
Abstract
Occipital nerve stimulation (ONS) may be effective for the treatment of headaches that are recalcitrant to medical therapy. The objective of this study was to determine if response to occipital nerve block (ONB) predicts response to ONS in patients with chronic, medically intractable headaches. We evaluated 15 patients who underwent placement of occipital nerve stimulators for the treatment of chronic headaches. Data were collected regarding analgesic response to ONB and to ONS. Nine of 15 patients were ONS responders (≥50% reduction in headache frequency or severity). Thirteen patients had ONB prior to stimulator implantation. Ten of 13 who had ONB had significant relief of head pain lasting at least 24 h, and three were ONB non-responders. Of the three ONB non-responders, two were ONS responders. Of the two patients who did not have ONB prior to ONS, one was an ONS responder and one was an ONS non-responder. In conclusion, analgesic response to ONB may not be predictive of the therapeutic effect from ONS in patients with medically refractory chronic headaches.
Keywords
Introduction
Occipital nerve stimulation (ONS) is currently under investigation for its use in the treatment of medically recalcitrant headache disorders (1). Small studies have shown the efficacy of ONS for the treatment of occipital neuralgia and chronic migraine. In light of the cost and invasive nature of the procedure, it is essential to identify possible predictors of ONS response. In clinical practice, an occipital nerve block (ONB) with a short-acting local anaesthetic and corticosteroid is often performed prior to considering treatment with an occipital nerve stimulator. However, it is not known whether the analgesic response to ONB predicts headache outcomes after ONS.
Methods
This is an Institutional Review Board-approved retrospective analysis of 15 patients who underwent off-label placement of an occipital nerve stimulator for chronic, medically refractory headache disorders. All potential subjects were evaluated in our headache specialty clinic, by one neurosurgeon who performed all of the procedures and one anaesthesiologist specializing in pain, and all underwent psychiatric evaluation. Headache diagnoses were made according to the criteria of the International Headache Society (IHS) (2).
As part of the pre-ONS evaluation, 13 of 15 patients underwent ONB prior to temporary stimulator placement. Patients underwent ONB at the discretion of the treating physician and the procedure was performed during periods of headache pain in all patients. The rationale for not performing ONB in two of the 15 patients was not clear from the medical record. ONB was accomplished by injecting 3 cm3 of 0.5% bupivacaine mixed with 20 mg (0.5 cm3) methylprednisolone acetate (40 mg/ml) subcutaneously over the expected locations of the greater and lesser occipital nerves. ONB response was defined as a significant reduction (≥50%) in the severity of pain between C2 and the vertex that endured for at least 24 h. Analgesic response to ONB was then correlated with ONS response, as defined below, in order to determine if it predicted ONS outcome.
All subjects underwent a percutaneous stimulator trial lasting 5–7 days, followed by permanent implantation within 1 month. All patients who underwent trial stimulation went on to have permanent ONS placement. Pisces Quad Plus leads and Synergy implantable pulse generators (IPGs) from Medtronic Inc.® (Minneapolis, MN, USA) were used in all subjects. Leads were placed unilaterally or bilaterally according to the subjects' headache location. Patients with exclusive or near-exclusive side-locked hemicrania had unilateral lead placement. Surgical technique was modelled on that described by Weiner (3). Stimulation amplitude and frequency were patient controlled, with subjects instructed to use and adjust their stimulator per effect. Additional acute and prophylactic medications were not prescribed in the peri-implant or immediate post-implant period.
Data regarding IHS headache types, patient demographics and headache frequency, severity and disability pre- and post-ONS placement were collected during follow-up visits and telephone interviews with the aid of headache diaries and Migraine Disability Assessment questionnaires. ONS responders were defined as those with at least a 50% reduction in the frequency or severity of headaches post ONS.
Results
Fifteen patients underwent placement of occipital nerve stimulators for the treatment of chronic headaches. Subjects' ages ranged from 21 to 52 years with a mean of 39 years. There were 12 females and three males. Eight patients met IHS diagnostic criteria for chronic migraine, three for chronic cluster, two for hemicrania continua and two for post-traumatic headache. The two patients with hemicrania continua were responsive to indomethacin but had to discontinue its use secondary to medication side-effects (bleeding, nausea/vomiting).
Thirteen of these patients had ONB prior to stimulator implantation. Ten of 13 who had ONB had at least a 50% reduction in head pain lasting at least 24 h, and three of 13 were ONB non-responders.
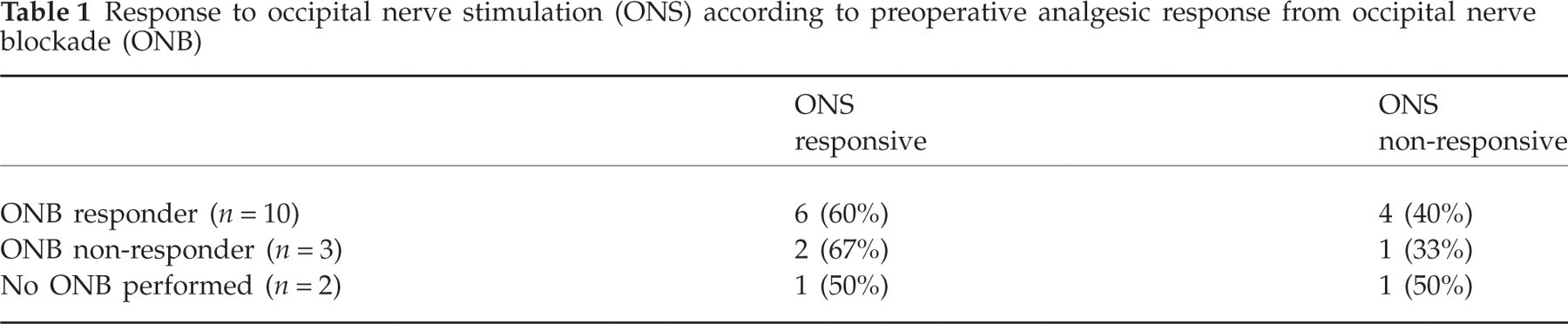
Overall, nine of 15 (60%) patients were ONS responders. Six of 10 (60%) ONB responders were also ONS responders. Of the three ONB non-responders, two (67%) were ONS responders. Of the two patients who did not have ONB prior to ONS, one was an ONS responder and one was an ONS non-responder (Table 1). ONB was not predictive of ONS response regardless of the number ONBs performed and whether ONBs were unilateral or bilateral (Table 2).
Response to occipital nerve stimulation (ONS) according to preoperative analgesic response from occipital nerve blockade (ONB)
Response to occipital nerve stimulation (ONS) according to response from occipital nerve blockade (ONB) (number and location), International Headache Society headache type, gender, age, years with headache type, laterality of ONS, and length of follow-up

ND, Not done; R, response; NR, non-response; Uni, unilateral; Bil, bilateral.
Response to first three blocks (unilateral) with subsequent non-response to two bilateral blocks.
Discussion
Sixty percent (9/15) of patients in this study were responders to ONS. Of the responders who underwent an ONB, 2/8 did not report analgesia, whereas 4/5 ONS non-responders reported analgesia from an ONB. Therefore, these data support previous reports of the efficacy of ONS for intractable headache disorders, but indicate that an analgesic response to an ONB will not reliably predict the outcome of ONS. While the numbers are small to draw definite conclusions on the response of individual headache subtypes to ONS, patients with hemicrania continua may be particularly responsive to this treatment modality.
Antinociceptive therapies targeted at the occipital nerves may be effective for the treatment of head pain located in the direct territory of the occipital nerves as well as in trigeminal innervated locations. The trigeminal nucleus caudalis receives input from C2 fibres as well as from the first division of the fifth cranial nerve. Studies have shown that stimulation of the greater occipital nerve causes increases in metabolic activity in the trigeminal nucleus caudalis and cervical dorsal horn at C1 and C2 (4). Stimulation of both the dura and the greater occipital nerve results in activation of neurons in the dorsal horn at C2, neurons which have receptive fields corresponding to the first division of the trigeminal nerve as well as skin and muscle from C2 (5). This anatomical and functional continuity explains how nociceptive input from the upper cervical segments can result in head and facial pain and how painful stimuli targeted at the head and face can result in neck pain. ONS and ONB, via different mechanisms, may thus modulate pain located in the posterior neck, head and face.
Although the mechanism of action of ONB is not completely elucidated, antinociceptive effect may be secondary to direct anaesthetic effects, mechanical effects of the injection itself, or to blockade of neurogenic inflammation. Like ONS, it may alter nociceptive trafficking into the trigemino-cervical complex. ONB has been shown to reduce head pain and brush allodynia in migraineurs (6). It has been hypothesized that ONB reduces trigeminal hyperexcitability by blocking the conduction of noxious stimuli and by blocking the antidromic flow of nociceptive vasoactive neuropeptides such as substance P and calcitonin gene-related peptide (7). Reduction of central sensitization may account for the prolonged effects of ONB in some patients.
Repetitive electrical stimulation of the occipital nerves has an analgesic effect which is probably a result of both peripheral and central mechanisms. The gate control theory of Melzack and Wall suggests that the relative activity of large sensory afferents compared with small sensory afferents mediates pain perception. Stimulation of large sensory afferent nerves suppresses small-fibre nociceptive input at the level of the spinal cord (8). Thus, repetitive electrical stimulation of the occipital nerves (large sensory afferents) may result in analgesia by presynaptic inhibition of small-diameter nociceptive fibres. Large sensory afferent stimulation also suppresses A-δ fibres, the activity of which correlates with pain perception (9–12). Suppression of A-δ fibres is accomplished through peripheral conduction blockade of these fibres and fibre ‘fatigue’ distal to the spinal cord (12). Direct evidence for central modulation of pain from ONS has been documented in a positron emission tomographic study. ONS-induced paraesthesias were found to correlate with changes in cerebral blood flow in the anterior cingulate cortex and left pulvinar (13).
Small studies of ONS have shown the efficacy of the treatment of occipital neuralgia and chronic migraine (3, 13–17). Prospective, randomized, sham-controlled studies of ONS for the treatment of medically recalcitrant headaches are currently enrolling.
Finding possible predictors of response to ONS is important in order to maximize its therapeutic potential in patients more likely to respond and to minimize patient exposure to an invasive procedure in those unlikely to respond. Current randomized controlled trials will, it is hoped, confirm the efficacy results demonstrated in open-label studies and identify reliable predictors of ONS outcome in migraineurs.
Conclusion
The data from this study, albeit in a small number of patients, confirm previous reports of the efficacy of ONS in patients with refractory headache disorders and suggest that neither a response nor non-response to ONB predicts response to ONS. Therefore, ONB may not be useful as a screening tool in patient selection for ONS.