
Abstract
Introduction
Medical treatments for trigeminal neuralgia secondary to multiple sclerosis have low efficacy and tolerability and scientific evidence regarding efficacy of neurosurgery is scarce. We aimed to assess neurosurgical outcome and complications in trigeminal neuralgia secondary to multiple sclerosis.
Methods
Patients with trigeminal neuralgia secondary to multiple sclerosis who underwent microvascular decompression, glycerol rhizolysis or balloon compression were prospectively and consecutively included from 2012 to 2019. Preoperatively, we systematically obtained clinical characteristics and performed a 3.0 Tesla MRI. Follow-up at three, six and 12 months was performed by independent assessors.
Results
We included 18 patients. Of the seven patients treated with microvascular decompression, two patients (29%) had an excellent outcome (both had neurovascular contact with morphological changes), three patients (43%) had a good outcome, one patient (14%) had treatment failure and one patient (14%) had a fatal outcome. Three patients (43%) had major complications. Of 11 patients treated with percutaneous procedures, seven patients (64%) had an excellent or good outcome with major complications in three patients (27%).
Conclusion
Percutaneous procedures provided acceptable outcome and complication rates and should be offered to the majority of patients with trigeminal neuralgia secondary to multiple sclerosis who need surgery. Microvascular decompression is less effective and has a higher complication rate in trigeminal neuralgia secondary to multiple sclerosis compared to microvascular decompression in classical and idiopathic trigeminal neuralgia. Microvascular decompression should only be considered in patients with trigeminal neuralgia secondary to multiple sclerosis when they have neurovascular contact with morphological changes.
Keywords
Introduction
Trigeminal neuralgia (TN), often referred to as one of the most painful diseases known, and multiple sclerosis (MS), the central nervous system (CNS) disorder, most frequently causing disability in young adults, are both chronic neurological diseases that negatively affect quality of life (1,2). TN is characterized by severe unilateral electric shock-like pain paroxysms in one or more branches of the trigeminal nerve. The paroxysms are short lasting with a maximum duration of two minutes and triggered by innocuous sensory stimuli (3). Based on magnetic resonance imaging (MRI), TN is classified as idiopathic, classical or secondary TN (4). Classical TN is diagnosed when MRI demonstrates neurovascular contact (NVC) between a vessel and the trigeminal nerve with morphological changes on the side ipsilateral to the pain. Conversely, idiopathic TN is diagnosed when no NVC is found or the NVC is without morphological changes, (i.e., simple NVC), as this is a common finding in healthy individuals (5,6). Secondary TN is caused by intracranial pathology, such as MS or a space-occupying lesion. MS is an autoimmune demyelinating disease with both inflammatory and neurodegenerative mechanisms (7). While TN is a rare disease in the background population, patients with MS have a 20-fold increased risk of developing TN (8,9). In the last decade, there has been an increased focus on the patho-aetiology and treatment strategies in patients with idiopathic and classical TN. Current evidence support the hypothesis of focal demyelination in a transition zone from central oligodendroglia myelination to Schwann cell myelination of the trigeminal nerve, termed the root entry zone, as a pathophysiological mechanism in TN of all causes (6). In TN secondary to MS (MS-TN) the demyelination of trigeminal afferents is most likely caused by a pontine plaque. However, Truini et al. (10) conducted a prospective clinical MRI study of patients with MS-TN and found evidence of a dual mechanism of NVC with morphological changes concurrent with an intrapontine demyelinating lesion on the symptomatic side (10,11). A recent MRI study in MS-TN patients from our group did not find a dual mechanism being prevalent as NVC with morphological changes was a rare finding (12).
There is still a lack of knowledge regarding aetiology and treatment of MS-TN. Previous studies on neurosurgical outcomes report only excellent outcome, i.e., complete pain freedom and no medication, in 15–39% of patients with MS-TN after microvascular decompression (MVD). These studies are hampered by a weak methodology of retrospective cohorts, non-independent evaluation of outcome and complications as well as no predefined outcome measures (13–17). In the absence of high quality evidence, the treatment strategy of MS-TN follows the same guidelines as for idiopathic and classical TN with respect to both medical and surgical treatment (18). The European Academy of Neurology guideline on trigeminal neuralgia recommends the use of carbamazepine and oxcarbazepine as first-choice medical treatment for idiopathic and classical TN. If ineffective, lamotrigine, gabapentin, botulinum toxin type A, pregabalin, baclofen or phenytoin can be considered (18). In medically refractory patients, MVD is the first-choice surgical treatment in classical TN. In idiopathic TN with NVC, there is no recommendation of one surgical procedure over another. In patients without NVC, neuroablative methods are recommended (18). These consist of gamma knife surgery, glycerol rhizolysis (GR), balloon compression (BC) and radiofrequency thermocoagulation. The neuroablative methods are – in view of low evidence – considered equally effective (18).
As outlined above, the evidence to support a specific treatment guideline for secondary TN is sparse and high-quality data is needed to allow for comparison between surgical outcome in classical TN, idiopathic TN and MS-TN. Medical treatments have poor tolerability in MS-TN due to significant side effects such as tiredness and ataxia and carries a risk of potentiating existing MS symptoms (19,20). Thus, neurosurgical interventions are often considered. We aim to report the efficacy of surgical treatment in medically refractory patients with MS-TN in a prospective manner using independent assessors.
Methods
Definition of the cohort and baseline characteristics
We consecutively and prospectively included patients diagnosed with MS-TN who underwent neurosurgery after referral from a neurologist at the Danish Headache Center (DHC), a tertiary medical treatment centre for headache and facial pain, between May 2012 and October 2019. Depending on the time of inclusion, the diagnosis of MS-TN was based on the International Classification of Headache Disorders (ICHD)-2, ICHD-3 beta or ICHD-3 criteria (4,21,22). Exclusion criteria were: a) incomplete one-year follow-up of surgical data and b) inability to provide informed consent.
After referral to DHC, all patients were evaluated through a clinical interview and a neurological exam. At the clinical interview, the neurologist filled out a semi-structured interview which included items on demographics, clinical characteristics, current and previous medical and surgical treatments, comorbidities, and sensory deficits. The methodology of the data collection was largely similar to the methodology described in previous studies from our research group of classical, idiopathic and secondary TN (12,23–26). The patients were referred to neurosurgery only when medical treatment failed, which was defined as insufficient efficacy or intolerability to carbamazepine and oxcarbazepine, or a combination of the best of the two and gabapentin, lamotrigine or pregabalin (18). Only patients with NVC were considered for MVD.
Presurgical neuroimaging
All patients had a 3.0 Tesla MRI scan within eight weeks of the clinical interview. The MRI scans were all evaluated by an experienced neuroradiologist (EAS), who was blinded to the symptomatic side. We used a 3.0 Tesla Phillips Achieva imager (Phillips Medical Systems, Best, Netherlands) equipped with a 32-channel head coil with Multi Transmit parallel RF transmission. The MRI protocol included sagittal T2-weighted turbo-spin-echo sequences covering the whole brain, T2-weighted DRIVE SPIR, 3D time of flight MR angiography (s3DI MC HR) and 3D high spatial resolution heavily T2-weighted sequences (3D balanced fast field echo [BFFE]). Multiplanar reconstructions were performed on the cisternal part of the NVC strongly parallel to the trigeminal nerve in the axial and sagittal plane and perpendicular to the trigeminal nerve in the coronal plane.
NVC was defined as contact between the trigeminal nerve and a blood vessel without visible cerebrospinal fluid between the two structures (5). If the neuroradiologist was uncertain whether there was contact or not, it was considered as no NVC. We distinguished between NVC with or without morphological changes. NVC with morphological changes was defined as NVC with compression, displacement, indentation, distortion or atrophy of the trigeminal nerve (4,5).
Pontine demyelinating plaques were considered relevant when located along the course of the intrapontine trigeminal afferents in the ventrolateral part of the pons including the pontine part of the trigeminal nuclei. The imaging protocol did not include the trigeminal nuclei located at the medulla oblongata or the spinal medulla. Postoperative imaging was only performed on clinical indication.
Neurosurgical technique
MVD, BC and GR were performed by specialized and highly experienced neurosurgeons (JBS and PR) at the Department of Neurosurgery, Rigshospitalet, Denmark.
Microvascular decompression
MVD was conducted as outlined in our previous publication concerning patients with classical and idiopathic TN (27). We only considered MVD when NVC was detected on presurgical MRI. The procedure was performed via a supracerebellar infratentorial approach through a retrosigmoid craniectomy. No retractors or specific relaxation techniques were used during surgery, and neither was neuronavigation nor brainstem auditory evoked responses or other neuromonitoring. The cerebellopontine angle was approached, and the trigeminal nerve and the compressing vessel(s) identified. In case of an arterial compression from the superior cerebellar artery, the nerve was preferably alleviated by transposition of the vessel. The vessel was transposed upwards and fixed to the tentorium with a piece of Teflon and glue. If transposition was not possible, a piece of Teflon was interposed between the nerve and the offending vessel. If the neurovascular contact was with the anterior inferior cerebellar artery or the posterior inferior cerebellar artery the interposing technique was used. If the compression was caused by a vein, the vein was either transposed and fixed with Teflon and glue or coagulated and divided to avoid avulsion (25).
Balloon compression
The patient was in the supine position with the head extended on a malleable pillow. A needle was placed in a custom-made handle visible to the neuronavigation system (Brain Lab). Guided by a predefined neuronavigation trajectory the needle was inserted through the skin near the corner of the mouth on the symptomatic side and thereafter passed through the oval foramen. The stilet was then removed from the needle and a balloon inserted and inflated with approximately 0.8 mL contrast medium (Omnipaque) under x-ray illumination. Correct position of the balloon was verified by the shape of the balloon corresponding the shape of the Meckel’s cave. The trigeminal ganglion was compressed for two minutes whereafter the balloon and needle were removed (28).
Glycerol rhizolysis
The patient was in the supine position with the head extended on a malleable pillow. A needle was inserted through the foramen ovale as described above. The head of the patient bed was then elevated to 90 degrees and 0.8 mL of glycerol injected through the needle. The patient’s head was then slightly flexed and fixed to a custom-made pillow with the patient still in a sitting position. This position was kept for one hour to ensure that the glycerol to the largest extent stayed in the Meckel’s cave.
Follow-up
All patients were assessed at three, six and 12 months after the surgical intervention and a purpose-built follow-up scheme was completed by a neurologist at DHC. Details on outcome according to a seven-point Barrow Neurological Institute Scale (BNI) (25,29), surgical complications, medication and medical side effects and pain intensity were included in the scheme. At the 12-month surgical follow-up, the patient received a self-complete patient-directed questionnaire (30) which was translated with minor modifications by our research group (25). In the event of any discrepancy between data from the patient-directed questionnaire and the clinical follow-up scheme, the data from the clinical follow-up scheme was reported. If the patient had undergone multiple surgical interventions, follow-up data from the first procedure was reported.
Surgical complications were graded as major or minor according to a predefined protocol described in detail elsewhere (27). Major complications were defined as death, ischaemic or haemorrhagic cerebellar or brainstem stroke, anaesthesia dolorosa, meningitis, cerebrospinal fluid leak, hydrocephalus, permanent ataxia, permanent diplopia, corneal keratitis, permanent severe hypoesthesia, permanent facial nerve palsy, permanent hearing loss or permanent hearing impairment. If a patient experienced a stroke due to the surgical procedure, the possible cranial nerve dysfunction, dizziness or ataxia caused by the stroke were not included as separate major or minor complications.
A complication was categorized as transient if it lasted less than 12 months and permanent if it persisted at the 12 months follow-up after surgery.
Minor complications were defined as dizziness, tinnitus, tiredness, wound infection, headache, cicatricial discomfort, transient ataxia, transient diplopia, reduced corneal reflex, missing corneal reflex, permanent mild hypoesthesia, transient mild hypoesthesia, transient severe hypoesthesia, trigeminal motor weakness (masseter dysfunction), transient facial nerve palsy, transient hearing loss, transient hearing impairment or altered sense of taste.
Outcome
The primary outcome was pain relief quantified on a modified BNI pain scale. The modification of the BNI was to ensure a more refined scale with a better distinction between the different outcomes of the procedure: I; complete pain relief: no pain and no medication (excellent outcome). II; partial pain relief: occasional pain but no medication required (good outcome). IIIA; partial pain relief: no pain but daily medication required (good outcome). IIIB; partial pain relief: occasional pain but adequately controlled with medication (good outcome). IV; poor pain relief: reduced pain but not adequately controlled with medication (poor outcome). VA; no pain relief (failure). VB aggravation of pain (failure).
Statistical analyses
Continuous and ranked data are summarized by descriptive statistics. Categorical variables are presented with frequency distributions (N, %), reported as numbers, means, percentages and with 95% confidence intervals (CI).
If more than 10% of the clinical data were missing, the patient was excluded from the analyses. Missing data was considered missing at random. P-values was reported as two-tailed with a level of significance of 5%. Analyses were carried out using SAS 9.4 (SAS Institute Inc., NC, USA). We used the STROBE reporting guidelines.
Results
Figure 1 displays the 18 patients included in this study of which 11 were women (61%) and seven were men (39%). The mean age was 54.6 years (range, 37 to 71) and the mean age at TN onset was 46.3 years (range, 36 to 57 years). The mean duration of TN and MS was 7.7 years (range, 0 to 27 years) and 15.9 years (range, 0 to 29 years), respectively. The majority (12 patients) had left sided pain, five had pain in the right side and one had bilateral pain. Seven patients (39%) were treated with MVD, six patients (33%) had BC and five patients (28%) underwent GR. The baseline characteristics are presented in Table 1.

Flowchart of patient inclusion from May 2012 to October 2019.
Baseline clinical characteristics of included patients with MS-TN (n = 18) who have undergone microvascular decompression (n = 7), balloon compression (n = 6) and glycerol rhizolysis (n = 5).
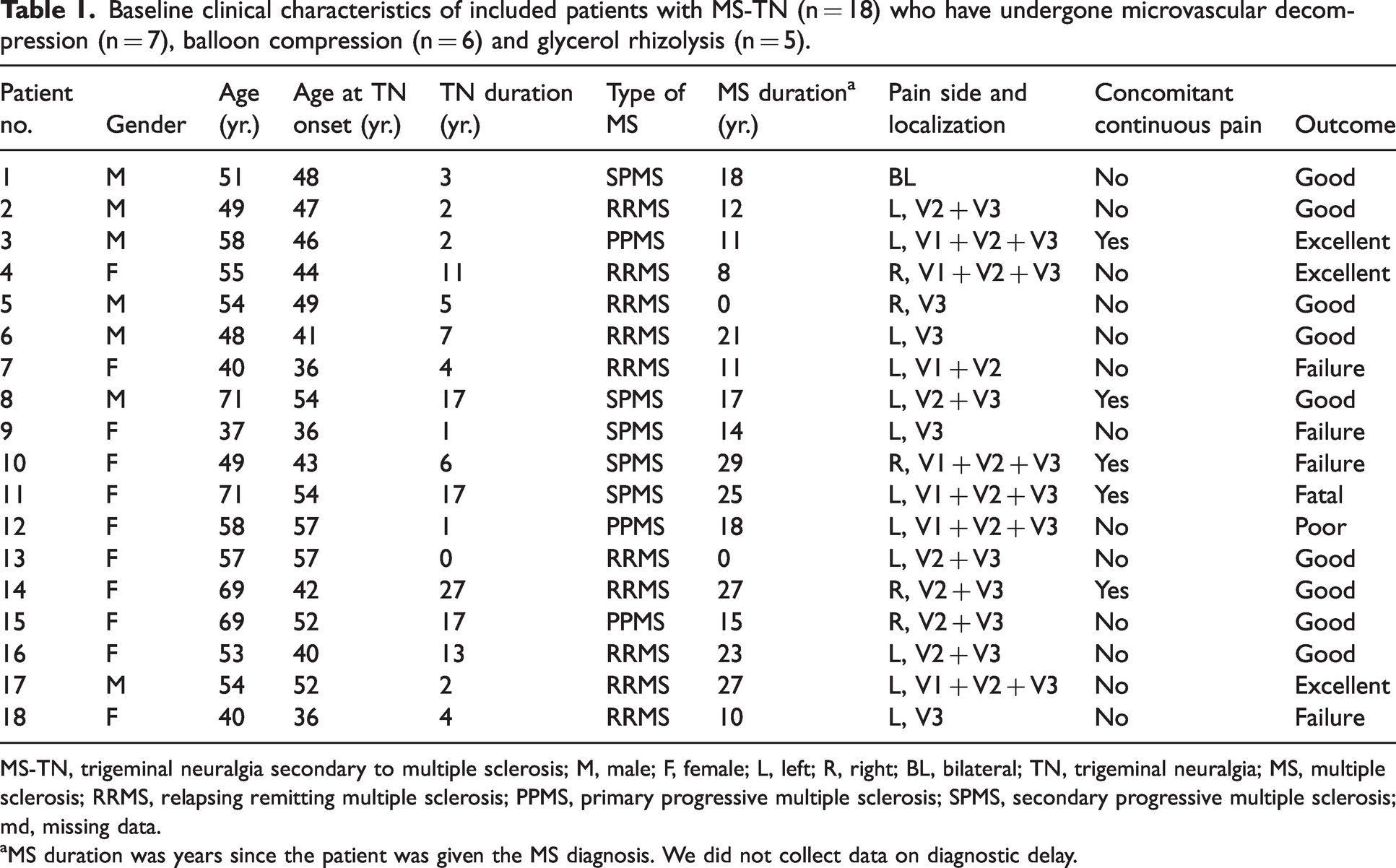
MS-TN, trigeminal neuralgia secondary to multiple sclerosis; M, male; F, female; L, left; R, right; BL, bilateral; TN, trigeminal neuralgia; MS, multiple sclerosis; RRMS, relapsing remitting multiple sclerosis; PPMS, primary progressive multiple sclerosis; SPMS, secondary progressive multiple sclerosis; md, missing data.
aMS duration was years since the patient was given the MS diagnosis. We did not collect data on diagnostic delay.
Outcome
Of the seven patients who underwent MVD, two patients (29%) had an excellent outcome (BNI I), and three patients (43%) had a good outcome (BNI IIIA-IIIB). One patient (14%) had treatment failure (BNI VA) and one patient (14%) had a fatal outcome (Figure 2 and Table 2). Presurgical MRI demonstrated NVC with morphological changes of the trigeminal nerve on the symptomatic side (Table 3) in the same two patients with an excellent outcome.

Outcome and complications after MVD and percutaneous procedures (BC and GR). For a graphical illustration of the differences across groups and procedures our data from patients with MS-TN on MVD outcome (a) and complications (b) and outcome (c) and complications (d) following percutaneous procedures are presented, with data on MVD outcome (e) and complications (f) from a recently published study 27 using the same methodology in CTN and ITN (n = 115) with NVC.
Outcome and complications after microvascular decompression, glycerol rhizolysis and balloon compression.
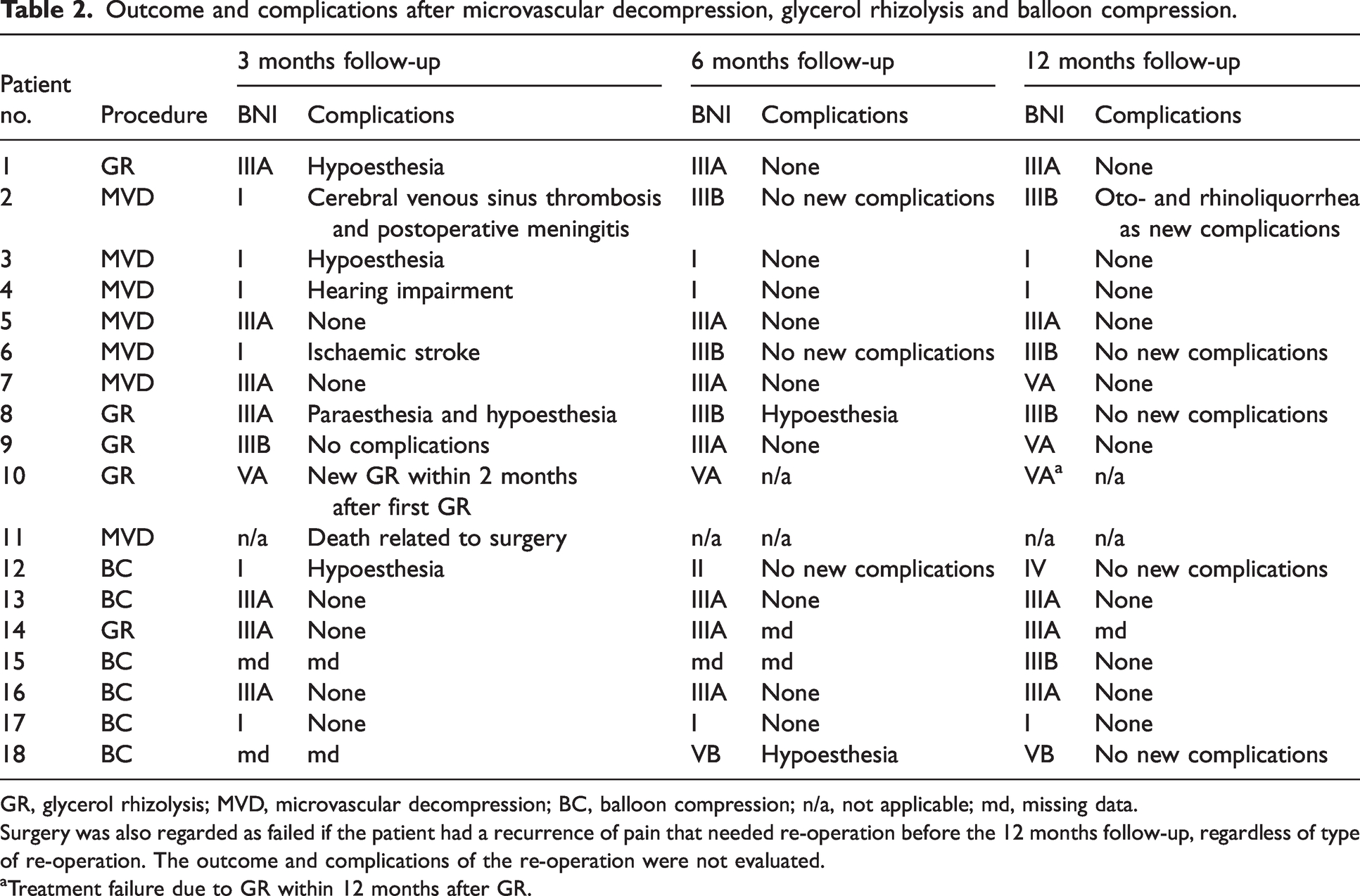
GR, glycerol rhizolysis; MVD, microvascular decompression; BC, balloon compression; n/a, not applicable; md, missing data.
Surgery was also regarded as failed if the patient had a recurrence of pain that needed re-operation before the 12 months follow-up, regardless of type of re-operation. The outcome and complications of the re-operation were not evaluated.
aTreatment failure due to GR within 12 months after GR.
Neuroimaging characteristics prior to microvascular decompression, glycerol rhizolysis and balloon compression.
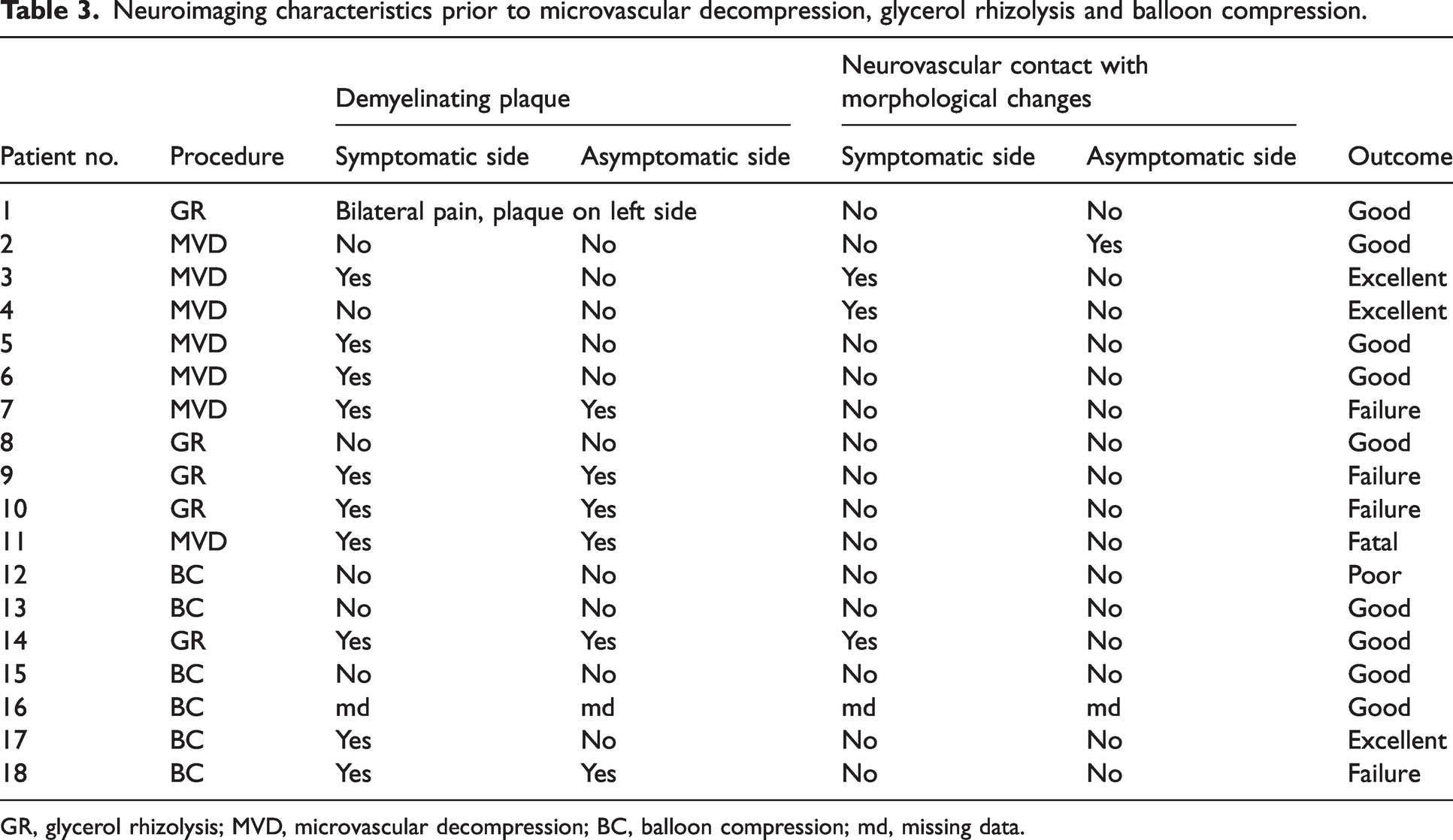
GR, glycerol rhizolysis; MVD, microvascular decompression; BC, balloon compression; md, missing data.
Six patients underwent BC. One patient (17%) had an excellent outcome (BNI I), and three patients (50%) had a good outcome (BNI IIIA-IIIB) at the 12-months follow-up. One (17%) patient had a poor outcome (BNI IV), and one (17%) patient had treatment failure (BNI VB). Of the five patients who had GR two (40%) patients had a good outcome (BNI IIIB). The remaining three (60%) patients had treatment failure (BNI VA) (Table 2).
Concomitant continuous pain was present in five of the 18 patients. One patient had NVC with morphological changes, underwent MVD, and had an excellent outcome. Three patients were treated with GR. Of those, two had a good outcome and one had treatment failure. One patient had a fatal outcome after MVD (see complications section).
The mean duration of disease was 8.8 years in patients with an excellent or good outcome, and 5.5 years in patients with an outcome defined as poor, failure, or fatal. The duration of MS was 14.9 years in patients with an excellent or good outcome, and 17.8 years in patients with an outcome of either poor, failure, or fatal. The difference between the means of disease duration was not significant.
Complications
Major and minor complications at the 12 months follow-up are presented in Table 2.
Microvascular decompression
Three patients (43%) had major complications, including the patient with a fatal outcome, and two patients (29%) had minor complications (transient hypoesthesia and transient hearing impairment). Two patients (29%) had no surgical complications (Figure 2). One patient was re-operated due to displacement of the inserted Teflon verified by postoperative MRI, but this was not considered a complication to surgery.
Patient no. 2 had three major complications that were considered as independent complications. Post-operative meningitis was confirmed by a spinal fluid tap. It was treated with intravenous antibiotics and re-operation by insertion of TachoSil covering a dural defect. A cerebral venous sinus thrombosis was verified on an MRI scan 35 days postoperatively. The sinus thrombosis was localized to the internal jugular vein and was treated with anticoagulant medication. Cerebrospinal fluid (CSF) leakage by means of oto- and rhinoliquorrhea due to a CSF fistula was verified 12 months after surgery. The patient was re-operated once with surgical closing of two defects of the dura mater identified intraoperatively. Patient no. 6 had a symptomatic mesencephalic ischemic stroke on day one postoperatively. The patient was known to have protein S deficiency. The patient had permanent dysarthria, ataxia and diplopia caused by the stroke. Patient no. 11 had a fatal outcome that was considered a complication of surgery. A few hours after surgery, the patient gradually lost consciousness. A CT-scan showed a subdural hematoma in the posterior fossa, which prompted an acute re-operation to evacuate the hematoma. However, the hematoma was only incompletely removed, and the procedure was complicated by insufficient coagulation. The patient died a few hours postoperatively.
Balloon compression and glycerol rhizolysis
Of the six patients who underwent BC, two patients (33%) had persistent hypoesthesia at the 12-months follow-up, which was considered a major complication. Four patients (67%) did not have any complications related to BC.
Following GR one patient (20%) had hypoesthesia at the 12-month follow-up which was considered a major complication and one patient (20%) had transient hypoesthesia. The remaining three patients (60%) did not have any complications related to GR.
Discussion
This is the first study to follow surgically treated MS-TN patients prospectively and systematically with independent assessors of outcome and complications after one year. We show that 64% of the patients treated with percutaneous procedures had a good or excellent outcome versus 71% of patients treated with MVD. However, major complications were more frequent and generally more serious after MVD compared to the percutaneous procedures. The age of onset is consistent with the known earlier onset of MS-TN, typically in the between 40 and 50 years (31,32).
Does diseases duration and concomitant continuous pain determine surgical outcome?
Five patients in this study had concomitant continuous pain. Of those, three had a good or excellent outcome, one had treatment failure and one had a fatal outcome. The patient with excellent outcome had MVD and significant neurovascular contact. More than half had a clinically significant outcome (excellent or good), and TN duration showed a trend towards being shorter if the patient had poor outcome or failure. However, due to the small population, it is not possible to conclude whether concomitant continuous pain or disease duration significantly influences the surgical outcome.
Outcome after microvascular decompression may be dependent on neurovascular contact
In the present cohort, two patients had NVC with morphological changes and both patients had an excellent 12-month outcome after MVD. This is an important finding and highly indicative of NVC with morphological changes being a positive prognostic factor when it comes to efficacy of MVD in MS-TN. NVC is probably the primary cause of TN in patients with classical TN, and consequently many patients with classical TN obtain not only a good but an excellent outcome after microvascular decompression (5,18,25,27). In a recent paper from our center using the same methodology as the present study on the two-year outcome after MVD in patients with idiopathic with simple NVC (i.e. without morphological changes) and classical TN, we found that NVC with morphological changes was highly predictive of an excellent outcome and an excellent outcome occurred in 70% of all patients. Historically, studies on outcome after MVD in MS-TN have shown inconsistent results. A recent study with a mean follow-up of 88.2 months included 15 patients and reported an excellent outcome in three patients (20%). The study did not use independent assessors nor reported on complications and five patients were re-operated (14). Other retrospective studies reported an excellent outcome after MVD in 15-39% of patients (15–17).
Truini et al. (10) found that 17 of 28 patients with MS-TN had ipsilateral NVC with morphological changes and along with a demyelinating plaque. The authors concluded that NVC appeared to be of major importance to disease aetiology in MS-TN. In contrast, our research group recently found no association between a NVC with morphological changes and the symptomatic side in patients with MS-TN (12). The present results are in agreement with this as only two MS-TN patients had NVC with morphological changes. As outlined above, our study and previous studies report much lower rates of excellent outcome after MVD in MS-TN compared to studies in idiopathic and classical TN. This is suggestive of NVC being a less significant mechanism in MS-TN compared to its importance in idiopathic and classical TN. We suggest, that MVD should only be performed in MS-TN patients who have NVC with morphological changes on the relevant side.
Recent diffusion tensor imaging (DTI) studies from a neurosurgery-based research group in Canada indicated that microstructural white matter abnormalities in the cisternal segment of the trigeminal nerve – as opposed to the root entry segment or the intrapontine segment – can predict a good outcome after MVD in MS-TN (33). By using diffusion tensor imaging assessing trigeminal microstructure a pre-surgical method of response prognostication is proposed. This method could potentially heighten the rate of surgical success in MS-TN (34,35). However, DTI is not performed routinely in most clinical centres.
To our knowledge there are no previous studies of surgical treatment in patients with MS-TN using independent assessors of complications. In a study of 35 patients, Broggi et al. (15) reported complications (CSF leakage and one case with facial nerve palsy) in only 6% of the patients. In a cohort of 24 patients, Paulo et al. (16) found a 38% rate of major complications (aseptic meningitis, CSF leakage and pseudomeningocele), hence similar to our findings. The combined findings from the current and previous studies indicate that complications related to MVD are generally much more frequent in MS-TN compared to classical and idiopathic TN, but the evidence is based on few studies (20,36,37).
Percutaneous procedures
Percutaneous procedures are more often performed in patients with MS-TN compared to MVD (20). A retrospective study by Noorani et al. (38) with a mean follow-up of 25 months including 33 MS-TN patients who underwent 64 percutaneous procedures, reported an excellent outcome in 56% of the patients after BC and in 48% of patients after GR. Another retrospective study by Mohammadi-Mohammadi et al. (39) included 277 procedures in 96 patients with MS-TN and of the 19 patients who underwent BC as the first procedure, 39% had a good outcome after a mean follow-up of 29 months. Thirty-nine patients underwent GR and 49% had a good outcome after a mean follow-up of 28 months. The complication rate was 25% after BC and 16% after GR. Most complications were minor such as dysesthesia and reduced corneal reflex.
We considered hypoesthesia as both a major and minor complication in this study, according to the degree of severity. However, a Danish neurosurgical study reported longer pain relief in patients with hypoesthesia following glycerol injection (40). Thus, in future studies it should be considered whether hypoesthesia should be regarded as a complication.
Strengths and weaknesses
This study reports outcome and complications from surgical procedures in patients with MS-TN using independent evaluators which – in addition to the prospective design – is a major strength and most likely reduces the risk of evaluation bias. Simultaneously, this design probably results in a lower efficacy and a higher complication rate in comparison with results from retrospective studies without independent assessment.
The BNI scale is the most widely used scale in neurosurgical TN studies although it has never been validated (41). The modified BNI scale we used in this study is easy to use in the clinical setting but yields only degree of pain relief and the level of medication usage among several other important outcome measurements, e.g., pain intensity, physical and emotional functioning. To obtain more details regarding outcome we used a modified version which unfortunately hampers the ability to compare results across studies. A well-defined set of core outcomes is much needed in TN and would be more appropriate for future neurosurgical studies. We did follow-up until 12 months postoperatively, which is a limitation to our study as other studies report longer follow-up data. Lastly, the small sample size is an important limitation of this study.
Conclusions
Surgical treatment with MVD is effective in the sub-group of MS-TN patients with morphological changes of the trigeminal nerve, but MVD also carries a high risk of major complications. The outcome and rate of surgical complications after percutaneous procedures were acceptable and comparable to MVD in classical and idiopathic TN. As a surgical treatment strategy in patients with MS-TN, we propose that percutaneous procedures should be first-choice in the majority of patients and that MVD should only be considered in patients with NVC with morphological changes.
Article Highlights
MVD is less effective and has a higher complication rate in MS-TN. Percutaneous procedures recommended as first-choice surgical treatment. MVD only recommended when NVC with morphological changes is present.
Footnotes
Declaration of conflicting interests
The authors declare no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research data
Qualified researchers can, upon reasonable request to the corresponding author, be given access to the data after approval from the Danish Data Protection Agency, after approval of a proposal and with a signed data access agreement. Patient-level data will be deidentified and study documents will be redacted to protect the privacy of the included participants.
Standard protocol approvals and patient consents
The Danish National Committee on Health Research Ethics confirmed that this project did not need ethical approval, as it was observational and based on routine clinical care and laboratory workup. All patients gave their written informed consent according to the regulations of the Danish Data Protection Agency.