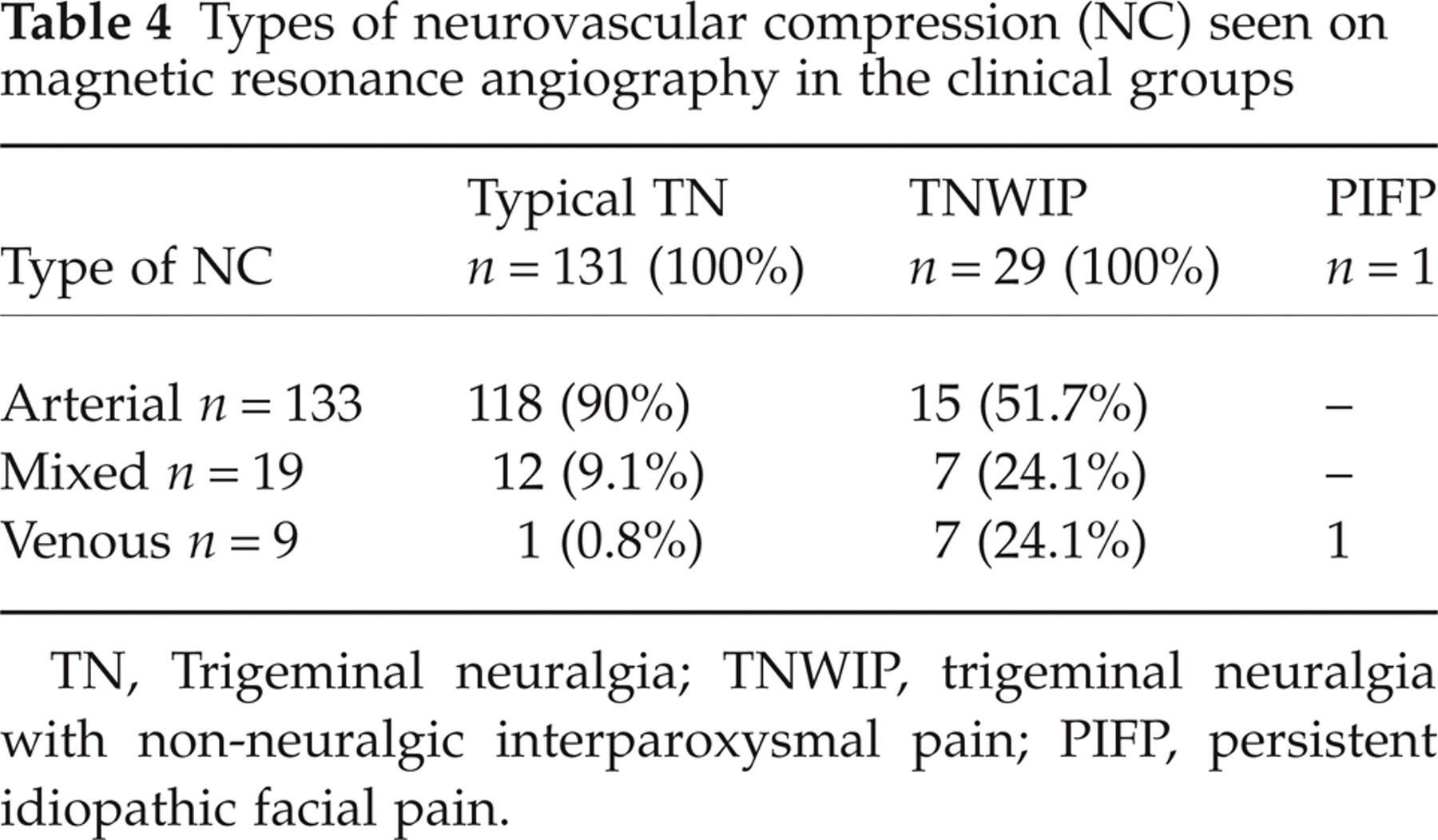
TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
Comparison of 3D TOF MRA images and intraoperative observations
Between January 1994 and December 2003, 99 patients underwent unilateral MVD and two patients underwent bilateral MVD. The general characteristics of the patients are presented in Table 5.
General characteristics of the 101 operated patients

All these patients were treated with a minor ablative surgical method.
TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
In the 101 patients and 103 cases, we could always identify NC on MRA (which was mandatory for the MVD in this series). The 0.5-T MR unit was used in 56 cases, and the 1-T MR unit was used in 47 cases to demonstrate the NC. During surgery, NC was observed in 97 cases (94.1%), while in six cases (5.9%) we could find a loose contact, when an artery was running on the nerve, but there was no distortion of the nerve, or there was a visible gap between the nerve and the artery and the vessel touched the nerve periodically, only in the systolic phase. This loose contact could be seen in three cases in the group where the 0.5-T unit was used, and also in three cases where the 1-T MR unit was used.
When the 0.5-T MR unit was used, in three cases the NC seemed to be arterial on MRA, but proved venous during surgery. Re-evaluation of the MRA scans of these patients postoperatively led to the identification of veins instead of the superior cerebellar artery. (This was the fault of the initial evaluation, but not of the method.) In the remaining 100 cases (97.1%), the MRA findings corresponded to the surgical observations. In 96 (93.2%) cases, the compression was arterial (87 pure arterial and nine mixed arterial + venous); only in seven cases (6.8%) was pure venous compression found (Table 6).
Vessels causing neurovascular compression (surgical observations, n = 103)

In the six patients operated on from the MRA-negative group (three patients were investigated with the 0.5-T and three with the 1-T MR unit) in whom open craniotomy was carried out for selective rhizotomy, no NC of the trigeminal nerves was observed during surgery.
As regards the surgical findings, the rate of arterial NC was significantly higher in the typical TN group (90.6%) than in the TNWIP group (56.2%). Pure venous compression was found frequently (31.2%) in the TNWIP group, whereas it was rare (1.2%) in the typical TN group (FET, P < 0.0001) (Table 7).
Type of neurovascular compression (NC) in respect of the clinical symptoms (surgical findings)
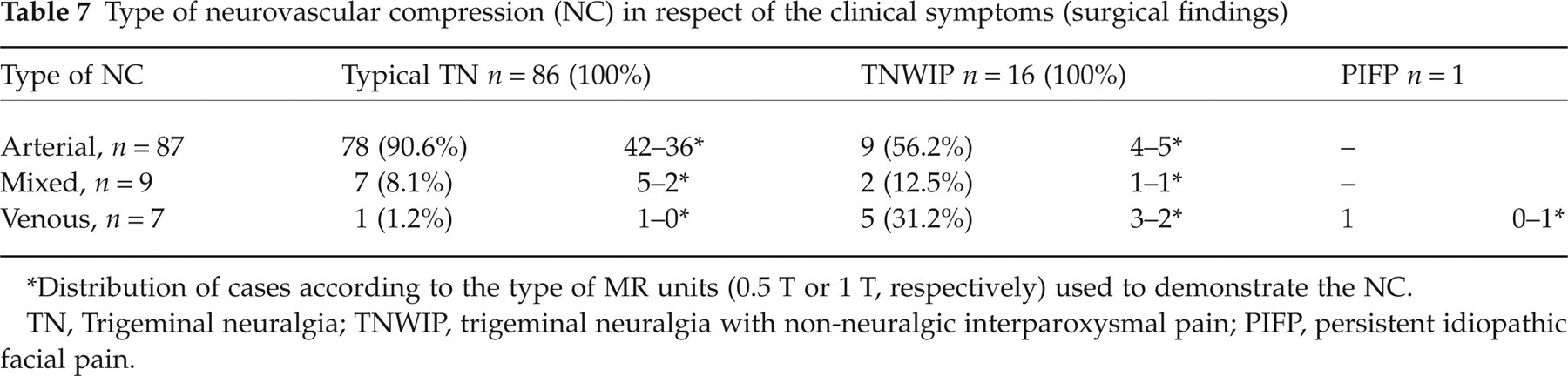
Distribution of cases according to the type of MR units (0.5 T or 1 T, respectively) used to demonstrate the NC.
TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
Outcome after microvascular decompression
The median length of follow-up for the 101 patients (103 cases) was 43.6 months. One patient died from cardiac failure 3 weeks postoperatively; seven other patients (7%) were lost to follow-up, one after 1 year, four after 2 years and two after 4 years.
The immediate postoperative relief from tic and facial pain was complete in 90%, partial in 5% and absent in 5%. Six months after MVD, 89% gave excellent, 5% good and 6% poor results. One year after MVD, 80% gave excellent, 12% good and 8% poor results. Four years after the procedure, 69% of the patients gave excellent, 23% good and 8% poor results (Table 8, Fig. 1).
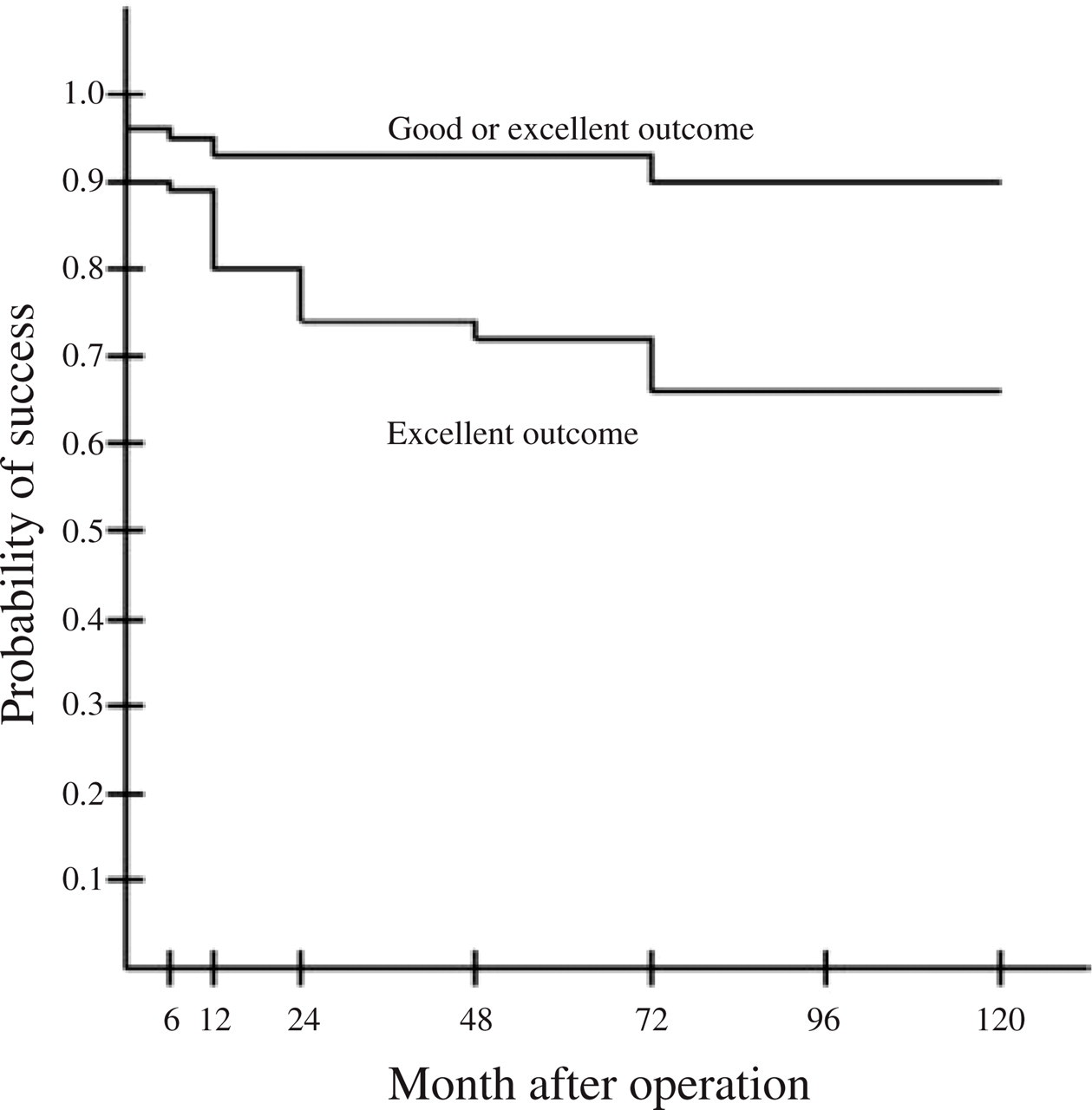
Kaplan–Meier analysis of the success of microvascular decompression (MVD). The curves show the proportions of patients with successful outcomes after MVD for all 103 cases.
Distribution of outcome after given follow-up periods

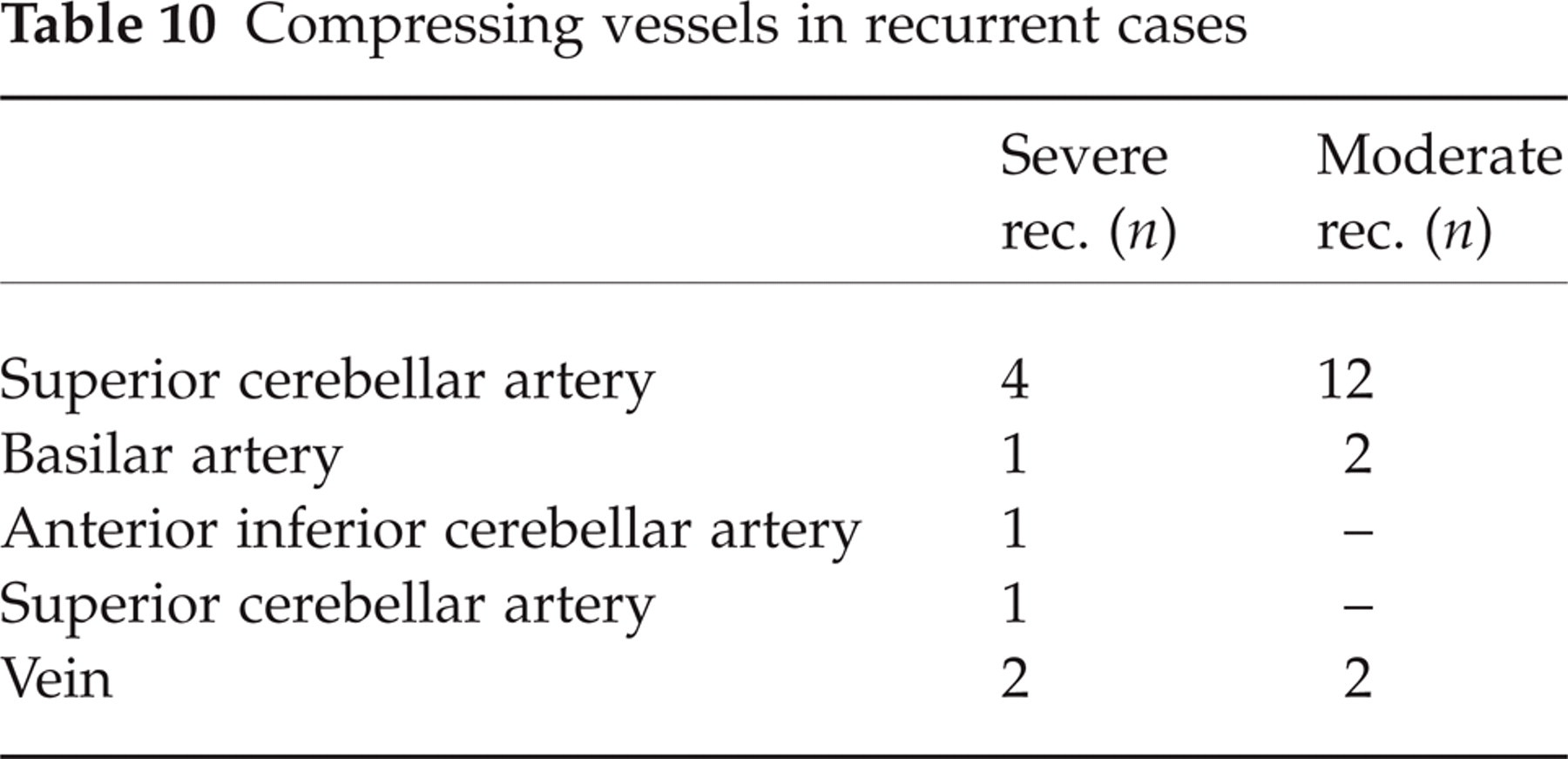
Most of the recurrences, either severe or moderate, appeared within 1 year following MVD. In only one case did the recurrent tic appear 6 years following MVD; in this case, the basilar artery was the compressing vessel (Tables 9 and 10).
Time of onset of recurrence and its severity

Compressing vessels in recurrent cases
One patient, who experienced moderate recurrence 6 months after MVD, suffered a severe recurrence 1 year later. Altogether, 25 patients had some kind of recurrence. From among the nine severe recurrent cases, one patient was treated with selective rhizotomy, one with stereotactic thalamotomy and three with glycerol rhizotomy; the remaining recurrent cases resumed taking medication.
The distribution of the compressing vessels in the cases in which recurrence appeared is to be seen in Table 10.
While the rate of some kind of recurrence among the typical TN cases was only 20%, among the TNWIP cases it was 44% (approaches significance, FET, P = 0.054) (Table 11).
Onset of recurrence in the different clinical symptoms

TN, Trigeminal neuralgia; TNWIP, trigeminal neuralgia with non-neuralgic interparoxysmal pain; PIFP, persistent idiopathic facial pain.
The patients’ assessments of MVD
Five of the patients would not recommend MVD in the future. All of them belonged in the group who complained of immediate recurrence of the pain. Three patients did not answer this question. All three gave a poor final result. One patient died 3 weeks after MVD. One patient, who underwent MVD on both sides, with an excellent result on one side but a poor result on the other side, both recommended and did not recommend MVD. All the other 92 patients (91%) recommended MVD for TN.
Discussion
In most classical TN cases, vascular compression of the trigeminal nerve is involved in the aetiology, and MVD is a safe surgical method widely used throughout the world for the treatment of TN. However, there have been reports that NC can not always be found during surgical exploration. These negative findings varied from 4% to 89%, with an average 7.5% (3, 13–15); the rate in our initial series was 20%. Before considering a posterior cranial fossa exploration for MVD it is advisable to prove the presence of NC of the trigeminal nerve. MRI and later MRA investigations have demonstrated the usefulness of the preoperative evaluation of NC in TN cases (8, 9, 12, 15–22).
In everyday clinical practice, neurologists encounter many patients with unilateral facial pain that is difficult to classify into the well-known types of headaches, facial pain syndromes and trigeminal neuralgia. In these PIFP cases, the origin of the pain is unclear and the treatment is often not fruitful. We performed 3D TOF MRA in 29 patients with PIFP, and only one of them yielded a positive result. This was most probably only an accidentally positive NC, because this patient showed no improvement after MVD. On the basis of these results, we can rule out NC in the background of PIFP.
The situation with typical TN and TNWIP cases was quite different. The MRA findings were positive in 66.5% in the typical TN group, and in 47.5% in the TNWIP group. Patients were selected for MVD only from among the MRA-positive cases (86 typical TN and 16 TNWIP), and in all these cases NC was found during surgery. With regard to the good postoperative results after MVD in the literature and in the present series, NC appears to be an obvious aetiological explanation of typical TN and TNWIP. However, it is noteworthy that, whereas typical TN was found to be caused by pure venous compression in only 0.8% on MRA and in 1.2% during surgery, TNWIP was caused by pure venous compression in 24.1% on MRA and in 31.2% during surgery. This might seem significant (FET, P < 0.01), but the small number of our cases permits only the suspicion that venous compression may cause TNWIP. On this basis, the different clinical symptoms (typical TN and TNWIP) seem to be dependent on the type of the compressing vessel. The duration of compression may also influence the appearance of clinical symptoms, and the typical form sometimes transforms into the TNWIP form (23).
It should be stressed that only patients who gave positive imaging results for NC were included in the MVD-treated group. Accordingly, the study is strongly biased from this aspect. It may be supposed that more cases from the MRA-negative group had NC, but the vessels were too small to be detected. The quality of the MR unit seems to be very important in this process. In our series of patients with TN, there were 72 patients with negative MRA results on use of the 0.5-T machine (see Table 3). The relative data suggest that, of these, 47 of these cases (65%) would have been positive if the 1-T MR unit had been used. This was not available to us at that time, but it means that approximately 47 patients were denied MVD due to ‘poor’ MRA. When the MRA investigations were performed with the 0.5-T machine, the positive ratio in the typical TN group was 60% (12); the corresponding value with the 1-T machine was 88%. This latter positive ratio approaches that for the surgically positive cases of Jannetta (5), and some cause other than NC (probably of central origin (24–26)) in the background of typical TN can be suspected only in 12%. At this point, the question arises of whether it is worth performing MRA in patients with typical TN when the expected negative ratio is only 12%. The answer may be ‘no’ if we consider selective partial rhizotomy as an alternative to MVD, while it may be ‘yes’ if we consider other surgical treatment (glycerol rhizotomy, thermocoagulation, balloon compression, etc.). In the TNWIP group, the positive MRA ratio was 25% with the 0.5-T machine, and 56% with the 1-T machine (Table 3). In this clinical group, preoperative MRA investigation seems to be indicated unequivocally. The previous published MRA studies were performed on 1.5-T MR machines (8, 9, 15, 18, 20, 21). Even with such technically superior equipment, there were false-negative cases (8, 9, 15, 22), which indicates that small arteries and also veins and thickened arachnoids can probably go undetected on MRA. Unfortunately, there are no data regarding the type of TN in these cases.
The 9.4% NC on the asymptomatic side suggests that the clinical symptoms and MRA results must be evaluated together. If we consider the same proportion of asymptomatic NC on the symptomatic side, this may explain the unsuccessful MVDs, where causes other than NC were to be found in the background of TN.
There were six operative cases where only loose contact could be observed during surgery; however, an NC was obvious on MRA. This reflects the importance of the condition of the patients. The position of the head and the discharge of cerebrospinal fluid during surgery may modify the relationship of the nerve and vessel (5, 27). It is worthwhile to mention that all of the six patients had typical TN, and five of them exhibited an excellent and one of them a good outcome.
Correlation between clinical symptoms, type of vascular compression and outcome of MVD
Many factors which may contribute to the success of MVD have been discussed in the literature, in connection with large series of TN patients (13, 28–41). We focused on the clinical symptoms and type of vascular compression. Szapiro et al. (38) consider the mode of pain manifestation of TN to be the most significant prognostic factor in the outcome of MVD. They categorize ‘paroxysmal pain only’ and ‘paroxysmal with a permanent pain component’. These two clinical groups correspond to our typical TN and TNWIP groups. Szapiro et al. (38) found that 95% of the typical TN group and 58% of the atypical TN group could be cured. In our study, 80% of the typical TN group were considered cured, while 14% had a moderate and 6% a severe recurrence; in the TNWIP group, 56% were cured, while 25% had moderate and 19% severe recurrence (Table 11). Patients with TN treated by ablative neurosurgical techniques also seemed to have a better outcome if they had typical TN rather than TNWIP (42–46). With respect to these results, we may say that the clinical appearance of the TN is an important prognostic factor in the outcome of MVD, and taking an exact history from the patient is mandatory.
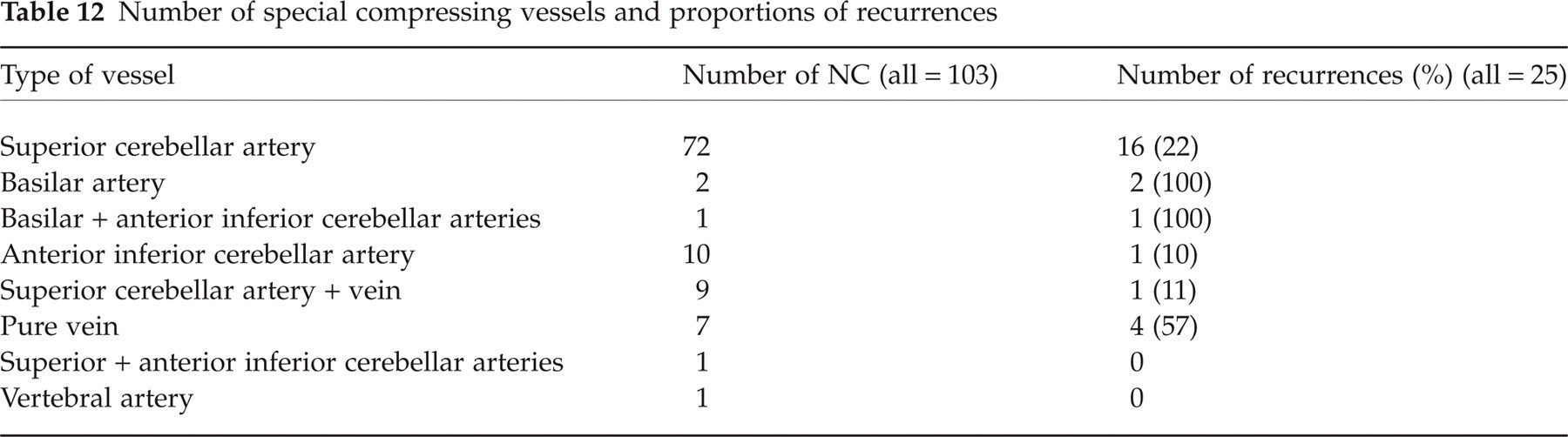
With regard to the special vessels and the number of all recurrences, it can be seen that, in cases where the basilar artery and veins are involved in the NC, the probability of recurrence is higher (Table 12). The reason for the recurrences in the basilar artery-caused NC cases might be the stiffness of the artery, which could therefore be moved away from the nerve only with difficulty (47). Since we used gelatin foam interposition between the nerve and vessel, the stiffness of the vessel may compress the gelatin foam after a certain time and the NC can be newly formed. This may be the cause of the recurrence of the other arterial compressions. The superior cerebellar artery (SCA) and the anterior inferior cerebellar artery (AICA) are also sometimes very stiff and difficult to move.
Number of special compressing vessels and proportions of recurrences
In one patient, the sensory root of the trigeminal nerve was divided longitudinally by a SCA loop; the distance between the two parts of the nerve (where the loop was) was around 10 mm, and the nerve seemed to be completely degenerated. In this case, there was no clinical improvement at all after MVD and later selective rhizotomy. We presume that the TN originated from the central structures by the time of MVD; nevertheless, the arterial compression could originally have been involved in the aetiology (31, 48).
The reason for the recurrences in cases involving the veins might be different. In most cases, the veins were divided and no chance of compression remained following MVD. In spite of this, the venous compression predicts a higher rate of recurrence of TN (13, 27, 30, 32, 33, 39). Since the veins can be distinguished from arteries on MRA, the positive MRA result may play a predictive role in the prognosis following MVD.
Little is known about the different potential effects of arterial vs. venous compression and the possible influence on the outcome of MVD. We may merely hypothesize, but without experimental or pathological proof. The arterial compression has two components: the constant compression due to the anatomical position of the vessel, and the strong rhythmic pulsation force on the nerve. The venous compression has only a constant ‘positional’ compressing force, but no strong pulsation. Both types of compression can cause focal demyelination, but there might be some difference between them. This pathological difference might be subtle, because both arterial and venous compression can cause typical TN and TNWIP, whereas arterial compression causes mainly typical TN, while in TNWIP the venous compression can frequently be found. An animal model or intraoperative biopsy taken from the affected nerve may answer this question, but this seems to be difficult in practice (49, 50). The pathomechanism must be clarified in the future.
Conclusions
PIFP is not related to NC of the trigeminal nerve.
In this series, patients with typical TN and TNWIP display special characteristics:
NC can be identified on MRA on a 1-T MR device in 88% of the typical TN cases and 56% of the TNWIP cases.
TNWIP is caused by venous compression at a significantly higher rate than that for typical TN.
Typical TN cases can be cured by MVD at a higher rate (80%) than can TNWIP cases (56%). This may be the most important prognostic factor in MVD (38).
In this series of patients, the type of vascular compression may play a role in the recurrence of TN following MVD.
MRA can be involved in the decision-making when considering MVD.
The type of MR unit significantly determines the accuracy of the MRA result and the percentage of MRA-positive cases. At least a 1-T MR unit is needed for the investigations.
Arterial and venous compression can be differentiated.
MRA-negative cases, and especially TNWIP cases, can be considered for treatment other than MVD.