
Abstract
The majority of the patients who seek medical care in tertiary headache centres present with transformed migraine, and convert to daily headache, as a result of excessive intake of symptomatic medications (SM). This study aimed to analyse the possibility of using a short course of oral prednisone for detoxifying patients with chronic daily headache due to medication overuse in an out-patient setting. Four hundred patients with headache occurring more than 28 days per month for longer than 6 months were studied (mean baseline frequency of 0.96). Symptomatic medications were stopped suddenly and prednisone was initiated in tapering doses during 6 days, followed by the introduction of preventive treatment. Withdrawal symptoms and the frequency, intensity and duration of the headache, as well as the consumption of rescue medications, were analysed during the first 16 and 30 days of withdrawal. Eighty-five percent of the patients experienced a reduction in headache frequency and no patients presented severe attacks during the first 6 days. With regard to the following 10 days, 46% of the patients experienced at least 2 days without headache and 58% less intense attacks. Most of the patients noticed attacks with longer duration. After the 30-day period there was a significant decrease in headache frequency (mean 0.83, P < 0.001), and no patients returned to overuse of SM. This study demonstrates that it is possible to detoxify patients suffering from rebound headaches, using oral prednisone during the first days of withdrawal, in an out-patient setting.
Introduction
The prevalence of daily headache is high as 5% of the adult population (1). In headache clinics, daily headache sufferers represent more than 35% of the patients that seek help (2). Patients with episodic migraine may gradually develop a pattern of daily or almost daily headache, losing migraine features and presenting characteristics resembling those of the chronic tension-type headache (3, 4). The conversion to a modified pattern of migraine is known as transformed migraine (5). Among transformed migraine patients, over 80% have converted to the daily pattern and maintained it as a result of the overuse of medications taken to relieve headache or symptoms (6), therefore changing the episodic pattern into a transformed migraine one (7–9). The mechanisms by which the overuse of symptomatic medications (SM) play a role in this transformation are uncertain. Srikiatkhachorn & Anthony (10) emphasize that patients with drug-induced daily headache present a higher concentration of 5-HT2 receptors in platelet membranes compared with episodic migraine patients, suggesting that this could be found in central serotonergic receptors as well, and explain the transformation of episodic migraine into daily headache associated with overuse of drugs. Bowdler et al. (11) and Lance et al. (12) suggest that patients with primary headaches, especially migraine, develop a pattern of daily headache in the presence of various kinds of SM overuse. These authors point to the fact that a higher suppression, induced by the SM, over an already deficient anti-nociceptive system may play a role in this pattern of transformation. Srikiatkhachorn et al. (13) suggest that the excessive use of SM could lead to an up-regulation of central serotonergic receptors, suppressing therefore the function of serotonergic pathways involved in central pain modulation. Hering et al. observed an increase in blood level of serotonin after withdrawal of overused SM in chronic daily headache patients (14), and analysed the platelet membrane transduction of patients with daily headache, suggesting that the overuse of SM would result in a modification of this process, possibly playing a role in such a headache pattern modification (15).
In order to restore the episodic pattern of migraine and allow the preventive treatment to be effective, it is imperative that the overused medications be withdrawn, which may create rebound and withdrawal reactions (7). Mathew et al. (16), studying a group of 200 patients taking daily symptomatic medications, observed initial withdrawal reactions, commonly in the first 4 days, that included nervousness, increased headache, nausea, vomiting, insomnia, diarrhoea and tremor in most of the patients. Dichgans et al. (17) also observed withdrawal symptoms after abrupt discontinuation of mixed analgesics in 52 patients. The withdrawal symptoms may persist for up to 2–3 weeks (16, 18) along with the exacerbation of the headache, therefore requiring hospitalization, which was the standardized treatment in the past (19).
Drug-induced daily headache and the so-called rebound headache are characterized by the regular, dependable and predictable development of a headache, within hours of the waning therapeutic effect of the last dose of medication, therefore creating a refractory headache cycle (20).
To approach these patients more efficiently, in addition to the clear understanding of the role the abused medications play in causing the daily headache, it is important that the rebound-causing medications be withdrawn. Sometimes however, the process of detoxification from these substances may be extremely uncomfortable for patients and frustrating for the physician since withdrawal reactions and worsening of headache frequently occur (7, 16, 17).
There are proposed methods of restoring the episodic pattern of migraine: ceasing abruptly all rebound-causing medications, administering intravenous dihydroergotamine (DHE) during a period in the Hospital (21) and repetitive use of oral sumatriptan in an out-patient setting (7). These two options represent a bridge to detoxification during withdrawal of symptomatic medications (7, 21, 22). The substitution of the overused substances by a long-acting non-steroidal anti-inflammatory drug (NSAID) or the use of intramuscular DHE or corticosteroids, for those with an abrupt discontinuation, are also suggested for the out-patient setting (18).
For some patients, a period in the Hospital is not affordable or even possible, and some others consistently do not respond to the use of oral sumatriptan even for the acute treatment of migraine attacks (23). Besides, the use of injectable medications in an out-patient setting or simply the substitution of one symptomatic medication for another, may not be recommended for patients that already are psychologically and physically dependent on the chronic use of symptomatic drugs.
This study was undertaken to determine whether the use of a short course of prednisone, an oral corticosteroid, could be useful as an out-patient option for detoxification, reducing withdrawal symptoms and headache intensification, obviating the need for Hospitalization.
Patients and methods
Four hundred patients, 318 women and 82 men, aged 19–64 years (mean 38 years) (Table 1), from a tertiary headache centre were sequentially selected and prospectively studied. All presented with headache for > 28 days per month (Table 2) for longer than 6 months, meeting the proposed criteria of Silberstein et al. for transformed migraine with medication overuse (9). The mean baseline headache frequency (calculated considering the number of headache days divided per 30-day period of each patient and taking into account the mean number for all 400 patients) was 0.96 (
Temporal characteristics of daily headache patients

Frequency of headache

Pattern of overused medications

Pirazolonic derivative.
May include other formulations (such as injectable and nasal spray).
Frequency and percentages of comorbid sleep and emotional disturbances

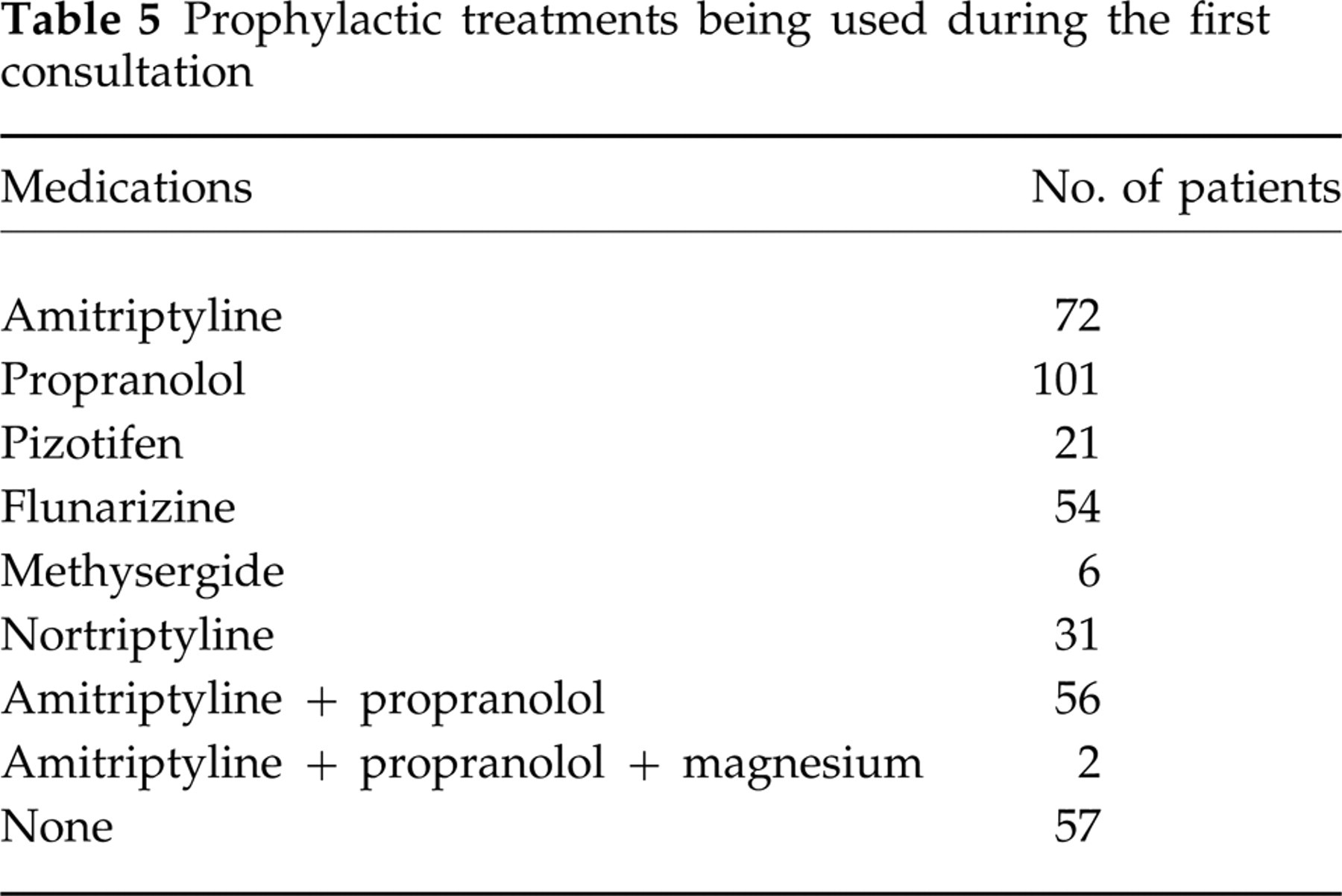
Prophylactic treatments being used during the first consultation
Prophylactic treatments after withdrawal

Results
During the first 6 days of treatment, on prednisone, 340 patients (85%) noticed a reduction in frequency, experiencing at least 2 days without headache, mainly from the third or fourth days on. One hundred and forty patients (35%) had experienced mild to moderate attacks and 260 patients (65%) moderate or moderate to severe attacks. Forty-six patients (11.5%) noticed a shortened duration of headache episodes (< 4 h) while 354 patients (88.5%) reported longer-lasting attacks, some longer than 24 h (average 8–12 h). None of the patients presented severe attacks requiring bed rest, and none consumed any type of symptomatic or rescue medication. With regard to the following 10 days, with patients off prednisone and under various types of preventive medications (Table 6), 184 patients (46%) observed reduced frequency with at least 2 days with no headache. Two hundred and thirty-two patients (58%) reported experiencing moderate or moderate to severe attacks. During the second time period, again none of the patients presented severe attacks requiring bed rest or used symptomatic medications.
Withdrawal symptoms, including nervousness, nausea, vomiting, insomnia, diarrhoea and mild tremor, were reported by 48 (12%) patients during the first 16 days.
After the 30-day period, the mean headache frequency (calculated considering the number of headache days divided per 30-day period of each patient and taking into account the mean number for all 400 patients) was 0.83 (
During the 30-day study period, none of the 400 patients developed fever, myalgias, arthralgias, malaise, increased intracranial pressure with papilledema or large joints pain, or consumed any type of symptomatic medications.
Discussion
Although this study was not randomized or blinded, it did demonstrate that the patients were able to be detoxified in an out-patient setting, avoiding the time, costs and difficulties related to hospitalization. Most of the patients habituated to substances like ergotamine and caffeine may present after withdrawal, nausea, vomiting, agitation, restlessness, sleep disorder, depression and even seizures during detoxification (16). Only 12% of the patients presented withdrawal symptoms, and none of them seizures.
The absence of headache during 2 days in the first 6-day period occurring in 85% of the patients does not necessarily imply headache improvement, since the baseline frequency was 28/30-day period. However, if we consider the baseline mean headache frequency (0.96) and compare it with the end of treatment mean headache frequency (0.83), there was a significant frequency reduction (P < 0.001). With regard to the intensity, even though there was an increase in the mean headache intensity from the baseline period compared with that of the end of treatment, none of the patients returned to the daily consumption of symptomatic medications or even used rescue medications. Diener et al. (24) observed that analgesic-induced daily headache patients may return overusing SM due to the escalation of headache intensity after withdrawal.
The mean duration of the headache during the first days of detoxification and at the end of the 30-day period was longer than the baseline period, which was probably due to the prohibition of taking SM. However, the fact that patients did not present severe attacks may have contributed to the lack of consuming rescue medications and to the success of the detoxification of our 400 patients on an out-patient basis. Diener et al. (25) were able to detoxify successfully only 1.5% of 200 patients on an out-patient basis. Silberstein & Lipton (18), based on experience of many clinicians, suggested that the detoxification process may require hospitalization and can last up to 2 weeks.
Steroids has been suggested to terminate the refractory headache cycle observed in rebound (22, 26) and for the acute treatment of headache as well (27–29). Dexamethasone given intravenously at a dose of 6 mg following the i.v. administration of metoclopramide, was demonstrated to be effective in the acute treatment of a migraine attack (28). Gallagher (27) suggests a combination of dexamethasone and narcotics to provide additional relief. With regard to ‘status migranosus’, a state of intractable debilitating pain, often arising from a setting in which the patient becomes dependent on SM (30, 31), the headache may last for several days. The patients may present with consequent exhaustion, depression and even de-hydration (when there has been vomiting). In this condition, the usefulness of steroids, especially prednisone 40–60 mg/day for 1 or 2 days, appears to shorten dramatically the course of ‘status migranosus’ (32). To break the cycle of rebound headache, Silberstein & Saper (20) also suggested the use of i.v. or i.m. dexamethasone, starting at a dose of 8–20 mg/day in divided doses, rapidly tapering over 2–3 days. Intravenous hydrocortisone can be used in the following tapering manner: 100 mg via a saline ‘drip’ over 10 min every 6 h for 24 h; every 8 h for 24 h; every 12 h for 24 h; and then a final dose. Silberstein & Lipton (18) suggested the i.m. use of steroids for those out-patients that abruptly discontinued overused medications. Saper (33) and Silberstein et al. (22) emphasize that oral steroids also can assist in terminating an otherwise refractory migraine.
The mechanisms by which steroids are useful in headache are uncertain (32, 34). Steroids affect neuronal activity and steroids produced locally in the brain (neurosteroids) may regulate neuronal excitability (35). Edmeads (32) suggests that the anti-inflammatory effect of steroids may be the mechanism of action in treatment of ‘status migranosus’, which may be mediated through reduction of oedematous artery walls, blocking of histamine and sensitization of arterial smooth muscle to catecholamines. In fact, steroids can prevent or suppress inflammation in response to multiple inciting events, including radiant, mechanical, chemical, infectious, and immunological stimuli. Steroids inhibit the production by multiple cells of substances that are critical in generating the inflammatory response. As a result, there is decreased release of vasoactive and chemoattractive factors, diminished secretion of lipolytic and proteolytic enzymes, decreased extravasation of leucocytes to areas of injury, and ultimately, decreased fibrosis. The net effect of these actions on various cell types is to diminish markedly the inflammatory response (36). Saper et al. (34) proposed the following possible mechanisms on headache: anti-inflammatory effect on neurogenic inflammation, reduction of vasogenic oedema and effects on central aminergic/serotonergic mechanisms. The proposed mechanisms make the steroids recommended not only for cluster headache and headaches associated with increased intracranial pressure/oedema, but also for intractable migraine, in a short-term ‘tapering’ course of oral preparations. Steroids can be used in circumstances in which other appropriate agents have failed or are contraindicated. Patients with severe, acute and protracted conditions may also benefit from their use (34).
With regard to toxicity, two categories of toxic effects result from the therapeutic use of steroids: those resulting from withdrawal of steroid therapy and those resulting from continued use of supraphysiological doses (36). Sullivan (37) pointed to several complications associated with steroid withdrawal. The most severe is acute adrenal insufficiency which results from too rapid withdrawal of steroids after prolonged therapy. In addition, a milder characteristic steroid withdrawal syndrome consisting of fever, myalgias, arthralgias, and malaise may happen after short-term use of steroids. Pseudotumour cerebri, a clinical syndrome that includes increased intracranial pressure with papilledema, is also associated, rarely however, with the reduction or withdrawal of steroids. The patients in our study were advised to observe unusual symptoms, and at follow up after 30 days none of the 400 patients related any of the manifestations suggesting the described syndromes.
Aseptic necrosis of bone (osteonecrosis) may complicate long-term therapy with steroids and also has been occasionally reported following short courses with high-dose therapy (36). Large joints may be affected, and the femoral head is the most frequently involved, provoking joint pain and stiffness as early symptoms, but progressing to the point that joint replacement is required (38). Among our treated patients and during the period comprising the first 30 days after withdrawal, none of them reported any symptoms affecting joints.
Our use of prednisone to assist in withdrawal, providing a significant decrease in frequency, lack of withdrawal symptoms in the majority of the patients and not allowing an intense escalation of headache intensity, enabled our patients to avoid not only hospitalization, but also the substitution of one potentially rebound-causing medication for another. Studies have shown that rebound headache develops shortly after the suspension of small dosages of ergotamine and analgesics (6, 39, 40, 41), and frequently patients fail to withdraw completely due to escalation of headache, associated symptoms and consequent incapacitation (42), which was not observed in our patients.
This study was conducted in a private tertiary care centre, which receives ‘end-of-line’ headache patients, who have seen numerous doctors and treatments, without even stopping their overuse of SM. They present with psychological and emotional dependence, low frustration tolerance and sleep disturbances, as also observed in other centres (16, 43, 44). These patients are prone to the development of abstinence syndromes (18) which could have counteracted the previous attempts to withdraw overused medications. We are optimistic about this out-patient approach in treating rebound headache. There is need for a double-blind, randomized, placebo-controlled study with the use of prednisone, as well as the study of its long-term toxicity, long-term efficacy and potential use in wider groups of patients excluded in this series.
Footnotes
Acknowledgements
The authors are grateful for the valuable orientation and revision of the manuscript provided by Drs Alan Rapoport and Fred Sheftell, and for the statistical analysis provided by Dr Luiz Alves PhD.