
Abstract
Several studies have shown the presence of a comorbidity between migraine and vascular diseases, like hypertension and stroke. The mechanisms of this comorbidity are unknown. Impaired insulin sensitivity has recently emerged as a risk factor for hypertension and stroke. We evaluated insulin sensitivity in 30 young, nonobese, nondiabetic, normotensive migraine patients and in 15 healthy controls. During the OGTT, glucose plasma concentrations were significantly higher in migraineurs than in controls. Insulin sensitivity, as measured by ISI-stumvoll and OGIS-180 indexes, was significantly altered in migraine. Our data show that insulin sensitivity is impaired in migraine and suggest a role for insulin resistance in the comorbidity between migraine and vascular diseases.
Introduction
Migraine is a chronic neurovascolar disorder characterized by recurrent headache attacks associated with neurological and autonomic symptoms. Epidemiological studies have shown the presence of a strong association between migraine and vascular diseases, such as hypertension and stroke (1–3). In women of childbearing age, migraine significantly increases the risk of ischaemic stroke independently from other vascular risk factors (4). The putative neurobiological mechanism underlying this comorbidity is unknown.
Impaired insulin sensitivity (insulin resistance) has recently emerged as a risk factor for hypertension and stroke (5, 6). Insulin resistance is a state in which a normal amount of insulin produces a subnormal physiological response. The hyperinsulinaemic-euglycaemic glucose clamp is considered the most definitive method to measure insulin sensitivity in humans but it is experimentally demanding and costly. Alternative methods have been proposed. The oral glucose tolerance test (OGTT) is a test widely used for glucose tolerance classification. The OGTT provides information on insulin secretion and action but does not directly yield a measure of insulin sensitivity. Various attempts have been made to obtain such a measure and, recently, some of these indexes showed a highly significant correlation with the clamp (7, 8).
To evaluate whether migraine patients present an impaired insulin sensitivity we performed the OGTT in a group of otherwise healthy migraine patients recruited from an university-based Headache Clinic and in healthy controls.
Methods
Patients
Thirty consecutive migraine patients (10 men, 20 women; mean age ± SD, 30.3 ± 8.5 years), attending for the first time the Headache Centre of the University of Turin (Italy), were selected for the study. The diagnosis of migraine was made according to the ICHD-II criteria (9). The patients underwent an extensive physical and neurological examination. A standardized record of all the clinical and psychological characteristics of headache was obtained. No patient was on prophylactic antimigraine treatment. Patients with drug abuse, anxiety (STAI-X1 and STAI-X2) and/or depressive (BDI) disorders were discharged. A group of 15 age and sex matched healthy subjects (5 men, 10 women, mean age ± SD, 28.2 ± 10.3 years) was used as control. Subjects were excluded if they were obese (BMI ≥ 25 kg/m2), had diabetes (2-h plasma glucose ≥ 200 mg/dl), hypertension (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg). No subject had a medical history positive for TIA or stroke. The diet and the physical activity were not significantly different in migraine patients from controls. All the subjects gave their written informed consent to the study. The demographic and clinical characteristics of migraineurs and controls are shown in Table 1.
Clinical and laboratory characteristics of migraine patients and controls
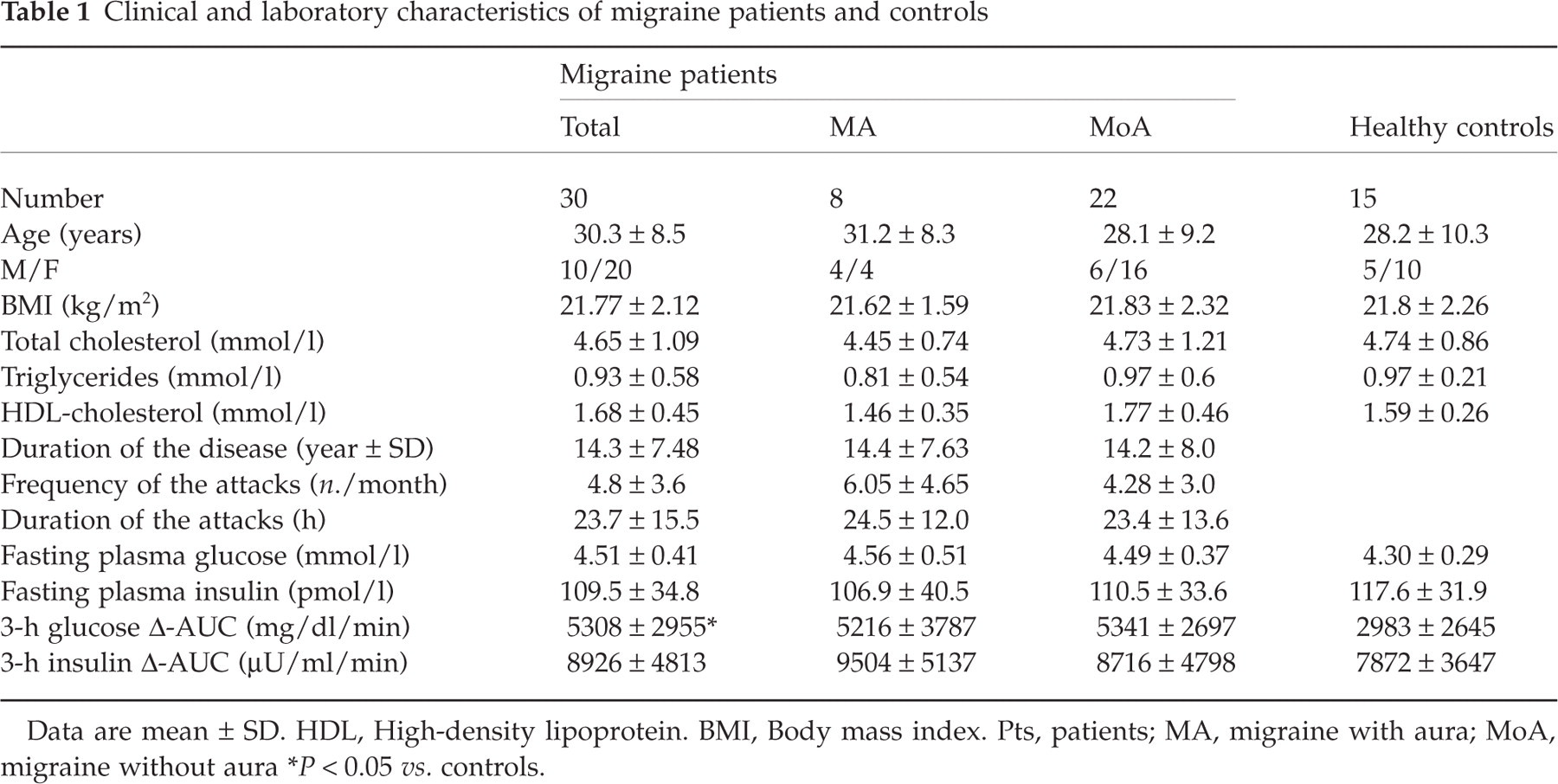
Data are mean ± SD. HDL, High-density lipoprotein. BMI, Body mass index. Pts, patients; MA, migraine with aura; MoA, migraine without aura
P < 0.05 vs. controls.
Laboratory analyses
A standard 75 g OGTT was performed after a 10-h overnight fast. Plasma samples were obtained at 0, 30, 60, 90, 120 and 180 min after glucose loading. Glucose was determined using a glucose oxidase autoanalyser, and immunoreactive insulin was measured by an enzyme immunoassay (Insik-5, Dia-Sorin, Saluggia, Italy).
Calculations
The plasma glucose response and total insulin secretion were evaluated from the Δ-AUC (area under the response curve after the subtraction of the basal concentrations) for plasma glucose and insulin concentrations. Insulin sensitivity/resistance was evaluated, using the OGTT values, by five different formulas: HOMA-R, ISI-composite, ISI-stumvoll, QUICKI and OGIS-180 (10).
The HOMA-R was calculated from the product of the fasting concentrations of plasma insulin and plasma glucose divided by 22.5. The insulin sensitivity index proposed by Matsuda and De Fronzo (10) was calculated as follows:
ISI-composite = 10,000/√[(mean plasma insulin × mean plasma glucose during OGTT) × (fasting plasma glucose × fasting plasma insulin)].
The ISI index proposed by Stumvoll et al. (10) was calculated as follows:
ISI-stumvoll = 0.226 − (0.0032 × BMI) − (0.0000645 × I120) − (0.00375 × G90).
The QUICKI was calculated as follows:
1/[log (fasting plasma insulin) + log (fasting plasma glucose)].
The OGIS-180 index (http://www.ladseb.pd.cnr.it/bioing/ogis) was calculated as follows:
ClOGTT = p4 × {[p1 D0 − V(G180 − G 120)/60]/G120 + p3/G0}/[I120 − I0 + p2]
B = [p5 (G120 − GCLAMP) + 1] × ClOGTT;
OGIS Index = 0.5 × {B + √[B2 + 4 × p5 × p6 × (G120 − GCLAMP) × ClOGTT]}
in which p1, p2, p3, p4, p5, and p6 are parameters (289, 270, 14,000, 440, 0.000637, and 117, respectively), D0 is the oral glucose dose, V represents the total glucose distribution volume, and GCLAMP is 90 mg/dl.
Statistics
Statistical analyses were performed using SigmaStat – version 1.0 (Jandel Corp., 1994, San Rafael, CA, USA). Data are presented as the mean ± SD. After normality tests for numeric values, comparisons between groups were performed using Student t-test, one way
Results
No patient developed migraine during the OGTT. Table 1 and Fig. 1 show glucose and insulin plasma concentrations during the OGTT. Basal glucose and insulin concentrations were not significantly different between patients and healthy controls. Glucose concentrations at time 90, 120, and 180 mins and 3 h glucose Δ-AUC were significantly higher in migraine patients than in controls.

Oral glucose tolerance test (OGTT) in patients with migraine and controls. ▪ Migraine patients, □ Controls. Values are mean ± SE.
Table 2 shows the indexes of insulin sensitivity in migraine patients and controls. HOMA-R, QUICKI and ISI-composite were not significantly different between patients and controls. However, in comparison with controls, ISI-stumvoll and OGIS-180 were significantly altered in migraine patients. When the patients were divided into subgroups (migraine with aura/without aura) no significant difference between subgroups was found. The OGIS-180 was significantly lower in migraine without aura patients than in controls.
Insulin sensitivity indexes in migraine patients and controls

Data are mean ± SD. Pts, patients; MA, migraine with aura; MoA, migraine without aura.
P < 0.05 vs. controls,
P < 0.01 vs. controls.
Discussion
In our study we found that insulin sensitivity is altered in migraine. During the OGTT, glucose plasma concentrations in nonobese, nondiabetic, normotensive migraine patients resulted significantly higher than in controls. Fasting-based indexes of insulin sensitivity were not significantly different between patients and controls. However, indexes of insulin sensitivity including all the OGTT-derived data and the BMI values, like ISI-stumvoll and OGIS-180, showed a condition of insulin resistance in migraineurs. No significant difference between migraine with aura and migraine without aura was found, but the number of patients examined in the subgroups may be too low to reach a statistically significant difference. To our knowledge, this is the first study that examined insulin sensitivity in patients with migraine and additional studies in different populations may be useful to confirm our data. Recently, Bic et al. (11) suggested that biological states, like insulin resistance, that increase free fatty acids and blood lipids may be an underlying factor in the development of migraine headaches. However, no experimental data supporting this hypothesis were provided.
Insulin resistance has been associated with a number of diseases, including type 2 diabetes, hypertension, obesity, dyslipidaemias, coronary artery disease and stroke (12–15). Our data suggest the presence of insulin resistance also in migraine. There are several findings suggesting a link between insulin metabolism and migraine. Patients with migraine frequently report that fasting, a condition where there is an insulin receptor activation, is a trigger of headache attacks (16). Low-sucrose diet may reduce the frequency of migraine attacks (17). In migraineurs, the onset of diabetes significantly increases the average yearly number of headache days (18). Finally, a recent study showed a significant association between polymorphisms in the insulin receptor (INSR) gene and migraine and suggested possible functions for the insulin receptor in migraine pathogenesis (19).
The adverse biological events associated with insulin resistance include abnormal fibrinolysis, hyperglycaemia, hyperinsulinaemia, systemic inflammation, hypertension, altered vascular endothelial function, and atherogenesis. Insulin resistance is also associated with enhanced platelet aggregation and incremented serum von Willebrand factor. Several of these abnormalities have been reported in patients with migraine and may be related to the increased risk for hypertension and stroke in this disease (20–22).
The results of our study, if confirmed in independent populations, may have practical applications. Strategies that improve insulin sensitivity may be of benefit in migraine. Aerobic exercise reduces insulin resistance and therefore could reduce the vascular complications in migraineurs (23). Effective insulin sensitizing drugs have recently become commercially available (24) and these drugs could be tested in migraine prophylaxis. Additional research will be necessary to elucidate the role of insulin resistance in migraine pathogenesis and to evaluate new strategies for disease prevention.
Footnotes
Acknowledgements
The study was supported by a 2001 grant from the ‘Ministero dell’Università e della Ricerca Scientifica (MURST) of Italy and by a 2003 grant of Regione Piemonte.