
Abstract
During the past few years, several surveys have highlighted the high prevalence of migraine amongst the general French population and the large healthcare burden associated with suboptimal treatment. Since it opened, the Centre d'Urgences Céphalées (EHC) has treated more than 55 000 patients, the majority of whom were suffering from migraine. Expert diagnosis of the type and causes of the headache, followed by immediate medication, allows patient stabilization. Detailed assessments can then determine the most appropriate treatment for each patient to improve outcomes and reduce the necessity for further emergency admissions. Triptans are generally recommended, and for those patients who currently have ineffective migraine control with one triptan, individual evaluation allows prescription of an alternative triptan which will better suit their needs. Follow-up is crucial to ensure that treatment remains optimal and that patient expectations are being met. Although a minority of patients with severe headache will continue to require repeated emergency treatment, more than 90% of patients seen at the EHC can be successfully managed with this combination of accurate diagnosis, effective treatment and individualized follow-up care.
Introduction
Several epidemiological surveys have been carried out to evaluate the prevalence, impact and management of migraine in France. The first survey was carried out in 1989; using the International Headache Society (IHS) classification scheme [International Classification of Headache Disorders (ICHD)], the prevalence of migraine was estimated to be 8% (1). Subsequent surveys, in 1999 and 2000, have also highlighted the high prevalence of migraine in France, as well as its detrimental impact on patients (2–4).
Migraine is also a burden on healthcare resources, and this is not limited to the community setting. Studies carried out during the 1990s estimated that approximately 2% of patients presenting at an emergency department had migraine as their chief complaint (5, 6). However, treatment of migraine in the general emergency setting can be variable (7), and it has been suggested that this may reflect, at least in part, emergency physicians' lack of experience with ICHD (8).
The Centre d'Urgences Céphalées (EHC) was opened in Paris in September 2000. It is staffed by neurologists and provides a devoted emergency service for patients with headache, aiming to improve assessment and management and minimize the debilitating effects on patients.
Centre d'Urgences Céphalées
The EHC is based at Hôpital Lariboisière in Paris. The hospital, which has the largest emergency department in Paris, also comprises several departments that complement the service provided by the EHC; these include neuroradiology, neurology, ophthalmology, ear, nose and throat, and pain and headache clinics. When the EHC opened, it was predicted to receive 2000 patients per year; the actual number is closer to 8000, with > 55 000 patients overall having received consultations since 2000. In 2007, we have seen 8200 patients at the EHC.
The centre is open 6 days a week (Monday to Saturday) and receives, on average, approximately 600 patients per month, although there is some variation according to the time of year; for example, September and October are busier than December and February. Patient numbers also vary according to the day of the week; average patient numbers on a Monday are 60, compared with 15 on Saturdays.
The clinical profile of migraine patients attending the centre has been evaluated in a prospective study in 50 patients (Table 1). Young women predominated and 86% of patients were aware that they had migraine; this is high compared with the general migraine population in France (40%) (9). This is an important observation, because patients who are self-aware use recommended (and more effective) treatments for migraine more frequently than those who are not self-aware (9). Those who were not aware were younger (29.1 vs. 33.6 years), had a much shorter duration of migraine history (4.4 vs. 15.6 years), had consulted fewer physicians for headache (1.0 vs. 2.3), and were not receiving regular medical follow-up (0% vs. 58%). Only one-quarter of the EHC patients were referred by a physician. One-third were advised about the centre by a family member, friend or pharmacist, and one-third were made aware of the centre by the media; the remainder lived near the hospital.
Clinical profile of migraine patients presenting at the Centre d'Urgences Céphalées (n = 50)
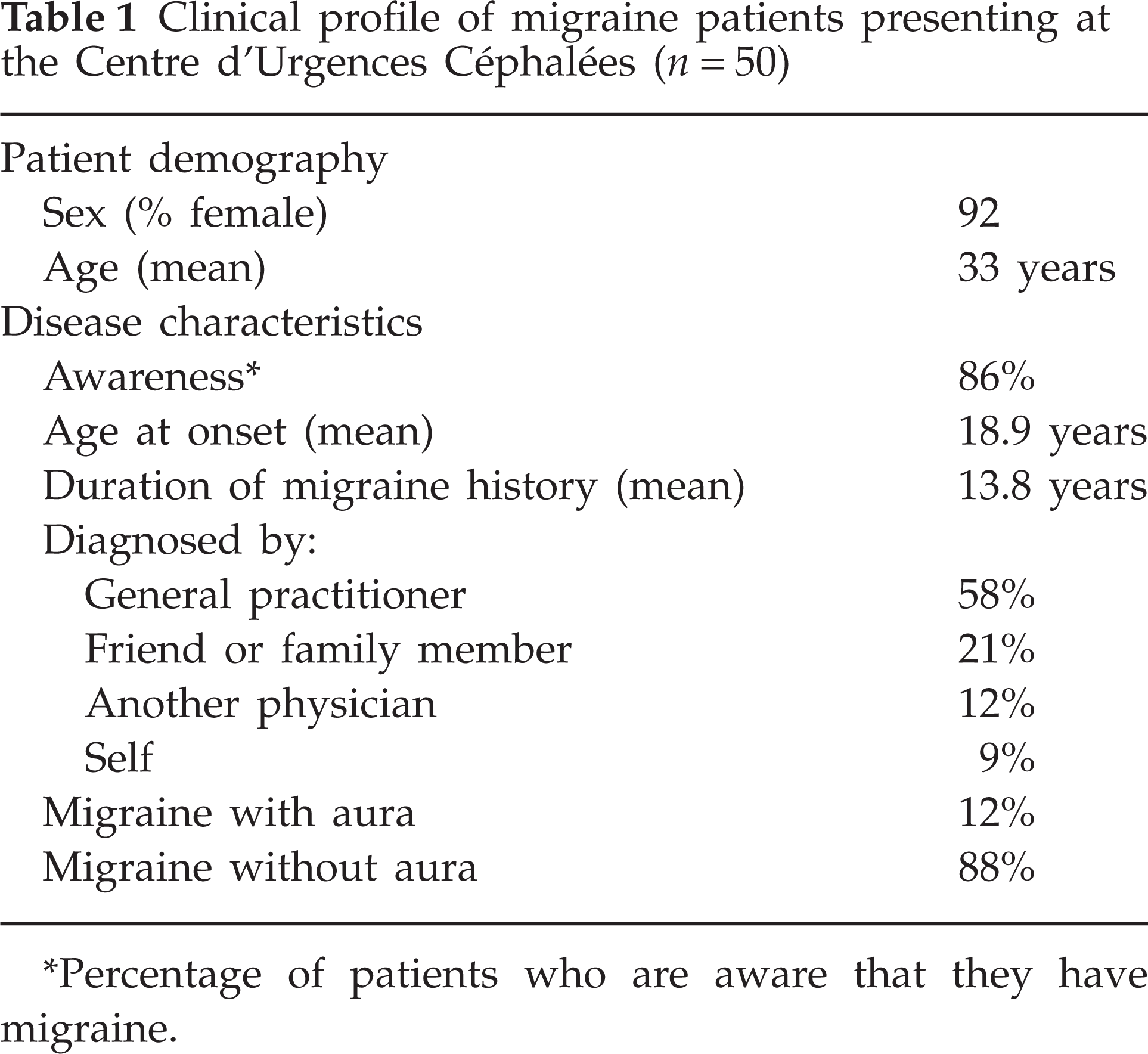
Percentage of patients who are aware that they have migraine.
The study also evaluated patients' reasons for attending the centre. Most patients attended because of a recent increase in the frequency of migraine attacks. However, migraine severity was also an important reason, particularly if it resulted in the need for the patient to take multiple medications or the inability to resume activities. The need to obtain a clear diagnosis was the reason for attending in only a small percentage of patients, probably reflecting the high self-awareness in this group of patients.
In terms of current medication at presentation to the EHC, 26 patients (52%) were receiving triptans for their migraine. This was high compared with the estimated 8–10% of the general migraine population in France who are treated with triptans (Fig. 1) (9). However, it was notable that in the group of EHC patients, triptan use was much higher in patients who were aware of their condition than in those who were not (58% vs. 14%, respectively). No patients in the non-aware group received preventative treatment, compared with six (14%) of patients who were aware.

Migraine medications used by the French migraine population (9) and in patients presenting at the Centre d'Urgences Céphalées (EHC).
Patient satisfaction with their current medication was also assessed, using a questionnaire developed by the French medicoeconomic evaluation service (ANAES) (10). The ANAES consists of four questions to evaluate pain relief at 2 h, medication tolerability, ability to resume activities, and the need for rescue medication. Compared with the overall French migraine population, those attending the EHC were less satisfied with their current migraine medication (Fig. 2) (9). In the group of EHC patients, of those who did not achieve significant pain relief at 2 h, 65% were taking analgesics, non-steroidal anti-inflammatory drugs (NSAIDs) or a combination of these, and 35% were taking triptans. In the overall French population, 65% of patients taking recommended migraine medication (triptans, ergotamines, NSAIDs, aspirin ± metoclopramide) were entirely satisfied, compared with 56% taking non-recommended medication (opioids, paracetamol, fixed combinations of simple analgesics and opioids, barbiturates and/or caffeine) (P < 0.01) (9). In addition, significantly more patients reported complete satisfaction with triptans (72%) compared with paracetamol (57%) or opioids (51%) (P < 0.01 for both) (9).

Satisfaction with migraine treatment in the French migraine population (9) and patients presenting at the Centre d'Urgences Céphalées (EHC).
Clinical care in the Centre d'Urgences Céphalées
A three-step approach is used to manage patients attending the EHC: diagnosis, treatment and orientation.
Diagnosis
Accurate diagnosis is crucial, as this drives subsequent management and follow-up of patients. However, studies have shown that patients with headache presenting at emergency departments are subject to inaccurate or non-specific diagnosis (8, 11, 12). It has been suggested that this is due, in part, to emergency physicians' lack of knowledge of the diagnosis criteria of the IHS for primary headaches, especially for migraine without aura (8).
At the EHC, precise diagnosis is a top priority, and, in particular, identifying patients with serious secondary headaches. Staff conduct an interview with each patient, a step that is considered pivotal in the diagnostic process. Questions are designed to establish the nature of the headache onset (sudden/explosive or progressive) and its pattern (usual/chronic or unusual/acute), as well as to highlight patients who require further investigation, the latter involving about one-quarter of patients who attend the EHC. Diagnosis is made according to the following categories: primary headaches (migraine and other headaches), benign secondary headaches (e.g. due to influenza or sinusitis) and serious secondary headaches (e.g. due to intracranial hypertension or subarachnoid haemorrhage).
Most patients attending the centre (77%) have primary headaches, and migraine is the single biggest cause, accounting for 42% of all patients. Other primary headaches include tension-type headache, cluster headache and other trigeminal autonomic cephalalgias. Secondary headache disorders are diagnosed in about 14% of patients. Cranial neuralgias are rare (< 1.5%). In a small proportion of patients (8%), no precise diagnosis can be made; these patients are designated as having an ‘unclassified headache’ according to item 14.2 of ICHD-II.
Treatment
Having established a diagnosis, the next key objective for staff at the EHC is to treat the pain, using abortive treatment and/or enhancement of current therapy. The parenteral route is preferred, as patients are often vomiting at the time of admission. In patients with severe migraine, first-line treatment is subcutaneous administration of sumatriptan, provided that the patient has not taken an oral triptan in the preceding few hours. The remaining patients receive an i.v. infusion of proparacetamol (acetaminophen) and metoclopramide, often in combination with the benzodiazepine, chlorazepate, to treat anxiety. Collectively, these actions lead to an improvement in > 80% of patients. In those with resistant attacks, an additional i.v. injection of aspirin, ketoprofen or nefopam is given. Under certain circumstances, (e.g. in pregnant women), oxygen or proparacetamol are used.
Patient orientation and follow-up
In the final step of the management process at the EHC, staff evaluate patients' current treatment strategies, with a view to improving future treatment. On discharge, and in accordance with French treatment guidelines (10), patients are prescribed a combination of an NSAID and a triptan as first-line abortive treatment of future attacks, and advised to take the medication as soon as possible after the onset of migraine (10). For patients who are already taking triptans but gaining suboptimal control, staff evaluate the characteristics of the migraine and prescribe an alternative triptan that better suits the patient's needs. Patients are generally unaware that if their usual triptan stops working, another agent may be effective. In addition, primary care physicians generally do not change the triptan if it becomes non-efficacious.
Only 3–4% of patients attending the EHC are hospitalized; most are managed as out-patients. For this reason, a patient follow-up plan is also considered a crucial part of the management process. Follow-up is provided at the hospital's headache clinic for about 2500 patients per year, with the aim of evaluating the efficacy of discharge medication and the need for preventative medication. The remainder of patients are advised to seek follow-up through their primary care physician or a neurologist. This is important, because an estimated 80% of the French migraine population do not receive medical follow-up (9). Furthermore, it has been shown that if headache patients receive follow-up at a specialist headache clinic, there is a reduction in the number of repeat visits to the emergency department (13).
Patients at the EHC are also provided with a migraine diary to complete. This is also consistent with the French guidelines, as a patient keeping a diary helps the physician to determine migraine severity and evaluate the effects the headache has on activities of daily living, and assists in the choice of treatment and the type of follow-up measures required.
Conclusions
An estimated 2% of all visits to general emergency departments are made by patients with migraine, and a significant proportion make repeated visits. In part, this reflects suboptimal management in the community setting, resulting in an increased burden on secondary and tertiary services (14, 15). However, a minority of migraine patients, whose headache is sufficiently severe, will continue to require emergency treatment.
The EHC was established in Paris in September 2000 as a devoted service for patients with headache. Since its inception, > 55 000 patients have attended the EHC, with migraine representing the single most common reason for attending. As well as providing expert diagnosis and stabilizing medication, one of the key aims of the EHC is to ensure that patients receive appropriate long-term follow-up and treatment. The repeat-visit rate for the centre is only 6–7%, attesting to the success of this integrated, specialized service.
Footnotes
Competing interests
A.D. has received speaker's fees from Almirall, AstraZeneca, GlaxoSmithKline and Pfizer.
Acknowledgements
The author would like to thank Nicola French PhD, from Complete Medical Communications, who provided medical writing support funded by Almirall.