
Abstract
Two patients with cerebrospinal fluid (CSF) leak, one at the level of fourth thoracic spine and another with undetermined level of leak, presented with paradoxical postural headaches in that the headaches were present when in a horizontal position and resolved if the patients were upright. One patient improved spontaneously and the other responded to a targeted epidural blood patch. Paradoxical postural headache is yet another headache type that can be associated with CSF leak and CSF volume depletion. Its mechanism is uncertain, but it could be related to congestion and dilatation of cerebral venous sinuses and large veins.
Keywords
Introduction
It is now recognized that the majority if not all cases of spontaneous intracranial hypotension (SIH) result from spontaneous cerebrospinal fluid (CSF) leaks. In the past decade, a much broader clinical and imaging spectrum of this disorder has been recognized. Headache, which is by far the most common clinical manifestation, is typically orthostatic (present when the patient is upright and relieved by recumbency). However, not all patients have orthostatic headaches (1). Several different types of headache have been reported in spontaneous CSF leaks (2). In this study, we report two patients who had paradoxical orthostatic headaches (headaches in recumbency, relieved when upright).
Case reports
Patient 1
A 53-year-old, right-handed woman was in good health except for a longstanding past history of migraine headaches described as unilateral, throbbing headaches preceded by scintillating scatomas and associated with photophobia, nausea, and sometimes emesis. These had occurred for many years with variable frequency, most recently a few times per month. In December 2000 patient developed tinnitus and sonophobia in the left ear. Treatment for ‘otitis’ was not helpful. About a month later, similar symptoms developed in the right ear, and there was also reduced hearing, nausea, and vertigo. The cochleovestibular symptoms on the left improved, but a fronto-occipital headache developed associated with off-and-on vague blurring of vision without diplopia or visual field defects. She also began to note that the headaches were noticeable when she lay flat and would markedly lessen and eventually resolve after having been upright for several minutes. Therefore, she had to sleep in a sitting position in a recliner. A head magnetic resonance imaging (MRI) in early March 2001 revealed diffuse pachymeningeal enhancement (Fig. 1a) and subdural fluid collections (Fig. 1b,c), pituitary enlargement, decrease in size of perichiasmatic cisterns and decrease in size of the lateral ventricles (Fig. 2a). A CSF examination revealed three leucocytes per cubic millimetre, protein concentration of 52 ml/dl, and glucose concentration of 50 mg/dl. CSF opening pressure was not measured.

(Patient 1.) Head magnetic resonance imaging (MRI), gadolinium enhanced T1-weighted axial images (a, d), unenhanced T1-weighted parasagittal images (b, e), and T2-weighted axial images (c, f). During the symptomatic phase (a–c) there is diffuse pachymeningeal enhancement (a) and subdural fluid collections (b, c). After clinical recovery, all of the MRI abnormalities have resolved (d–f).
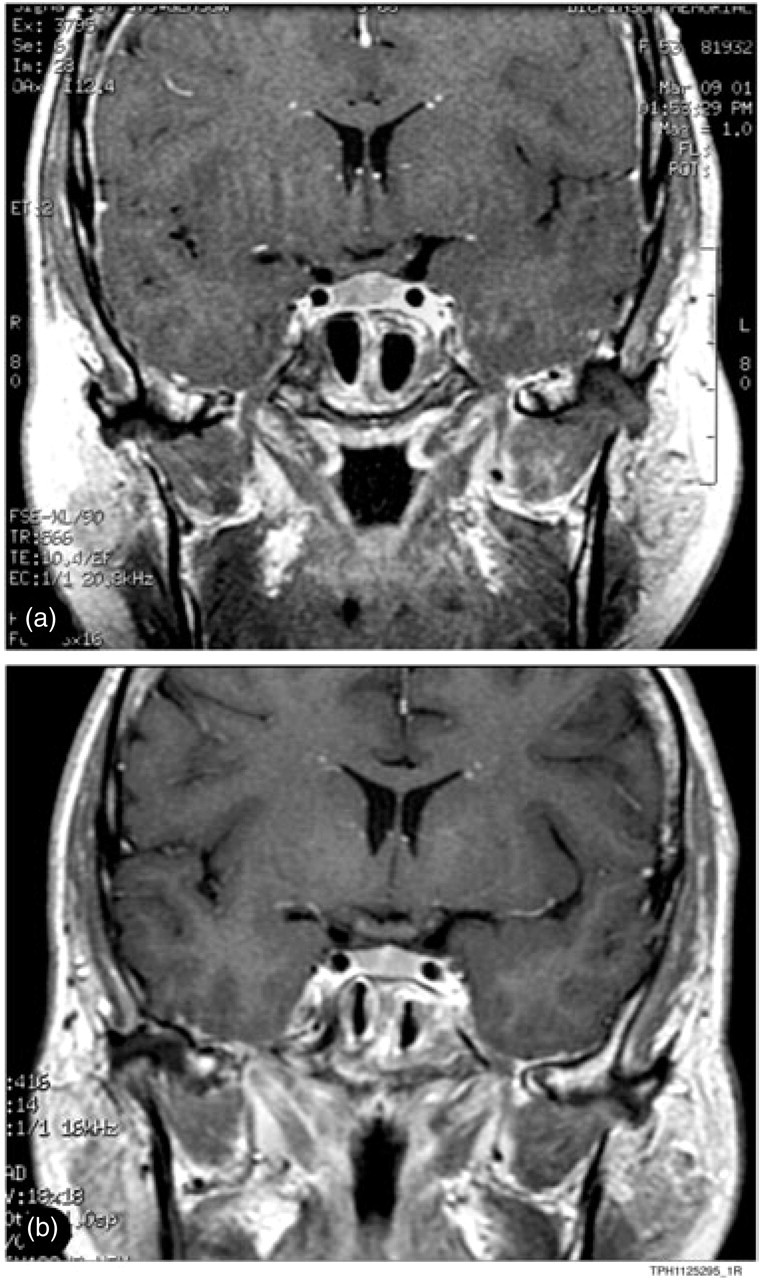
(Patient 1.) T1-weighted gadolinum-enhanced head magnetic resonance images, coronal cuts at the level of pituitary, during the symptomatic phase (a) and after recovery (b). Note relative enlargement of the pituitary, subtle decrease in size of the ventricles and decrease in size of the perichiasmatic cistern. All of these have resolved after clinical recovery (b).
The patient was seen at the Mayo Clinic in May 2001 with concerns about an unknown meningeal disease. By this time, however, her symptoms had essentially resolved. Repeat MRI showed resolution of the previously noted abnormalities (Fig. 1d–f and Fig. 2b). CSF opening pressure was 185 mm H2O, and CSF protein, glucose, and cell count were all normal. She has remained asymptomatic.
Patient 2
A 60-year-old right-handed woman in February 2002 following a ‘cold’ and coughing began to experience severe headaches with exertional features and much discomfort if she coughed, sneezed, bent over, or strained. Treatment with indomethacin was not helpful. Additionally, she became aware of headaches in recumbency that would dissipate within several minutes after having been upright. A head MRI showed diffuse pachymeningeal enhancement (Fig. 2a) and the question of ‘meningitis’ was raised. CSF examination revealed an opening pressure of 110 mm H2O, and CSF analysis showed no abnormalities. She subsequently underwent a meningeal biopsy in June 2002. It showed no evidence of inflammation, infection, or infiltration, but findings similar to a thin organizing subdural hygroma as has been described in intracranial hypotension and CSF hypovolaemia (3).
She continued to be disturbed by the headaches, that would start when she lay down although these were absent when she was upright. She would use extra pillows to keep the head up when she went to bed at night, and even then she had to get up once or twice and assume an upright position for 45 min to 1 h before getting relief. Additionally, Valsalva-type manoeuvres markedly aggravated the headaches or, if the headaches were absent (such as during the daytime when she was up and about), Valsalva manoeuvres would trigger the headache for a few to several minutes. These exertional and paradoxical orthostatic headaches persisted. The patient was seen at the Mayo Clinic in Rochester, Minnesota, in March 2003. Neurological examination showed no neurological deficits. Head MRI was tried but had to be aborted before completion because of severe headache in recumbency. MRI was subsequently tried under anaesthesia and revealed diffuse pachymeningeal enhancement, a prominent pituitary gland, flattened optic chiasm, mild compression and flattening of the anterior pons against the clivus, and low-lying cerebellar tonsils (Fig. 3a,b). The findings correlated strongly with CSF leak. MRI of the entire spine showed only mild to moderate spondylotic changes. There was some clumping of the roots of cauda equina and minimal enhancement. CSF opening pressure was 160 mmH2O and CSF analysis showed no abnormalities. Myelography/computed tomography (CT) myelography showed multiple, scattered, symmetric, dilatated nerve root sleeve pouches and small meningeal diverticula throughout the thoracic spine, particularly pronounced in the lower thoracic region. No evidence of contrast extravasation was seen.

(Patient 2.) Coronal section, T1-weighted gadolinium-enhanced head magnetic resonance imaging (MRI) (a) shows diffuse pachymeningeal enhancement, prominent pituitary gland, flattened optic chiasm, and partially obliterated perichiasmatic cistern. Unenhanced T1-weighted sagittal MRI (b) show low-lying cerebellar tonsils. 111Indium cisternogram (c) shows paucity of activity over the cerebral convexities at 24 h. MRI myelogram after introduction of intrathecal gadolinium (d) shows leak at upper thoracic spine level (E, arrow).
Radioisotope cisternography showed no parathecal activity, but there was paucity of activity over the cerebral convexities at 24 h (Fig. 3c). MR myelography following intrathecal injection of gadolinium (Fig. 3d) revealed the site of the leak at T4 (Fig. 3e). Targetted epidural blood patch at T4–5 interspace resulted in resolution of the headaches.
Discussion
Headache is the most common clinical presentation of spontaneous CSF leaks (4–6), although the disorder may have many other additional (2) manifestations.
The headache is typically orthostatic and resembles post-spinal tap headaches (present when upright, relieved by recumbency). However, there is considerable variability in the features of the headache in a substantial minority of patients: (i) with chronicity, sometimes the headaches may lose their orthostatic features and transform into lingering, chronic daily headaches (5); (ii) neck pain or interscapular pain may precede the headaches by days, weeks, or even a few months; (iii) the features of the headaches may occasionally be indistinguishable from benign exertional headaches (7); (iv) a lingering, non-orthostatic headache may precede orthostatic headaches by days, weeks, or months; (v) in some of the patients the headache may mimic chronic daily headaches in its entire course; (vi) occasionally the orthostatic headaches may have thunderclap onset, initially resembling a cerebrovascular event (8); (vii) some patients may have no headaches in the initial half of the day and by late morning or early afternoon may begin to develop increasing headaches that are more pronounced when upright and decrease in recumbency. In intermittent CSF leaks, the headaches, with whatever features they might have, may appear and disappear for variable periods of time. Some patients with documented CSF leaks and low CSF pressure and typical imaging features of the CSF leaks may have no headaches at all (9).
In the horizontal position the CSF pressure in the lumbar, cisternal, and probably vertex is equal (approximately 60–180 mm water). When an upright position is assumed, then these pressures diverge, the vertex pressure becomes negative while the lumbar CSF pressure would increase to 375–550 mm water (10).
We have previously reported a patient with CSF leak from a craniotomy site who had paradoxical postural headaches (headache present when lying down with relief of the headache in upright position) (11). In that patient, it was thought that the paradoxical, posture-dependent headache was probably related to leakage of CSF from the craniotomy site in recumbency, a position in which the vertex pressure is positive. The appearance of the headache with recumbency was not immediate but was delayed for several minutes, allowing time for enough CSF leak to occur, causing enough CSF hypovolaemia to produce headache. Conversely, in an upright position drop in intracranial and vertex pressure would lead to cessation of the CSF leak and after a period of delay, when enough CSF is replaced, the headache also ceases. This proposed mechanism, which appears acceptable for paradoxical postural headaches due to CSF leak from a craniotomy site or CSF leak at calvarial level, would be quite difficult to apply to spontaneous CSF leaks that occur at the spinal level.
The first patient had been evaluated elsewhere before referral to us. Although the CSF opening pressure had not been measured, the constellation of imaging abnormalities was highly suggestive of CSF volume depletion and CSF leak. Furthermore, we suspect that the leak was at the spinal level, since spontaneous CSF leaks at the skull level are uncommon. This patient had no history of trauma. There was no rhinorrhoea or otorrhoea or any hint of skull defect on imaging studies. In our second patient, MRI abnormalities and cisternographic finding of paucity of activity over cerebral convesities at 24 h (2) strongly suggested CSF leak. Although the site of the leak was not detected by CT myelography, MR myelography (spine MRIs after intrathecal introduction of gadolinium) revealed the site of the leak at the upper thoracic spine level. This technique may prove promsing (12, 13). The orthostatic headaches in CSF leaks are attributed to sinking of the brain and pressure upon, and traction of, pain-sensitive intracranial structures (4–6). It is likely that engorgement of cerebral venous sinuses may also be a contributing factor, but presumably to a lesser extent. It is possible that in occasional patients the latter mechanism may become the dominant factor, perhaps as the result of an associated dysfunction of autoregulation leading to increased cerebrovascular volume in recumbency and therefore to ‘paradoxical’ postural headaches, where in a horizontal position cerebral venous sinuses and larger veins are more engorged than in an upright position. This explanation, however, remains speculative. Paradoxical postural headaches, although uncommon, are yet another type of headache that can be seen in CSF leaks and CSF hypovolaemia.