
Abstract
As clinic-based studies show an association between headache and both high and low levels of haemoglobin, we analysed this relationship in a population-based cross-sectional study (the HUNT Study). A total of 2385 women aged 20-55 years responded to a headache questionnaire and gave blood samples for measuring haemoglobin and ferritin. In the multivariate analyses, adjusting for age and education, there was a linear trend of decreasing prevalence of headache (P = 0.02) and migraine (P = 0.01) with decreasing haemoglobin. In particular, migraine was less likely among women with low haemoglobin (values < 11.5 g/dl) (odds ratio 0.4, confidence interval 0.2, 0.9). There was no correlation between headache prevalence and ferritin. The present findings may be relevant for the headache reported in polycythaemia and chronic altitude sickness.
Introduction
The relationship between haematological parameters and headache is seldom commented on (1, 2), and it has been the subject of relatively few studies. As to the association between anaemia and headache, there are conflicting reports in epidemiological studies. In one study there was a positive association (3), but not in two others (4, 5). With regard to elevated haemoglobin levels, headache has been reported in conditions such as polycythaemia and chronic altitude sickness (6–10). All these clinic-based studies are prone to selection bias and these results have to be confirmed in unselected population-based studies.
As to the relationship between headache and iron, a population-based study has reported a high prevalence of headache in women with hereditary haemochromatosis (11). Elevated levels of iron in the periaqueductal grey matter in the brainstem have been found by magnetic resonance imaging in patients with migraine and chronic daily headache (12). No study has investigated the relation between headache (including migraine) and haemoglobin and iron stores, assessed by serum ferritin.
The main purpose of the present cross-sectional population-based study was to investigate the relationship between headache (including migraine) and haemoglobin and ferritin.
Materials and methods
Between 1995 and 1997, all inhabitants aged 20 years in Nord-Trøndelag County in Norway were invited to enter a health survey programme (the HUNT Study), encompassing about 40 subprojects. Of 92 566 invited individuals, a total of 64 560 (70%) answered a first questionnaire (Q1) and participated in a brief medical examination, at which they were given a second questionnaire (Q2) including 13 questions about headache to be filled in and returned from home. A total of 51 383 subjects (80% of the participants) answered Q2.
In order to evaluate the prevalence of iron deficiency anaemia, blood samples for serum ferritin and haemoglobin were drawn from a random sample of 2945 non-pregnant, non-blood donor females aged 20–55 years who participated in the brief medical examination. Participants who both answered Q2 and had blood samples were included in the present study.
Iron and haemoglobin status
The reference intervals for haemoglobin were 11.5–15.5 g/dl and for ferritin 14–110 µg/l. Individuals with values below or above the reference limits were grouped separately.
Headache diagnosis
The first of the 13 questions about headache in the Q2 was ‘Have you suffered from headache during the last 12 months?’. Individuals who answered ‘yes’ to the question were classified as ‘headache sufferers’. Based on data from the subsequent 12 headache questions, they were classified into two groups, either migraine or non-migrainous headache. Persons were diagnosed as migraine sufferers if they self-reported migraine or fulfilled the following three criteria:
Headache attacks lasting from 4 to 72 h (≤72 h for those who reported frequent visual disturbances before the attacks).
Headache had at least one of the following three characteristics: pulsating quality, unilateral location, or aggravation by physical activity.
During headache, at least one of the following was present: nausea, photophobia or phonophobia.
The diagnoses were mutually exclusive, so that headache not satisfying the criteria for migraine was classified as non-migraineous headache. Our criteria for migraine were a modified version of the migraine criteria of the International Headache Society (IHS) (13). The most notable modification was that severity of pain was not included among the pain characteristics. The questionnaire-based headache diagnoses were validated by interview diagnosis reported in a separate paper, including a discussion about the discrepancy between our migraine criteria and the IHS criteria (14). The positive and negative predictive values were, respectively, 84% and 78% for migraine, and 68% and 76% for non-migrainous headache. The 1-year prevalence of migraine and non-migrainous headache in the whole population (51 383) was 12% and 26%, respectively (15). Among those with non-migrainous headache, 80% had tension-type headache according to our validation study.
Statistical analysis
Differences between means were tested with unpaired t-tests. P-values < 0.05 were considered statistically significant. We estimated prevalence odds ratios (OR) with 95% confidence intervals (CI) for the association between headache (migraine and non-migrainous headache combined) and haemoglobin and ferritin. The general population was used as a reference, and the total number of participants was the same in all analyses performed. Potential confounding by age (5-year categories) and years of education (<10, 10–12, and >12) was evaluated using unconditional logistic regression. Haemoglobin was also treated as a single ordinal variable (categories, 1, <11.5; 2, 11.5–15.5; 3, >15.5) and was incorporated in a two-sided test for trend in order to evaluate the probability of a linear relationship between the haemoglobin categories and headache prevalence. In Fig. 1 haemoglobin was split into more subcategories than in Table 2. Proportions were compared with χ2 test (Table 1).

One-year prevalence of headache with 95% confidence interval (CI) related to haemoglobin values.
Demographics of the participants compared with the group who gave blood samples but did not respond to Q2, and the group who responded to Q2 but did not give blood samples
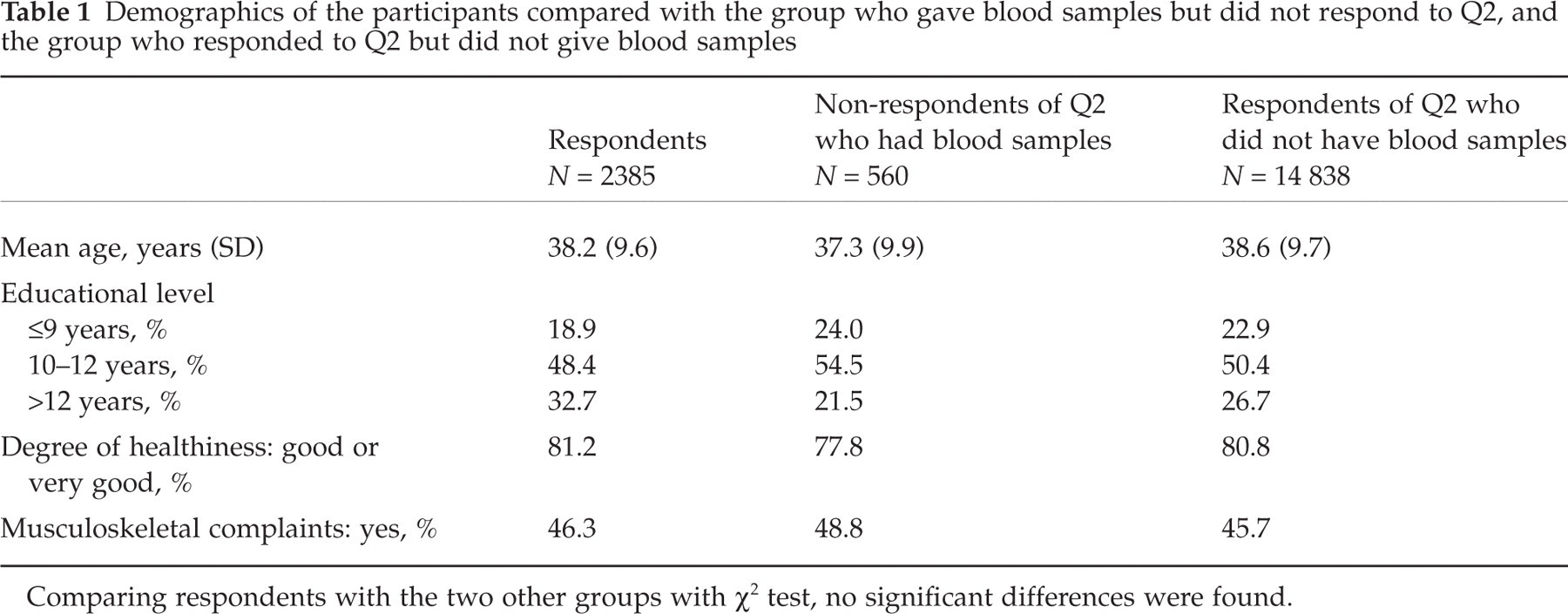
Comparing respondents with the two other groups with χ2 test, no significant differences were found.
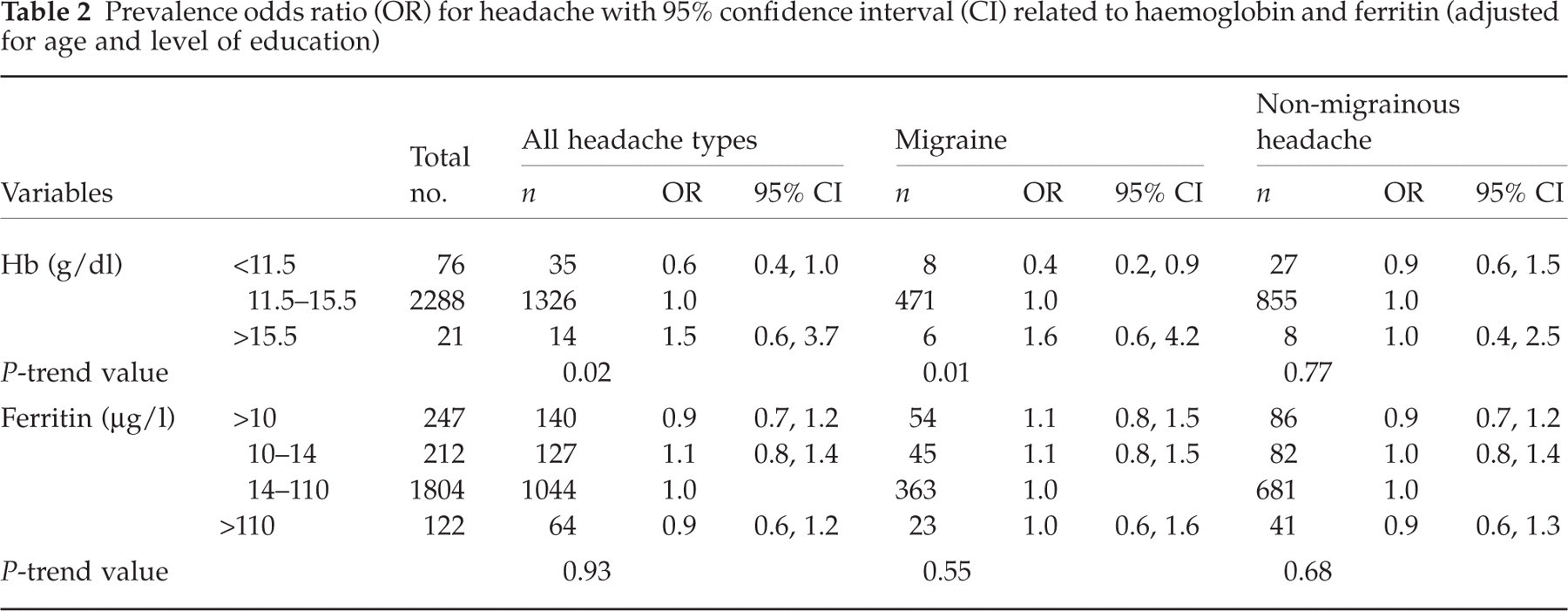
Prevalence odds ratio (OR) for headache with 95% confidence interval (CI) related to haemoglobin and ferritin (adjusted for age and level of education)
Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 8.0 (SPSS Inc., Chicago, IL, USA).
Ethical approval
The study was approved by the Regional Committee for Ethics in Medical Research, and by the Norwegian Data Inspectorate.
Results
Of the 2945 non-pregnant non-blood donor females who gave blood samples, 2385 (80%) answered Q2 and were included in the study. Mean age, educational level, degree of healthiness and musculoskeletal complaints did not differ significantly in these 2385 women compared with the 560 non-respondents to Q2 who gave blood samples and the 14 838 respondents to Q2 who did not give blood samples (Table 1).
As demonstrated in Fig. 1, there was a slight tendency to lower prevalence of headache among women with haemoglobin levels <11.5 g/dl. In the multivariate analyses, adjusting for age and education, there was a linear trend of decreasing prevalence of headache (P = 0.02) and migraine (P = 0.01) with decreasing haemoglobin levels. The headache prevalence was lower (OR = 0.6, CI 0.4, 1.0) when haemoglobin was low (<11.5 g/dl) than when haemoglobin was within the normal range (Table 2). In particular, migraine was less likely among subjects with low haemoglobin values (OR = 0.4, CI 0.2, −0.9). Admittedly, this group was small (only eight out of 76 women with haemoglobin <11.5 g/dl suffered from migraine), but when the cut-off point for defining anaemia was increased to 12.0 g/dl, the prevalence of migraine was still significantly lower [24 out of 175 subjects had migraine (OR = 0.6, CI 0.4, 0.9)].
There was no association between ferritin levels and headache prevalence (Table 2). A total of 247 women had ferritin <10.0 µg/l. Of these, only nine subjects had haemoglobin <10.0 g/dl. Headache prevalence did not differ between women with both low haemoglobin and ferritin (OR = 0.6, CI 0.2, 2.6) and those with normal values. There was no significant difference in the proportion of headache sufferers taking oral iron supplements (7.1%) compared with subjects without headache (5.5%) (P = 0.12).
Discussion
In this cross-sectional population-based study there was a statistically significant trend towards lower headache prevalence rates in the groups with low haemoglobin levels (Table 2). The groups with high or low values were relatively small, so these findings have to be interpreted with caution. The 2385 participants included in this study were selected randomly among non-pregnant, non-blood donor females aged 20–55 years collected from the general population. Therefore, it seems unlikely that selection bias can explain these positive findings. The fact that headache was not the primary objective of HUNT makes selective participation due to headache unlikely.
The questionnaire-based headache diagnoses have certain limitations. The headache questionnaire had to be adapted to the other questions in HUNT. We classified the headache diagnoses into only two types. The potential problems related to such diagnostic instruments, including a risk of misclassification, were evaluated by comparing the questionnaire-based headache diagnosis with diagnosis made in clinical interview (14). Although 80% of the non-migrainous headaches were of the tension type (14), this category is a mixture of different headache types. Probably, due to diagnostic inaccuracy, there were migraine patients in the group of non-migraineurs and vice versa, making the two groups more similar than they really were. Consequently, differences between migraineurs and the non-migrainous headache sufferers may have been underestimated rather than overestimated.
The lack of association between headache and ferritin seems to be in accordance with previous results (11). In the epidemiological study of headache prevalence and hereditary haemochromatosis no relationship between transferrin saturation and headache prevalence was found (11). The relationship between haemochromatosis and headache prevalence was strongest for women with both genotypic and fenotypic haemochromatosis, suggesting that the high headache prevalence in haemochromatosis is related to the genotype rather than the iron overload per se (11). Welch et al. reported elevated iron levels in the periaqueductal grey matter of patients with migraines and chronic daily headache (7), but ferritin levels were not measured.
Since the association between headache and haemoglobin is not related to iron stores, one may speculate that it is related to viscosity. Although we did not measure viscosity, there are some observations indicating that elevated haemoglobin values may induce headache by increasing blood viscosity. In polycythemia vera headache is one of the most common symptoms (6–8), and it is thought to be caused by hyperviscosity which induces disturbed microcirculation (7, 8). The increased viscosity is probably due to the increased haematocrit, but other factors such as increased adhesion of thrombocytes and erythrocytes may also contribute (8). Phlebotomy and normalization of blood chemistry often relieve headache (9).
In chronic mountain sickness also, headache is thought to be caused by both hypoxia and elevated haemoglobin values (10). Increased viscosity due to the elevated haemoglobin values and hypoxia reduces oxygen delivery to the tissues, and in the brain this may alter the levels of various neurotransmitters (16).
Headache has also been observed in anaemic renal failure patients after treatment with recombinant human erythropoietin (17, 18). The reason for this may be either increased blood viscosity or increased blood pressure (17, 19).
In addition, one study has reported increased blood viscosity in migraineurs, although the haematocrit was within normal limits in this study (20).
In the present study there are no indications that iron deficiency, either with or without anaemia, results in headache. We cannot, however, draw any conclusions about the association between very low haemoglobin levels and headache, since very few women had extreme values. Two previous studies have failed to demonstrate any relationship between anaemia and headache, but in these studies also the number of subjects with very low haemoglobin values was small. Only eight out of 295 persons (4) and 14 out of 82 (5) had haemoglobin levels < 10.0 g/dl. Furthermore, in the latter study only 298 out of 1462 women were interviewed about headache (17 anaemic women and 281 women with haemoglobin values within normal range) (5). One study among 515 pregnant Liberian women reported a positive association between headache and anaemia. In this study nearly half of the population had haemoglobin values <10 g/dl and 6.4% had haemoglobin values <8 g/dl (3). Women who reported headache had significantly lower mean haemoglobin values than women without headache (3). In severe anaemia with haemoglobin level < 7 g/dl other mechanisms, such as hypoxia and the resulting intracranial vasodilatation, may explain the occurrence of headache (21).
The association between haemoglobin levels and headache found in this population-based study is relatively weak. The finding may, however, be more important in certain subgroups of headache patients. Further studies should therefore investigate various haematological and rheological parameters in the groups of headache patients. This could be most important, since many of these parameters are amenable to therapeutic intervention.
Footnotes
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre, Faculty of Medicine, Norwegian University of Science and Technology (NTNU), Verdal, Norwegian Institute of Public Health, and Nord-Trøndelag County Council.