
Abstract
Clinical observations have shown that migraine is a progressive disorder, both within an acute attack, and within the disease itself. Rates of diagnosis for migraine have increased in the last decade, but more than half of migraineurs remain undiagnosed. Patient expectations of migraine therapies have also increased (patients require rapid and sustained pain relief with a treatment that has good tolerability), and can differ greatly from those of physicians. Management decisions should be made with these expectations in mind, to enhance patient outcomes and compliance with treatment. Improved understanding of acute migraine attack pathophysiology has led to the strategy of early treatment to modify both the progression of the current attack and, potentially, the progression of the disease itself in the individual. The triptans are effective acute migraine therapies. Each agent has its own distinct profile of efficacy and tolerability, enabling individualization of treatment.
Introduction
Formerly, migraine was perceived as a ‘troublesome’ complex of symptoms. However, over the last 20–25 years this perception has evolved and migraine is now classified as a disease. There has also been an increase in patient expectations from therapy.
Migraine is a progressive disorder. Within an attack, progression is seen from the phenomenon of aura (if present), to the development of pain and throbbing, and finally sensitization of central neurones leading to increased pain and the development of cutaneous allodynia (1,2). Early administration of migraine therapy, i.e. before the development of central sensitization, is associated with maximized effectiveness and optimal patient outcomes.
Furthermore, in some patients the disease itself can advance, for example evolving from an episodic condition with recurrent acute attacks into chronic daily headache with associated debilitation. Structural changes in the brain can accompany the progression in attack frequency and severity. These changes may include iron accumulation in the periaqueductal grey, which causes impairment of the antinociceptive system that controls activity in the trigeminovascular system (3), and changes in the primary visual cortex caused by cerebral ischaemia during acute migraine attacks (4). Subsequently, visual impairment and cognitive dysfunction may develop and affected individuals may be put at increased risk of stroke (5).
In clinical practice, observations of migraine characteristics and behavioural triggers can be made for the individual patient. Analytic epidemiological case-studies and cohort studies can be used to examine patterns of disease features in a wider population and to identify modifiable risk factors. These factors provide a basis from which to measure the efficacy of treatment through controlled clinical trials, which in turn provide the evidence base required to implement changes in clinical practice to improve management of the individual patient.
Modification of the clinical course of migraine requires an understanding of the natural history of the disease and the identification of measurable endpoints that reflect disease progression. In addition, those patients with migraine who are at risk of progression must be identified. Intervention should have disease-modifying effects, slowing or preventing such progression (6). Current estimates suggest that around 4% of the US population experience transformation from episodic migraine attacks to disabling chronic daily headache (7). These patients respond poorly to treatment, and often develop occupational, social and behavioural disability and psychological pathology (6).
This article reviews migraine therapy from the patient's perspective and discusses management strategies to abort attacks and to modify the clinical course of the disease.
A severe and disabling condition
Around 12% of the US population is affected by migraine, making this disease more common than osteoarthritis (7%), asthma (7%), diabetes (6%) and rheumatoid arthritis (1%) (8–11). A similar proportion of the population in Europe is affected by migraine (12). Women are 2–3 times more likely than men to be migraineurs (13).
In a survey of global disease burden, the World Health Organisation (WHO) identified severe migraine, along with psychosis, quadriplegia and dementia, as one of the most debilitating chronic conditions (14).
The second American Migraine Study evaluated the prevalence and burden of severe migraine in the US (15,16). A questionnaire, sent to 20 000 households chosen at random, evaluated headache features and related disability. Overall, 29 727 respondents completed and returned the questionnaire. The prevalence of migraine in this sample was 18.2% in females and 6.5% in males. Among those who had received a physician diagnosis of migraine, 89.7% reported suffering from severe or extremely severe pain (Fig. 1). A high prevalence of severe or extremely severe pain (72.1%) was also seen in respondents who met the International Headache Society (IHS) criteria for migraine but had not been diagnosed. More than 60% of respondents with migraine experienced one or more severe headaches per month.

Pain severity reported by participants of the American Migraine Study. (a) Diagnosed migraineurs; (b) Undiagnosed migraineurs (15).
The impact of migraine-induced impairment often goes unmeasured in clinical practice. The American Migraine Study found that the majority (>90%) of migraineurs reported functional disability with their headaches – 53% reported severe impairment or required bed rest during their attack (Fig. 2). One in every three migraineurs missed at least 1 day of school or work in the 3 months prior to the survey, with half of all patients reporting a reduction in productivity of at least 50% during an attack. Activity restriction lasted up to a day in 49% and between 1 and 2 days in 29% of migraineurs (16). In addition, migraine sufferers have lower health-related quality of life scores compared with control subjects, and quality of life in these individuals decreases further with increasing severity of migraine-related disability (15).

Disability during severe headaches among participants of the American Migraine Study. Adapted with permission from (15). © 2001, Blackwell Publishing Ltd.
Awareness of migraine is increasing in clinical practice, as witnessed by an improvement in diagnosis rates over the last decade recorded by the American Migraine Study (15–17). In 1989, only 39% (29% of males; 41% of females) of people meeting the IHS criteria for migraine had received a medical diagnosis from a physician. In 1999, the population receiving a medical diagnosis had increased to 48% (41% of males; 51% of females). However, this study illustrates that more than half of people meeting the IHS criteria for migraine remain undiagnosed (15–17). Rates of migraine diagnosis are higher for women than men (51% of women with migraine are diagnosed vs 40% of men), and increase with age in both sexes (15).
The lack of medical consultation for headache is a major contributing factor to the underdiagnosis and undertreatment of migraine, with one in every three migraineurs never having consulted a physician about their headache (18). Diagnosis is also complicated because patients rarely consult their physicians during an attack and physicians must therefore rely on a retrospective description of the patient's symptoms.
The continuing underdiagnosis of migraine constitutes a significant public health problem, due to the substantial disability associated with this disorder. As shown in Figs 1 and 2, a high proportion of these patients experience severe or extremely severe pain, associated with significant headache-related disability, and thus would benefit from intervention.
Goals of migraine management
Once migraine is diagnosed, illness severity and related disability can be assessed and a treatment plan developed. As migraine can vary between individuals, and even between attacks, any such management plan should be individualized and take into consideration patient needs and preferences for treatment.
The goals of long-term migraine management should include reducing attack frequency, duration and intensity, reducing headache-related disability and improving quality of life, reducing headache-related distress and psychological symptoms and educating patients to avoid triggers and manage their condition appropriately (19). Management of migraine often requires an integrated approach to care. The more severe the disease, the greater the need to involve additional aspects of treatment. For example, very mild cases may be managed successfully through avoidance of trigger factors alone, while patients with more severe attacks may require a combination of behavioural modification to reduce attack frequency and acute treatment to reduce attack duration and intensity. Preventive therapy may also be indicated; for example, if migraines are recurrent and disabling despite acute treatment.
The goals of acute migraine treatment are to treat attacks rapidly and consistently, prevent recurrence and restore the patient's ability to function. This should be achieved with minimal requirement for rescue medication, and acute treatments should have few or no adverse events (19).
Patient needs and expectations from acute treatment
Patterns of consultation for migraine can indicate levels of satisfaction with management and therapy. Surveys have found that fewer patients lapse from care than was previously the case (Fig. 3) (18,20). According to the American Migraine Study in 1989, 21% of migraineurs had consulted a doctor for their headache within the last year (current consulters) while 46% had lapsed from care (i.e. they had not seen a doctor for at least 1 year) (20). Almost a decade later, this trend had reversed with 48% of respondents remaining under the care of a physician while only 21% had lapsed from care (18). The increase in current consulters may be associated with improvements in treatment. Interestingly, the proportion of migraineurs never consulting for their condition remained relatively constant over this time span (18,20).

Patient expectations have changed dramatically since the recognition of migraine as a disease, and the introduction of effective treatments for migraine. According to a survey of 688 migraineurs, only 29% of patients state that they are ‘very satisfied’ with their usual acute migraine treatment (21). Reasons for dissatisfaction included the medication taking too long to work; not completely relieving the pain; not always being effective; not preventing recurrence; or having too many side-effects (Fig. 4).
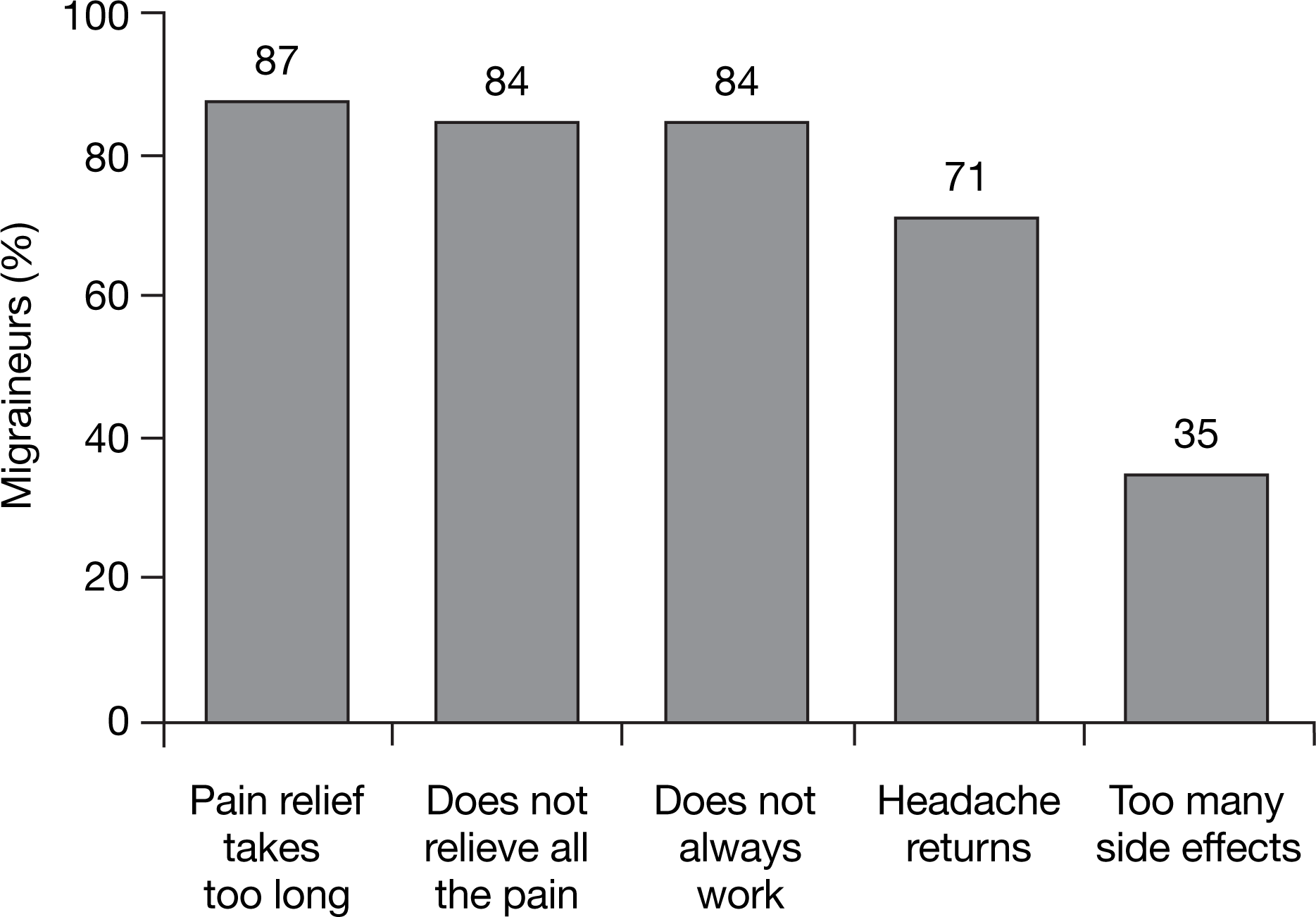
Reasons for dissatisfaction with acute migraine treatment. Reproduced with permission from (21). © 1999, Blackwell Publishing Ltd.
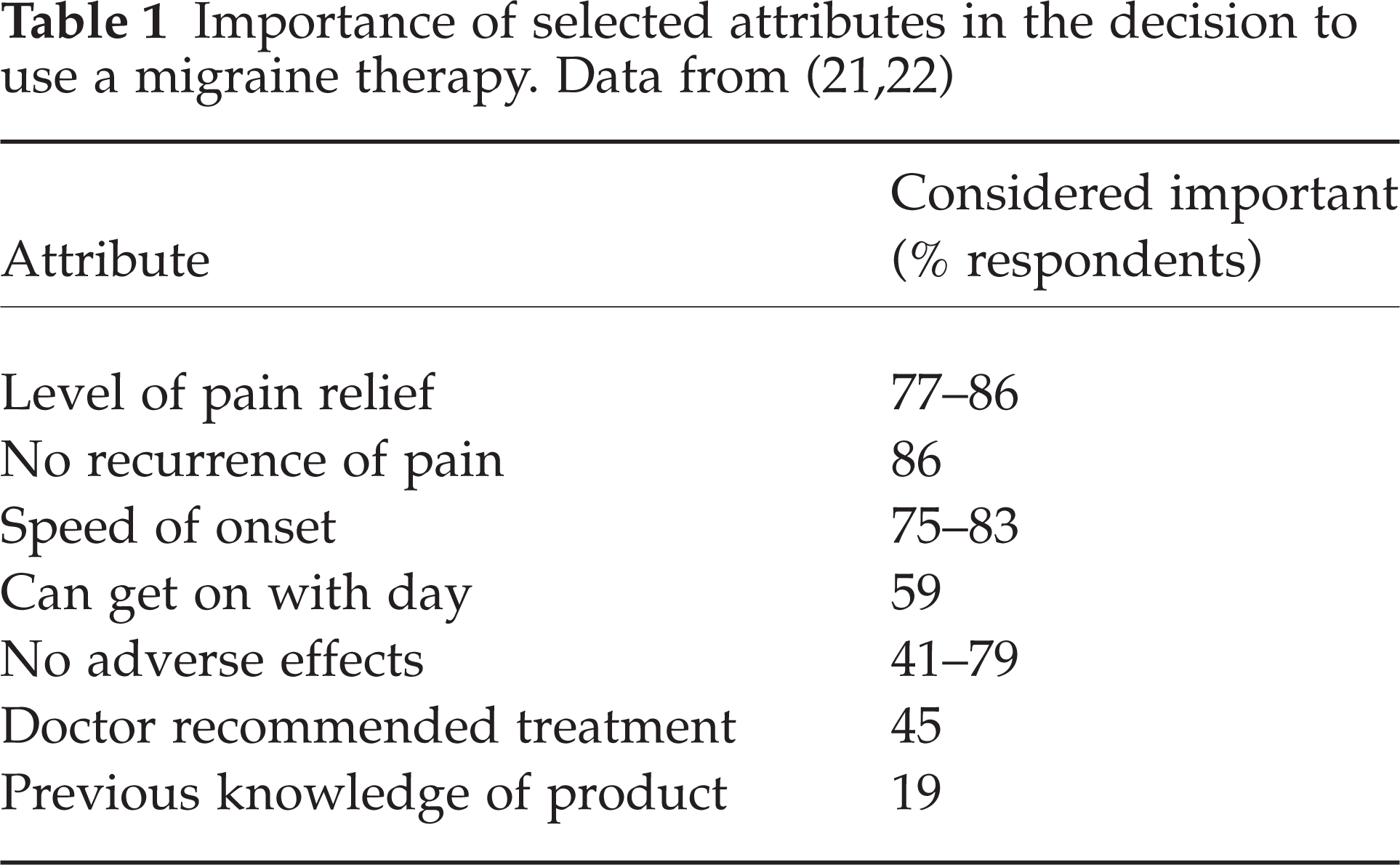
Patients want an acute migraine treatment that brings rapid, complete, sustained and well-tolerated pain relief. This knowledge has been obtained using two methods: patient surveys and analysis of clinical trial endpoints. In two independent surveys of migraineurs, respondents rated complete relief of pain, no recurrence of pain, rapid onset of pain relief and lack of adverse effects as the most important attributes of an acute migraine therapy (21,22) (Table 1).
Residual pain after acute treatment is inversely correlated with treatment satisfaction. Data from two clinical studies have shown that in patients who were pain-free at 2 h, more than 90% of patients were at least ‘somewhat satisfied’ with treatment. In those with remaining mild pain at 2 h after treatment, 60–70% were satisfied to any degree with their medication and for those with moderate or severe pain at 2 h, only 10% achieved satisfaction. These data have important implications for the clinical relevance of the headache ‘response’ endpoint, which has commonly been used to compare the efficacy of migraine treatment in clinical trials. Using this endpoint, a treatment may be considered effective if the severity of pain decreases from moderate to severe to mild or no pain. However, the residual pain, although mild, leaves a significant proportion of patients unsatisfied (23). Another study has confirmed this, with 84% of patients citing residual pain as a reason for dissatisfaction with their migraine medication (21). The IHS has recognized this, recommending that the endpoint of pain-free efficacy is used in preference to pain relief to compare acute migraine treatments in clinical trials (24).
A series of surveys asked patients, neurologists and primary care physicians to rate for an oral, acute migraine treatment the relative importance of efficacy, tolerability and consistency of effect. All groups identified efficacy as the most important attribute for therapy. Half of all patients identified pain-free at 1 h as the most important efficacy endpoint, while one third identified sustained pain-free efficacy as most important. As a composite measure of both pain-free efficacy at 2 h and lack of moderate or severe headache recurrence over 24 h postdose, sustained pain-free efficacy is meaningful for patients as it measures the ability of a treatment to remove pain and keep it away. Interestingly, patients in the surveys rated tolerability more highly than the physicians did (25–27).
Treatment tolerability has particular relevance for a patient, as associated adverse events can affect how a patient uses their treatment. Early treatment within an attack has been associated with improved efficacy, but a recent survey of the current self-medication behaviour of 1160 migraineurs has revealed that concern over adverse events from prescription medications can cause patients to delay or avoid taking their treatment, thus forfeiting the opportunity for optimal outcomes (22). In this group, 22% were currently taking sumatriptan, 20% were taking non-steroidal anti-inflammatory drugs (NSAIDs)/analgesics/opioids, 16% were taking butalbital combinations, while 8% were taking triptans other than sumatriptan and 4% were being treated with ergotamine combination products. Of those currently taking prescription medications, 16% reported regularly experiencing adverse events. One in three (37%) respondents had experienced adverse events with their current or past prescription medication for migraine. The most common adverse event with a triptan was ‘fast heartbeat’ (24%), ‘warm sensations’ (17%), and ‘chest symptoms’ (14%). With non-triptan medications, the most common adverse events were ‘tiredness’ (69%), and ‘difficulty in thinking clearly’ (35%). Although 37% of migraineurs had experienced prescription medication-related adverse events in the past, a much larger number (67%) reported that they had delayed or avoided taking their current treatment due to concerns about adverse events. Sufferers of severe headaches, in whom headache-related disability would be higher, were more likely to miss out on early treatment, with 74% reporting that they delay or avoid taking their current treatment due to concerns over adverse events. Overall, prescription medications were taken early during an attack only 60% of the time by these study participants. In addition, for prescriptions that were left unfilled, concern about tolerability was cited as the reason in 30% of cases. The impact of delaying or avoiding prescription treatment was evident through the high rates of resultant pain and disability: 60% of patients reported more intense pain, 59% suffered a longer duration of pain and the same number needed to lie down during their attack (22).
The tolerability of a migraine treatment clearly affects patient confidence in their treatment and their self-medicating behaviour. Delaying or avoiding treatment has implications for the ability of treatment to reduce attack severity and duration and related disability. Furthermore, understanding the difference between tolerability and safety is important. Tolerability refers to the proportion of clinically unimportant but bothersome events associated with a treatment, while the safety profile is a measure of medically important events. The triptans differ from one another in their tolerability profiles but not in terms of safety. A triptan with a low rate of adverse events, or a placebo-like tolerability profile, may promote patient confidence in therapy and encourage better compliance and appropriate early intervention.
Role of triptans in acute migraine treatment
The efficacy of triptans in the acute treatment of migraine is well established. Triptans are able to rapidly reduce or eliminate pain in a large proportion of patients, and prevent headache recurrence. In addition, in patients with severe migraine, the use of a triptan during acute attacks may improve functioning (6,28).
When an acute attack occurs, rapid achievement of therapeutic levels of an effective triptan can modify the attack if administered soon after the onset of pain. However, there are significant differences between the triptans in their pharmacokinetic profiles, for example in speed of onset and duration of action, which affects their relative efficacy profiles and therefore has implications for choice of agent when individualizing therapy (29,30). A meta-analysis of triptan clinical trial data found small but clinically relevant differences in efficacy (pain-free status and recurrence of headache), tolerability and consistency of effect between the seven commercially available triptans (31). The meta-analysis identified almotriptan 12.5 mg, eletriptan 80 mg and rizatriptan 10 mg as the three agents most likely to be associated with treatment success.
Despite the wide availability of triptans, and the knowledge of their efficacy in migraine treatment, only a relatively small proportion of patients are being treated with these agents (15). Results from the American Headache Study showed that in 1989, the majority of migraine sufferers (59%) used over-the-counter (OTC) medications alone to treat their attacks; in 1999, this value had dropped by only 2% to 57%. In 1989, over a third of patients (37%) used only prescription products, and this figure rose to 41% in 1999. Only a small number of patients (4% in 1989 and 2% in 1999) used no medication (15). A similar survey, conducted in 1999, found that about half (55%) of migraineurs used both prescription and OTC medications (22). A further study examined which prescription medications were routinely used for treating migraine in the US, Italy, Germany, France and the UK (12). The most frequently used medications were simple analgesics, ranging from 22% in France to 54% in Italy, followed by NSAIDs (5% in the UK to 43% in Italy) (Fig. 5) (12). The average rate of triptan use was 10%, with the lowest rate in Italy (3%) and the highest rate in the US (19%). These results therefore show that a variation exists in global treatment strategies for migraine, but triptan use remains relatively low. This failure to provide migraine-specific therapy might be a contributing factor to the dissatisfaction with therapy and lapsing from care reported in this patient population.

Patterns of migraine medication use in key countries. Reproduced with permission from (12). © 2003, Blackwell Publishing Ltd.
Management strategies to prevent progression
Management of migraine can be considered from two perspectives: halting progression within an attack and halting progression of the disease itself. Within an acute migraine attack, the development of central sensitization (and cutaneous allodynia), once peripheral sensitization has occurred, is associated with triptan refractoriness. This phenomenon occurs usually within 60 min of the onset of headache; therefore, treatment should be initiated prior to this time, allowing therapeutic levels of the triptan to be achieved to prevent central sensitization from occurring, and thus modifying the progression of the attack.
As discussed previously, in some patients the disease can be progressive. A sign of disease progression is when the individual changes from having a mild condition to suffering frequent, severe, repeated attacks, and this evolution is manifested by measurable changes in the brain. In some instances, episodic migraine can transform to chronic daily headache associated with severe disability. Potential strategies for limiting the progression of the disease in the individual include instigating attack modification using early intervention, modifying risk factors, and applying preventative treatment.
Central sensitization that occurs in migraine attacks is also seen in chronic daily headache. Hence, preventing the development of central sensitization via attack modification may also reduce the risk of patients developing chronic daily headache (1).
There are several modifiable risk factors associated with migraine. Risk factors or ‘triggers’ promoting acute attacks can be broadly classified into food (e.g. chocolate, caffeine), behavioural (e.g. stress, fatigue) and environmental factors (e.g. loud noises, pollution). Risk can be modified by identifying the individual's specific migraine triggers and changing behaviour in order to avoid these factors (32). Cognitive, emotional and behavioural factors all contribute to headache-related disability. Over time, frequent and severe attacks can lead to further disability as a result of maladaptive coping techniques, self-defeating illness beliefs, anticipatory anxiety about upcoming attacks and psychological morbidity such as depression. Repeated migraine attacks can be a risk factor for the progression of the disease, as they may change the antinociceptive capability of the trigeminovascular system, favouring the processing or generation of more attacks (3). Treatment-related complications, such as medication overuse, also contribute to morbidity and disease progression in many patients. Therefore, counselling to reverse these behaviours may be a beneficial adjunct to modifying the disease process (6). In addition, acute therapy should be limited to no more than two times per week to prevent medication overuse headache, which has a pattern of increasing headache frequency, often resulting in daily headaches. In patients with suspected medication overuse or patients at risk of medication overuse, preventative migraine therapy should be considered.
Preventative treatment is indicated when a patient experiences two or more attacks per month that produce long lasting disability lasting ≥ 3 days per month; where there is contraindication to, or failure of, acute treatments; or where patients use acute medications more than twice a week (32).
Treatment leading to reductions in attack frequency and severity should correlate with reduced disability and a decrease in central nervous system changes. Over a lifetime, the cumulative effect of shorter attacks, reduced periods of enforced inactivity, improved cognition and decreased anxiety associated with the effective treatment of individual attacks should result in decreased disability. Consequently, aggressive therapy might be indicated once a patient has demonstrated migraine progression but before daily headache develops. However, controlled long-term studies are required to test this hypothesis. By delaying or preventing loss of work, reduced family or social roles, as well as illness-related behavioural and psychological pathology, such treatments may have a protective effect on disease progression in migraine (6).
Summary
Migraine is a condition in which the majority of sufferers report severe pain and disability. However, migraine remains underdiagnosed and undertreated. Patient expectations from therapy have increased, yet these expectations still differ from those of physicians. Patients now expect an acute treatment to provide complete pain relief to reduce their migraine-related disability and return their normal level of functioning. Patients also expect rapid and sustained pain relief, and want a medication with a good tolerability profile. Understanding patients’ preferences may be a key to improving compliance and achieving long-term therapeutic success, for example allaying fears of adverse events that can cause them to delay treatment beyond the critical early period, and using a medication with an excellent tolerability profile.
Evidence indicates that there is a pattern of progression within acute migraine attacks that culminates with the development of sensitization. In addition, in some patients there appears to be a pattern of progression of the disease, characterized by an increase in attack frequency, intensity, duration and accompanying disability. Prevention of disease progression in high-risk individuals is required to limit the burden of future pain and disability.