
Abstract
This study validates the method of interviewing only the first-degree relatives indicated by the proband as possible cluster headache sufferers. We interviewed essentially all the first-degree relatives (93%) of 87 probands with cluster headache. We found only one new first-degree relative with cluster headache (1/ 40 = 2.5%). The selective interview may be used with confidence as a means of investigating the hereditary component of cluster headache.
Introduction
Until recently cluster headache (CH) was considered a sporadic disorder. In two separate studies a 45-fold increased risk of CH (1) and a 14-fold increased risk in first-degree relatives have been reported (2). In a more recent Italian study, the risk of CH was 39 times higher in first-degree relatives than in the general population (3). The variation is probably attributable to methodological differences. In one study (1), family history data were provided by headache patients and not confirmed by direct contact with relatives. In another study a postal questionnaire was sent to probands, and suspected cases were confirmed by interview (2). In the Italian study information on the relatives of 220 CH patients was obtained by direct interview with the probands in 124 cases, and by postal questionnaire in the remaining 96; subsequently all indicated relatives were interviewed by telephone.
In all three studies the point of departure was information obtained from the proband, but it does not seem intuitively likely that one person will be aware of the state of health of their entire family. The aim of the present study was to determine whether direct interview of all the first-degree relatives of a series of CH patients provided a more accurate estimate of the prevalence of CH in families than the method of simply interviewing the sample of relatives indicated by the proband as possibly suffering from the disease.
Methods
We telephone-interviewed all the first-degree relatives of 87 of the 220 CH patients we investigated in our previous study (3). We contacted all the first-degree relatives of the 44 patients in whom we previously found a positive family history of CH (76 males, 78 females, mean age 43 years, range 6–79 years). We also contacted all the first-degree relatives of 43 sporadic cases of CH (130 males, 109 females, mean age 46 years, range 5–91 years). The first group constituted the complete set of families with two or more members known to have CH (3). The 43 other families were selected in consecutive order of presentation of the probands at our headache centre. The telephone interviews were conducted with the aid of a previously validated questionnaire (2).
Results
As shown in Table 1, we identified a total of 393 first-degree relatives, 154 from the familial CH families and 239 from non-familial CH families. Thirty-nine first-degree relatives in the familial group were found to suffer from CH in a previous study (3) and were not considered in this study. Seventy-one relatives had died (22 in the familial group and 49 in the non-familial group). In addition, we did not contact the 23 first-degree relatives (10 in the familial group and 13 in the non-familial group) who were below the age 10 years. Subjects below 10 years were not included for an interview for two reasons: first, because CH is rare in this age group, and second because information is possibly less certain. Thus the participation rate was 393 − 71 − 23 = 299/(393 − 71) = 322, i.e. 93% among those it was possible to interview (the de facto rate was 299/393 = 76%). The direct interview of all first-degree relatives supplied only one new case with episodic CH.
Comparison of familial vs. non-familial cluster headache (CH) sufferers
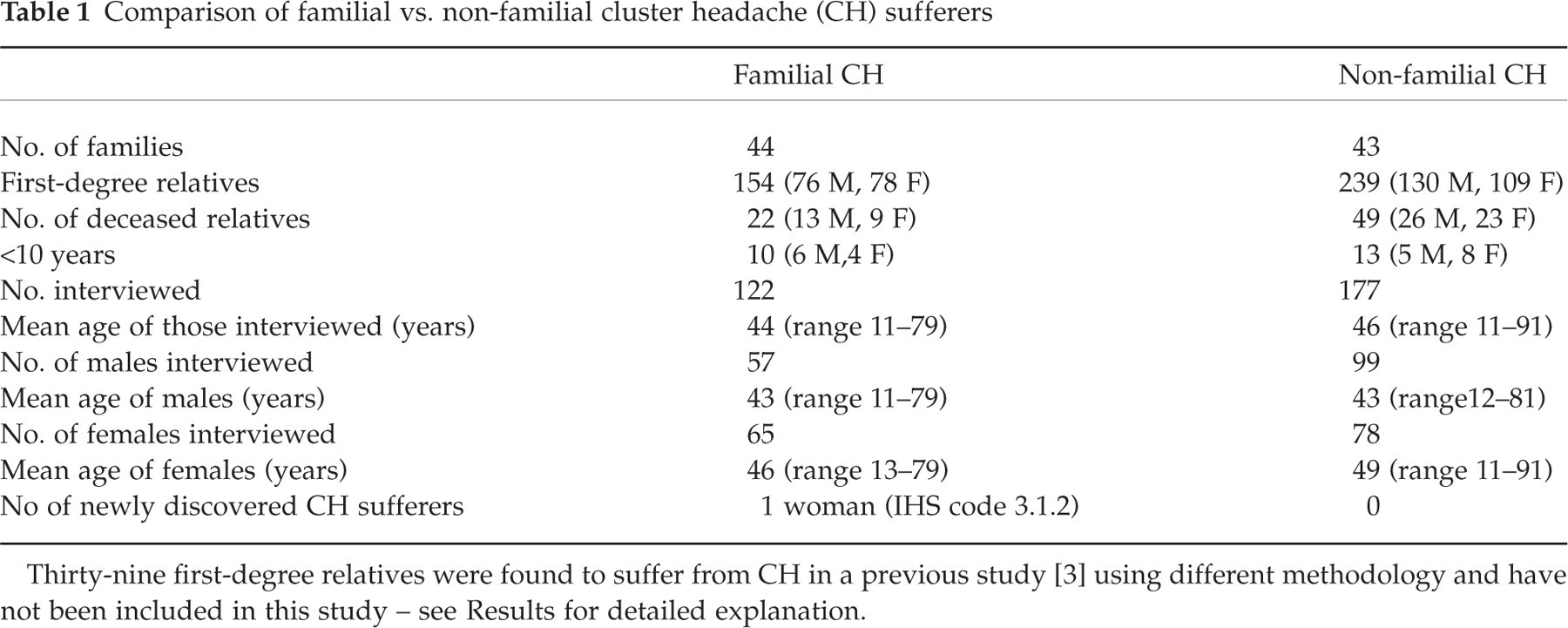
Thirty-nine first-degree relatives were found to suffer from CH in a previous study [3] using different methodology and have not been included in this study – see Results for detailed explanation.
Discussion
The methodology of the present study – interview of all the first-degree relatives – is too time-consuming and expensive to be proposed as a general one for investigating CH. However, this approach is not a valid investigation in migraine, as probands underestimate by 51% the number of affected first-degree relatives (4). This information was distorted even more looking at the specific subtypes of migraine, i.e. migraine without aura and migraine with aura. The high underestimation rate found in migraine studies is probably due to the non-uniform clinical picture of this form of headache; in contrast, the highly and easyily recognizable clinical picture of CH facilitates recognition of affected relatives.
It must be mentioned that in countries with a strong family tradition it may be easier to rely on questions regarding relatives than in countries with a high percentage of immigrants and possible barriers in familial face-to-face interaction. This factor has to be taken in account in future studies considering affected relatives.
The present data validate the methodology of our previous study (3), that of using only information supplied by the proband, and subsequent interview of those indicated, to identify relatives suffering from cluster headache.