
Abstract
Familial hemiplegic migraine (FHM) is a rare inherited autosomal dominant disorder. Migraine aura may last up to several weeks and then resolve without sequel. We report a 21-year-old male with FHM since the age of 3 years. Diffusion-weighted magnetic resonance imaging (DWI), perfusion-MR imaging (P-MRI) and [99mTc] hexamethyl-propyleneamine-oxime-single photon emission tomography (HMPAO-SPECT) were performed on day 2, when he was somnolent with right-sided hemiplegia, on day 9 when a mild hemiparesis was still present and on day 24 after recovery. The right central region showed normal findings in DWI, whereas P-MRI and SPECT revealed hyperperfusion on day 2, less marked on day 9, and normal findings on day 24. In conclusion, this case report indicates for the first time, by means of SPECT, P-MRI and DWI studies, that even extremely long-lasting migraine aura is not associated with cerebral ischaemia. Therefore, it supports the revised International Headache Society criteria where the term ‘persistent’ aura is proposed.
Introduction
Familial hemiplegic migraine (FHM) is a rare autosomal dominant allelic disorder (1, 2). It can be divided into a pure FHM, which is more common, and a FHM with permanent cerebellar signs. Moreover, there are reports of sporadic occurrence without affected family members in the literature (3–5).
According to the criteria of the International Headache Society (IHS), FHM is defined by migraine attacks with aura including a gradual progression of any degree of hemiparesis or other neurological deficits, which can outlast the headache, and where at least one first-degree relative has similar attacks (6). The aura symptoms may last > 1 h, but persistence of aura for more than 7 days, together with an corresponding MRI lesion in the brain, is attributed to migrainous stroke. Attacks usually start in childhood or adolescence. However, we know from various reports that attacks can last up to several weeks without any permanent neurological deficit (3, 7–9).
The diagnostic approach in patients with FHM is primarily focused on clinical symptoms and family history, although molecular biology is becoming more and more involved. In particular, mutation of the CACNA1A gene on chromosome 19p13, which encodes a neuronal calcium channel, is present in about 50% of patients with FHM (10, 11). Also imaging, such as single photon emission tomography (SPECT), positron emission tomography (PET) and different MRI techniques have become of interest in the pathogenesis of FHM.
The objective of this case report is to demonstrate the course of neurological deficits in a patient with FHM that lasted for more than 10 days without any permanent neurological deficit. Moreover, it is documented by follow-up findings of perfusion MRI (p-MRI) and diffusion-weighted MRI (DWI), as well as SPECT studies, without any signs of cerebral ischaemia.
Methods
P-MRI was performed as dynamic susceptibility enhanced MRI on a 1.5-T scanner as a whole brain study. A T2∗W-sequence with 20 slices and an acquisition matrix of 112 × 128 voxel slices were used and all images were reconstructed within a matrix of 256 × 256 voxels. Field of view was 240 mm and the slice thickness was 6 mm with a 0.6-mm gap. The temporal resolution was approximately 700 ms and scanning was performed in the axial plane. During the examinations a contrast medium bolus (Gd-DTPA, dose 0.15 mmol/kg) with an injection delay of 15 s was administered through a 20 G venouse canule in the cubita with 8 ml/s flow rate using an MR-motorinjector (Spectris; Medrad-Europe, AE Beek, the Netherlands). DWI was performed using a SE-EPI-sequence in three orthogonal planes with two b values: (i)
In each 99mTc-hexamethyl-propyleneamine-oxime (HMPAO)-SPECT investigation the patient underwent the same protocol. After resting for 20 min with eyes closed, 99mTc (Ceretec®; Amersham, Little Chalfont, UK) was administered intravenously in a quiet room. One hour later, SPECT studies were performed on a conventional three-head gamma camera (Multispect 3; Siemens, Knoxville, TE, USA) with a low-energy ultrahigh resolution collimator. The matrix size was 128 × 128, and data were collected in 60 directions at 2° steps over 120° (25 s per step). Data were reconstructed with a ramp filter and a Butterworth filter with the cut-off frequency of 0.9 and 9, respectively. Attenuation correction was performed by the Chang method with an attenuation coefficient of 0.12/cm. After reconstruction on the acquisition workstation, data were transferred to a Hermes workstation (Nuclear Diagnostics, Stockholm, Sweden). Quantification of perfusion defects was performed with both a voxel based analysis and a volume of interest (VOI)-based analysis using 46 predefined regions.
Case report
A 2-year-old male was referred to hospital because of subacute developing deterioration of vigilance, left-sided hemiparesis, and hemineglect to the left side. The patient was known to suffer from FHM. Since the age of 3 years, when FHM was diagnosed, four severe attacks with impairment of vigilance, hemiparesis and/or sensory deficits, and aphasia had occurred. Except the father, who also suffered from migraine with intermittent hemiparesis, the patient as well as the family members had no other relevant medical history.
Normally, the patient's migraine attacks lasted only several hours with various neurological deficits. Most frequently sensory symptoms on either right or left side occurred and progressed over a period of about 1–3 h, followed by a few hours of headache. This kind of headache in some cases could also be prevented by non-steroidal anti-inflammatory drugs, or if possible with one or two hours of sleep.
The last severe migraine attack occurred 4 years ago with right-sided hemiplegia and aphasia. At this time the patient's condition deteriorated subsequently over the next 24 h, so that he had to be intubated and admitted to an intensive-care unit. The attack lasted almost 3 weeks until complete remission. MRI showed a mild swelling of the left hemisphere but no signs of ischaemic stroke during the acute attack. Digital subtraction angiography (DSA), as well as CSF analysis was normal. Since then, the above described ‘normal’ migraine attacks occurred approximately once a month. The overall time span of these ‘normal’ attacks, starting with aura symptoms until the end of headache or end of the short sleep period, lasted from 2 to about 6 h.
Several hours before the recent severe attack started, the patient complained about subsequent increasing mild left-sided sensory disturbances as well as headache. On admission the patient was somnolent. Neurological examination demonstrated severe left-sided hemiparesis as well as left-sided sensory deficits such as hypaesthesia and hypalgesia, and a hemineglect to the left side. Symptoms deteriorated further over the next 24 h and the patient became hemiplegic.
Routine laboratory investigations from blood and urine samples were within normal limits. Electroencephalography (EEG) on day 2 demonstrated a diffuse slowing with high-amplitude theta/delta waves slightly pronounced over the right hemisphere. EEG on day 4 showed only mild slowing over both frontotemporal and temporal regions. Motor evoked potential (MEP) stimulated from Erb's point to the left abductor pollicis brevis muscle on day 2 was within normal limits on both sides (latency: right 12.0 ms/left 12.2 ms), whereas cortical stimulation revealed no amplitude after maximal stimulation on the left side, which is also in accordance with previous findings of van den Kamp (12), who demonstrated low amplitudes of MEP in FHM patients on the ictally paretic side. MEP to the right side was detectable (latency 23.1 ms). Somatosensory evoked potentials (SSEP) from the medianus nerve on day 2 showed normal latencies on both sides (right N1 = 18 ms, P1 = 22 ms, N2 = 37 ms; left N1 = 17 ms, P1 = 22 ms N2 = 34 ms), while the amplitude (N1-P1) on the left side (0.3 µV) was markedly decreased compared with the right side (4.4 µV). On day 28 MEP as well as SSEP returned to normal values.
MRI (T1/T2) and DWI on days 2, 9 and 24 were normal (Fig. 1). P-MRI demonstrated hyperperfusion on day 2, less marked on day 9, and normal findings on day 24 (Fig. 2). Also quantitative data of all p-MRI studies, by means of the left/right hemispheric asymmetry indices (AI), are shown in Table 1, indicating a continuous decrease of the AIs of cerebral blood volume (CBV) and estimated flow index (EFI) from day 2 to day 24 and a corresponding increase of stdTTP (time to peak).

Diffusion-weighted magnetic resonance imaging: normal findings.

Perfusion-magnetic resonance imaging showing hyperperfusion over the right hemisphere on day 2 (most pronounced over the precentral area: see white arrow), less pronounced on day 9 and normal findings on day 24. (See also quantitative data in Table 1.)
Asymmetry indices (AI) of perfusion MRI studies on days 2, 9, and 24

Continuous decrease of AIs of cerebral blood volume (CBV) and estimated flow index (EFI) from day 2 to day 24 and corresponding increase of time to peak (stdTTP). (See also Fig. 2.)
There were no signs of cerebellar atrophy as described in some patients with FHM (13–15).
On days 2, 9, and 24 also a technetium 99mTc-HMPAO-SPECT was performed (Fig. 3). Results on day 2 showed increased tracer uptake over the right frontobasal cortex, as well as over the right mesiooccipital region, and also over the right temporoparietal region, though not as pronounced in comparison with the left side. Moreover, increased tracer uptake could also be observed over the right cerebellum. Basal ganglia were normal on both sides. On day 9, a mild right/left asymmetry (increased tracer uptake over the right hemisphere), left parietooccipital sparing of tracer, as well as increased tracer uptake in the left cerebellum could still be demonstrated. On day 24 cortical tracer uptake was symmetrical over all other regions. Quantitative data, indicating the AIs over various regions from day 2 to day 24, are shown on Table 2.
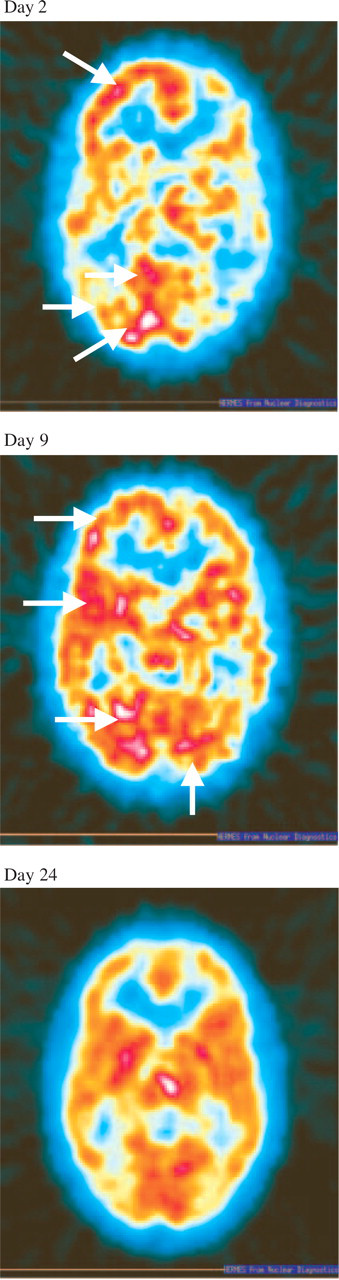
99mTc-HMPAO-SPECT. Increased tracer uptake on day 2 over the right frontobasal cortex, the right cerebellum, the right mesiooccipital region, and, not as pronounced, also over the right temporoparietal region compared with the left side (white arrows). On day 9, still increased tracer uptake over the right hemisphere, as well as increased tracer uptake in the left cerebellum (white arrows). On day 24 cortical tracer uptake was symmetrical over all other regions. (See also quantitative date in Table 2.)
Asymmetry indices (AI) of 99mTc-HMPAO SPECT studies on days 2, 9, and 24
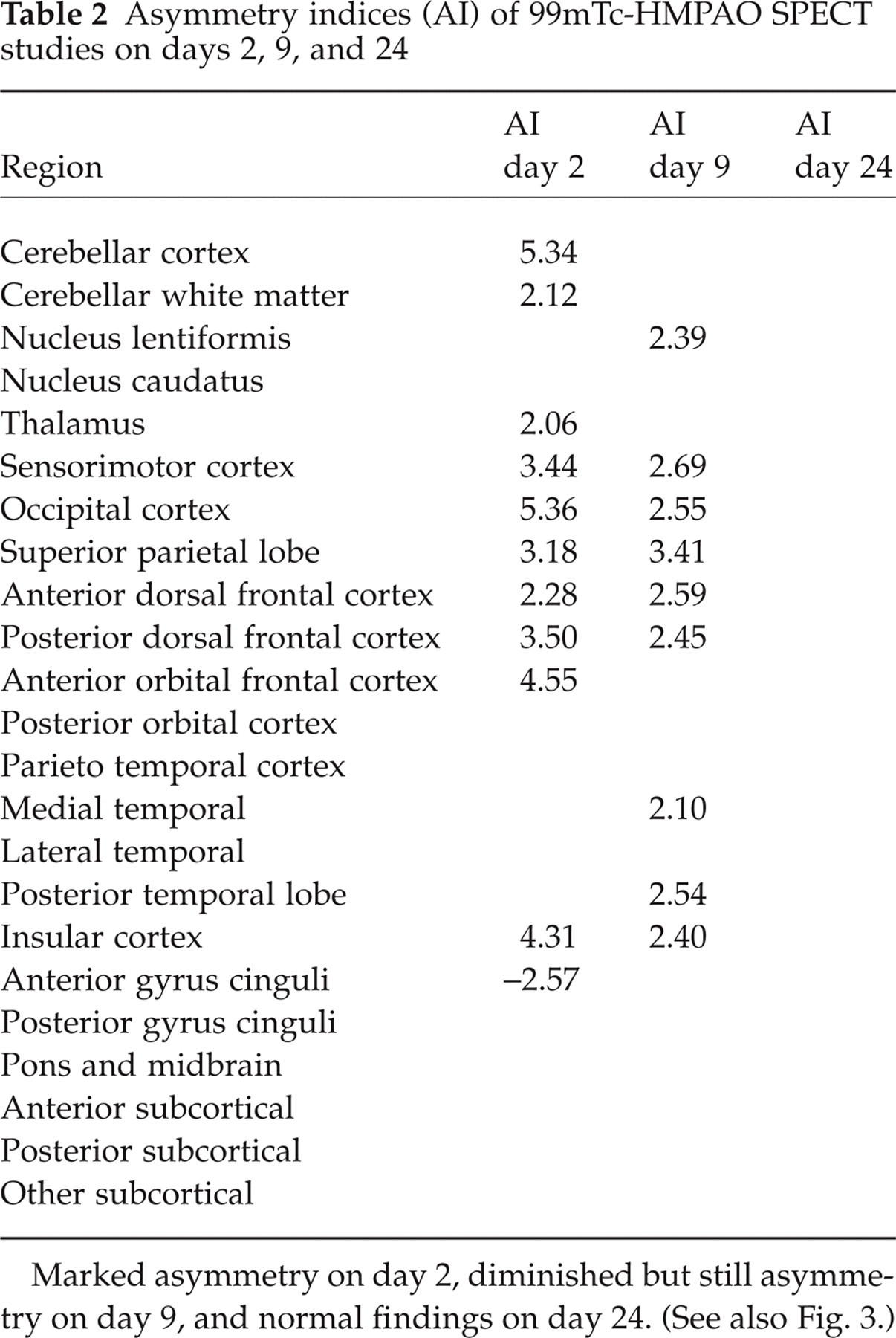
Marked asymmetry on day 2, diminished but still asymmetry on day 9, and normal findings on day 24. (See also Fig. 3.)
Ten days after the onset of the migraine attack the patient was discharged. Neurological examination revealed only a discrete paresis of the left arm and a mild left-sided ataxia in the finger nose test. The hemineglect completely remitted. Clinical follow-up investigations on days 17 and 24 after the attack showed no pathological findings.
Discussion
In migraine with aura, the symptoms of dysfunction of the cerebral cortex or brain stem usually last < 60 min, occasionally the duration exceeds 1 h, and rarely the neurological deficit persists for > 1 week. According to the current criteria of the IHS, the first is typical aura, the second prolonged aura and the third is defined as migrainous stroke suggesting an ischaemic event. As we know from our patient and various other case reports, migraine aura can last up to several weeks and then resolve without sequele (3, 7–9). Accordingly, the term ‘persistent aura’ as suggested in the proposal for the forthcoming revision of the IHS criteria (http://www.i-h-s.org) is useful and necessary for differentiating ischaemic from non-ischaemic events in migraine patients with long-lasting neurological deficits.
We report a young male suffering from FHM who experienced a severe and extremely long-lasting migraine attack. The present case report is the first showing follow-up findings of DWI, P-MRI and HMPAO-SPECT in a patient with persistent aura according to the new revised IHS criteria, in which neurological deficits, such as somnolence, hemiparesis and hemineglect, may outlast the 7-day limitation. It indicates, by means of different imaging techniques, that long-lasting migraine aura (>7 days) is not necessarily associated with cerebral ischaemia, as proclaimed by the 1988 IHS criteria (6).
Imaging techniques have proved helpful in investigating the pathogenesis of FHM. Masuzaki et al. reported dilatation of arteries in MR angiography as well as hyperperfusion in the affected hemisphere by means of P-MRI in a patient with FHM, which spontaneously resolved after the attack (16). Similarly, hyperperfusion was found in P-MRI in a patient with prolonged aura (17) and in another patient with persistent aura by means of SPECT (18). Guschalk et al. (9) demonstrated glucose-hypometabolism by means of PET in a patient with FHM in the affected hemisphere during the attack, suggesting a primary neuronal dysfunction causing prolonged neurological deficits. In migraine patients with aura, Sanches del Rio et al. showed transient decreased blood flow contralateral to the affected hemifield during aura using P-MRI (17). Hypoperfusion during typical aura was also observed by Andersen et al. and Cutrer et al. (19, 20), whereas in migraine patients without aura no haemodynamic changes were observed (6). It has also been reported in other series that during typical ‘prolonged’ or ‘persistent’ aura symptoms, initial hypoperfusion occurred followed by a period of hyperperfusion by means of transcranial Doppler, SPECT, MRI, DWI, p-MRI and functional MRI (fMRI) (16, 18, 19, 21–24). Cao et al. and Hadjikhani et al. additionally observed an initial brief wave of hyperperfusion which was followed by diminished blood oxygenation level-dependent signal changes in patients with migraine by means of fMRI (25, 26). In our patient, shortlasting initial hyperperfusion followed by hypoperfusion cannot be excluded. However, our findings clearly indicate that the ischaemic threshold had not been crossed even in this case of an extremely long-lasting migraine attack.
DWI studies recently found reversible decreased water diffusion contralateral to the clinically affected side in a patient with FHM which, however, could not be reproduced in our patient (27).
Concluding the imaging data from the literature in migraine patients, the aura seems to be associated with a brief wave of initial hyperperfusion followed by hypoperfusion of the affected hemisphere causing neurological symptoms, and later by a temporally variable state of hyperperfusion. In our patient imaging techniques such as p-MRI, as well as SPECT, were in accordance with the literature with respect to the enduring hyperperfusion. However, it is unclear why neurological deficits are still present under conditions of subsequent hyperperfusion.
With respect to the new imaging methods as well the neurological features, FHM may mimic a transient ischaemic attack (TIA). However, it can be clinically distinguished from TIA by the gradual development and progression of aura symptoms or even by the change of one aura symptom to another, whereas an instant onset of symptoms is characteristic of TIA. In our patient, neurological deficits proceeded from mild sensory disturbances to hemiplegia within 24 h, and lasted for > 10 days. Moreover, he initially complaint about headache, and family history regarding hemiplegic migraine was positive. All these clinical factors make a transient ischaemic event unlikely. Therefore, we propose an initial expanded state of hypoperfusion in our patient, which led to an ongoing impairment of neuronal cells but staying beyond the ischaemic threshold.
Another syndrome with headache, neurological deficits and CSF lymphocytosis (HaNDL syndrome) may be considered for differential diagnosis. As we know from the first severe attack 4 years ago, CSF analysis in our patient was normal. Moreover, HMPAO-SPECT in patients with HaNDL syndrome showed decreased tracer uptake topographically consistent with the neurological deficits, while in patients with prolonged aura tracer uptake is increased (28–30), as was the case in our patient. Moreover, the duration of neurological deficits from a series of 50 HaNDL patients was reported to be a mean of only 5 h (29). Therefore, the presence of HaNDL syndrome in our patient seems unlikely.
Additional aspects of a more precise clinical diagnosis of FHM are postulated by Thomsen et al. based on a population-based study in Denmark (31). Due to several cases with reduced penetrance, the authors recommend also including second-degree relatives without first-degree relatives in the new diagnostic criteria of FHM. Moreover, the requirement of two gradual developing aura symptoms and expanded duration of each aura symptom up to ≥ 24 h should be implemented. The term hemiparesis might also be changed to motor weakness, because in their study some patients had only one extremity affected. Despite the long-lasting aura, our patient seems to be a classical FHM patient, with first-degree FHM relative and hemiplegia. However, comparing our report with these adapted criteria for FHM, we would agree to expand the duration of aura symptoms, which is already accounted for in the revised IHS criteria.
Migraine attacks in patients with FHM also have a high variability in frequency as well as in neurological symptoms within and between different families (32). In a larger population-based study, 63% of patients reported their lifetime number of migraine attacks as < 100, but 37% suffer < 100 attacks (31). Our patient reported four severe migraine attacks so far, with variable degree and side of the hemiparesis. During the last years, slight attacks with mild sensory deficits and headache occurred about once every 2 months.
Our report is the first presenting follow-up findings in a patient with FHM and persistent migraine aura indicating that a long duration of the aura symptoms is not associated with cerebral ischaemia. Therefore, this case report supports the proposed revision of the IHS criteria in order to differentiate ischaemic events (migrainous stroke) from non-ischaemic (persistent aura) in migraine patients with long-lasting neurological deficits.