
Abstract
Using data from a cross-sectional survey and a prospective record linkage study the aims of this study were to: (i) determine sources of advice and care for headaches in a population survey of adults, and (ii) investigate prospectively the influences of headaches on general practice consultation in a 12-month follow-up of the responders to the population survey. A population based cross-sectional survey was mailed to 4885 adults (aged ≥ 18 years) with an adjusted response rate of 56% (n = 2662). The main outcome measures of interest were (i) self-report advice and care-seeking in the survey (ii) consultation with general practitioner for headache and for other conditions in 12-month period subsequent to the survey. Reporting a recent GP consultation for headache was associated with younger age (mean: 46 vs 48 years), female gender (68% vs 60%), and greater headache severity as measured by frequency, pain, and associated disability. The commonest sources of advice and care in the past were GPs (27%), opticians (21%), and pharmacists (8%). Consultations for headache were not common in the 12-months following the survey (n = 144); however, those reporting a recent headache were almost 4 times more likely to consult subsequently with a headache than those not (relative risk; 95% CI: 3.7; 1.9, 7.0). Recent reporting of headache was also associated with an increased risk of consulting for mental disorders (1.7; 1.2, 2.6), diseases of the digestive (1.6; 1.1, 2.3) and respiratory system (1.4; 1.1, 1.8), and a decreased risk of consulting for circulatory diseases (0.8; 0.7, 1.0). Only a minority of headache sufferers consult their GP, regardless of severity, with opticians and pharmacists being other important sources of information. Headache appears to have an additional impact upon GP workload through increased rates of consultations for nonheadache conditions amongst headache sufferers. The interesting findings regarding rates of consultation for digestive and circulatory conditions amongst headache sufferers may be linked to the use of headache medication.
Introduction
Although the occurrence of a headache at some point in life appears almost inevitable (1), the majority of sufferers do not seek advice from health care professionals (2–4). Data from the 4th national study of Morbidity Statistics from General Practice in the UK (5) suggests that consultations for back pain (37 per 1000 adults per year) are more than twice as common as consultations for headache (14 per 1000 adults per year) despite a greater lifetime incidence for headache (1, 6, 7). Understanding the reasons why only certain sufferers seek advice and from whom and why the advice is sought, may help future planning and provision of services, and influence how advice is disseminated to the public.
Moreover, differences in characteristics between sufferers who do and do not seek advice from health care professionals may also improve our understanding of headache-related consultation. Previous studies have found that females are more likely to seek advice then males (3, 4) though evidence regarding the influence of age is conflicting (5, 8). Health-care seeking is also more likely to occur in those with more severe headaches (8, 9) or those who also report comorbid conditions, including anxiety and depressive disorders (10–13). However, much of the available evidence in this field is restricted to migraine sufferers who represent the minority of all headache sufferers in the general population.
Using data from a cross-sectional population-based survey and a prospective record linkage study, we have investigated sources of advice and care for headache, the main reasons for seeking health care advice, and how sufferers who do seek health care differ from those who do not.
Methods
There were 3 phases to this study. Phase 1 was a population survey. Phase 2 was a prospective study, using practice records, of the consultations sought with general practitioners (GPs) by survey responders in the subsequent 12-month period. Phase 3 was a small validation study to compare self-reported consultations with a GP as recorded by self-report in the baseline survey with information on such consultations obtained from a retrospective review of practice records.
Phase 1: population survey
A population-based postal survey was carried out in one district of the UK (the North Staffordshire Headache Survey). Details of the survey methodology and questionnaire content have been presented elsewhere (6, 14). Ethical approval for the study was obtained from the Local Research Ethics Committee. In summary, 1000 adults, aged 18 years and over, were randomly selected from the population registers of each of five local general practices. In the UK, about 98% of the population are registered with a GP, hence practice registers provide a convenient frame for sampling a local population (15). After exclusions made by the GPs, the questionnaire was mailed to a 4885 sample enquiring about headaches and general health. Additionally, respondents were asked for consent to access their general practice records. After a three stage mailing procedure, an adjusted response (allowing for incorrect contact information and deaths) of 56% was achieved (n = 2662). The responders were 56% female, had a mean age of 52 years (range 18–98 years), and were almost exclusively Caucasian (99.3%).
The survey asked participants whether they had experienced a headache in the previous 3 months (‘recent’ headache) and separately whether they had ever experienced one in their life. For each of these time periods, those suffering from headaches were asked to recall whether they had sought advice for their symptoms. Recalled information was gathered for consultations with health care professionals (hospital specialist, general practitioner, dentist, optician, pharmacist) and advice sought from family, friends and other sources. Respondents recalling a consultation were given a list of possible reasons for seeking advice and asked whether each had been an influence on their most recent decision to consult. For those recalling a consultation with either a general practitioner or pharmacist, the importance of different areas of information covered in their most recent consultation, was rated on a 5-point Likert scale ranging from ‘not important at all’ to ‘very important’.
Those who reported a ‘recent’ headache were asked for descriptions of their headaches in terms of frequency, duration, and pain, together with symptoms associated with their headaches (6). The effects of these characteristics were then measured in terms of actions taken, medication or other therapies used, and disability, using the Migraine Disability Assessment (MIDAS) (16). In addition, respondents’ headache severity was classified on a combined scale using reports of headache pain and disability based on Von Korff's chronic pain rating system (17), as follows: 0 = no headache; I = mild disability and none or mild pain; II = mild disability and moderate pain; III = mild disability and severe or extremely severe pain; IV = moderate disability and any pain level; and V = severe or very severe disability and any pain level. Respondents were asked to report whether they had experienced any of nine symptoms with at least some of their recent headaches (unilateral pain, pulsating pain, pain worse with movement, nausea, vomiting, photophobia, phonophobia, visual disturbances, numbness). These symptoms were chosen to reflect the International Headache Society (IHS) migraine criteria (18) and sufferers reporting 5 or more symptoms were classified as ‘likely migraineurs’.
The Hospital Anxiety and Depression scale (HADs) was completed by all participants (19). The tool has been designed for use as a screening device and validated as a self-complete questionnaire. The scores for anxiety and depression have been calculated separately with higher scores indicating more severe symptoms.
Phase 2: prospective study of consultations
Data was downloaded, for those respondents who gave consent, concerning all consultations occurring with a GP in the 12-month period subsequent to the survey. This information was collated to determine for each subject (i) the total number of consultations for any reason (ii) the number of consultations relating to headaches (Appendix A), and (iii) whether or not a consultation had occurred within each of 16 diagnostic categories in this 12-month period. These categories were defined from the disease classification known as the Read Code system, a hierarchical directory of symptoms and morbidities widely used in the UK NHS for coding purposes. The study practices are all members of the North Staffordshire GP Research Network and all use this system as part of their computerized morbidity coding of consultations. For this study, the broad classification level of the coding system (cardiovascular, respiratory, etc.) was used: a level which goes by letter from A to R. Headache consultations were separately identified (Appendix A).
Information from the baseline questionnaire was linked to the general practice data, via a unique practice identification number provided by the software system used by all participating practices (the Electronic Medical Information System (EMIS) system), and all data was anonymised.
Phase 3: validation of self-reported consultations for headache
Using one of the study practices, two random samples of 25 survey responders were generated: (i) those who reported consulting their GP because of headaches in the last 3 months, and (ii) those who reported they had not consulted. The GP records relating to this period were then reviewed by one researcher (HO), who was blinded to the individual's recalled consultation status, to determine whether a headache consultation had occurred in the 3-month period immediately prior to the survey, or, if not, whether a consultation had occurred within the previous ear.
Statistical analysis
From the survey, frequencies and percentages of the occurrence of self-reported advice and care seeking (ever and ‘recent’), reasons prompting consultation and importance of factors within a consultation were calculated. Within those reporting a ‘recent’ headache, cross-tabulations are presented for demographic and headache characteristics (disability, frequency and pain intensity) against self-reported recent consultation with a health care professional. The cross–sectional associations are presented as odds ratios and 95% confidence intervals.
Survey data was linked with the prospective general practice data to determine predictors of consultation. Firstly, associations between ‘recent’ headache and subsequent consultation (any, individual Read code categories (A-R), headache specifically) were examined. Secondly, the association between baseline characteristics and subsequent consultation for headache among those with a recent headache were examined. This analysis was carried out only in those subjects reporting a recent headache as recent headache characteristics were felt to be important determinants of future consultation. A multivariate modelling procedure was used to determine factors that were independently associated with subsequent headache consultation. The prospective associations are presented as risk ratios and 95% confidence intervals. All analyses were performed using Stata 6.0 (20).
Results
Phase 1: population survey
This section concerns those respondents in the baseline survey who reported that they had experienced a headache ever(93% of responders; 1061 males, 1405 females) or ‘recently’, i.e. within the past 3 months (70%; 729 males, 1142 females).
Source of advice
Approximately half of the respondents who reported ever suffering from a headache had sought advice for their symptoms from at least one source (n = 1209; 49%). Most had sought advice from a health care professional (n = 991); general practitioners (n = 659, 27%), opticians (n = 527, 21%), pharmacists (n = 203, 8%), and hospital specialists (n = 170, 7%) were the commonest sources (Table 1). 575 respondents (23%) had sought advice from nonhealth care sources (family member, friend, or work colleague).
Sources of advice for headaches

Approximately one in 5 respondents reporting a headache in the 3 months prior to the survey recalled they had sought advice in this time (n = 384; 21%). This recent health care advice had been commonly sought from GPs (n = 142), pharmacists (n = 60) and opticians (n = 57), and more than half of the respondents had recalled seeking advice from family members or friends (n = 204).
Reasons for, and expectations of, consultations
Many respondents wanted information about their headaches, such as to know the cause (n = 391), whether there was a cure (n = 321), or what medicines they should use (n = 292). Particular aspects of headache appeared to be drivers for consultation; increase in the number of headaches (n = 298), increase in the pain from headaches (n = 151), concomitant symptoms experienced with headache (n = 264), and the general pain intensity (n = 241). Interference with life was another common reason for seeking advice; this included impaired work or household activities (n = 257), family or social role (n = 178)).
Respondents were asked to rate the importance of several factors in their most recent consultation with either a GP or a pharmacist (Table 2). In a general practice consultation, the majority of sufferers rated the following as of importance: explanation of headache, relief of pain, and time to ask questions. Having a medicine prescribed, being given an explanation of the medicine, and the need for further tests were rated as less important. By contrast, in a consultation with a pharmacist, respondents were less likely to rate gaining an explanation for their headache as important, and most rated advice on which medicine to buy, relief of pain, explanation of the medicine, and time to ask questions as important.
Perceived importance of factors in most recent consultation with either a GP or a pharmacist

Comparisons of sufferers who did and did not seek advice for a recent headache
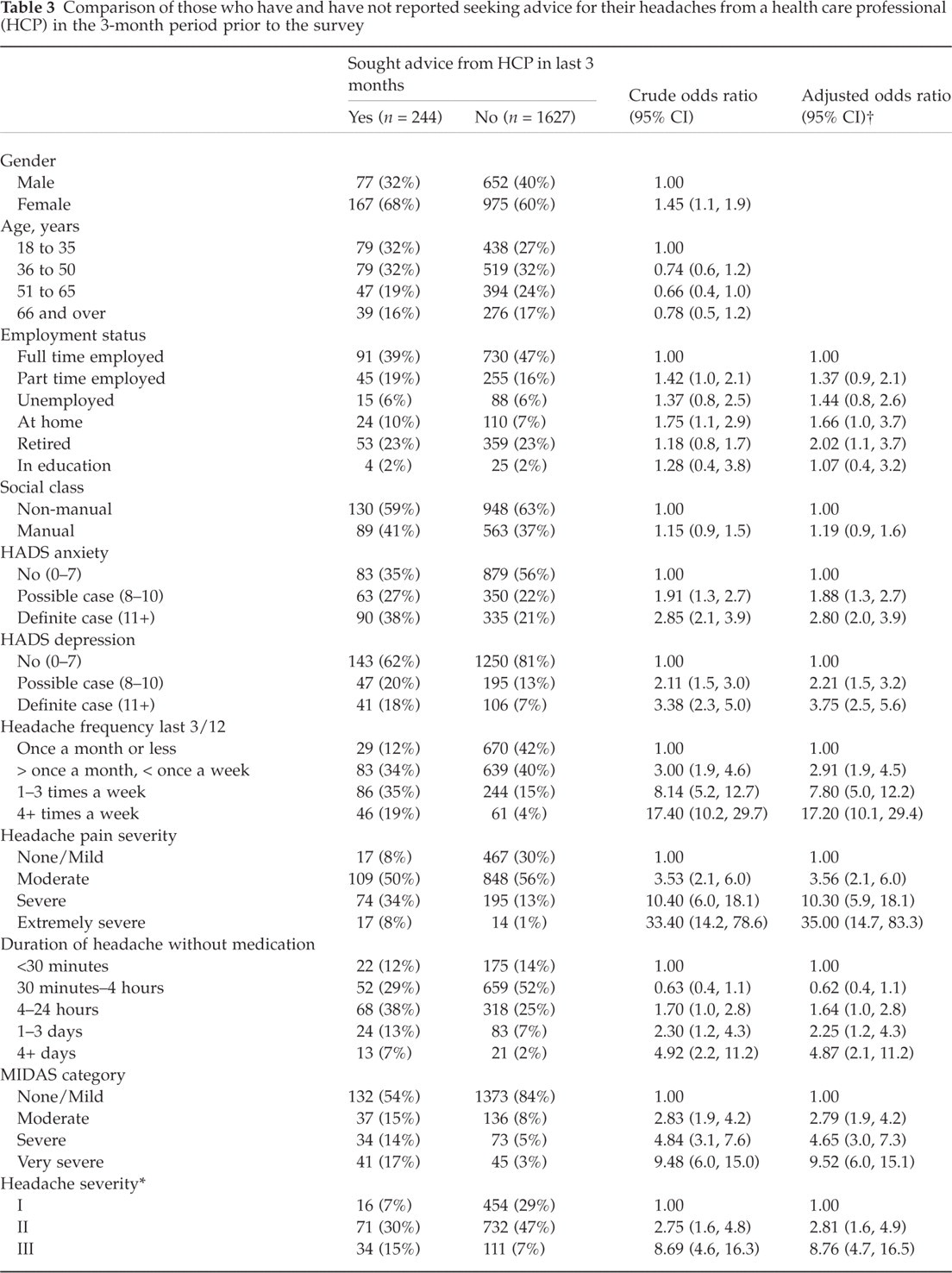
Those who recalled seeking advice from a health care professional for a recent headache were significantly more likely to be female, younger and not in full-time employment, but there was no effect with social class (Table 3). Sufferers recalling a recent consultation had higher anxiety and depression scores compared with those who had not sought advice. Recent headache characteristics in terms of higher frequency, longer duration, and more severe pain and disability were also strongly associated with seeking advice. Being classified as a ‘likely migraineur’ also conferred an increased likelihood of having sought advice.
Comparison of those who have and have not reported seeking advice for their headaches from a health care professional (HCP) in the 3-month period prior to the survey

Von Korff severity grading,
Adjusted for gender and age group.
Phase 2: prospective study of consultations
Of the 2662 responders to the survey, 2192 gave consent for access to their medical records. Headache, as a reason for consultation, was recorded in only 144 participants (6.5% of those undergoing record review) in the 12-months after the survey. Among these consulters, the average number of consultations for headache in the year varied, although most respondents (n = 108) had only one consultation (median = 1, range = 1–9). The proportion consulting with a headache was higher in those with a recent headache at baseline (8%) than in those who had been headache-free (2%), and four times as high in those with a prior history of headache consultation at baseline than in those with no such recall (16.8%vs 3.1%). For 35% of respondents, the consultation in the year subsequent to the survey was the first time they had consulted their GP because of a headache, assuming their recall at baseline to be valid.
The total number of consultations, for any reason during that year varied widely between respondents (median = 3, range = 1–29). Those with a recent headache at baseline were at an increased risk of consulting for any reason (Table 4). Too few consultations occurred in Read chapters D (blood diseases) and L (diseases associated with pregnancy) to allow for meaningful analysis. The crude risk ratios suggested several Read chapters occur more frequently in those with a recent headache at baseline. When adjusting for differences in age and gender between those with and without a recent headache, a moderate increase in risk (30–40%) was seen for consultations about diseases of the nervous (F), respiratory (H), and musculoskeletal system (N) and a more substantial elevation in risk (60–70%) for consultations about mental disorders (D) and digestive system diseases (J). Prior recent headache at baseline was associated with a modest reduction of risk for consulting for a circulatory system disease (G).
Increased risk of consulting within specific Read chapter in 12-month period subsequent to survey: Effect of ‘recent’ headache

95% confidence interval,
Calculated over gender and age group (≤50 years, ≥51years).
An adapted Von Korff severity grading for the self-reported headache symptoms in the 3-month period prior to the survey could be assigned to 2125 participants – 97% of those with a ‘recent’ headache (Table 5). No clear pattern emerged regarding the likelihood of consultation for any problem in the subsequent year and baseline headache grade. However, for consultations related to headache, the percentage of respondents seeking help increased with headache grade from 2% among those with no headache to 22% among those with the most disabling and painful headaches.
Headache classification at baseline and the likelihood of consultation in the 12-month follow-up period (n = 2125)

Median (IQR).
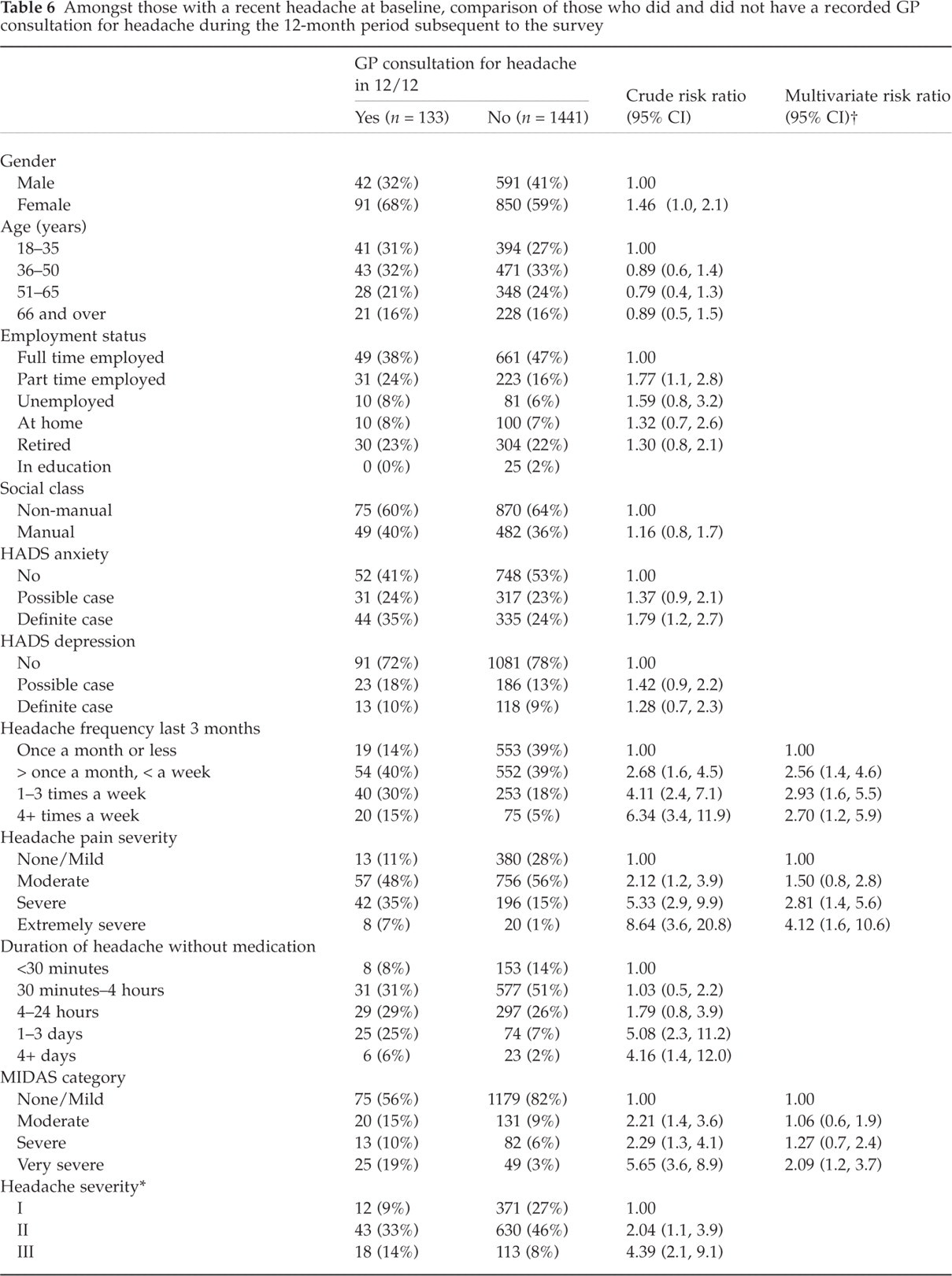
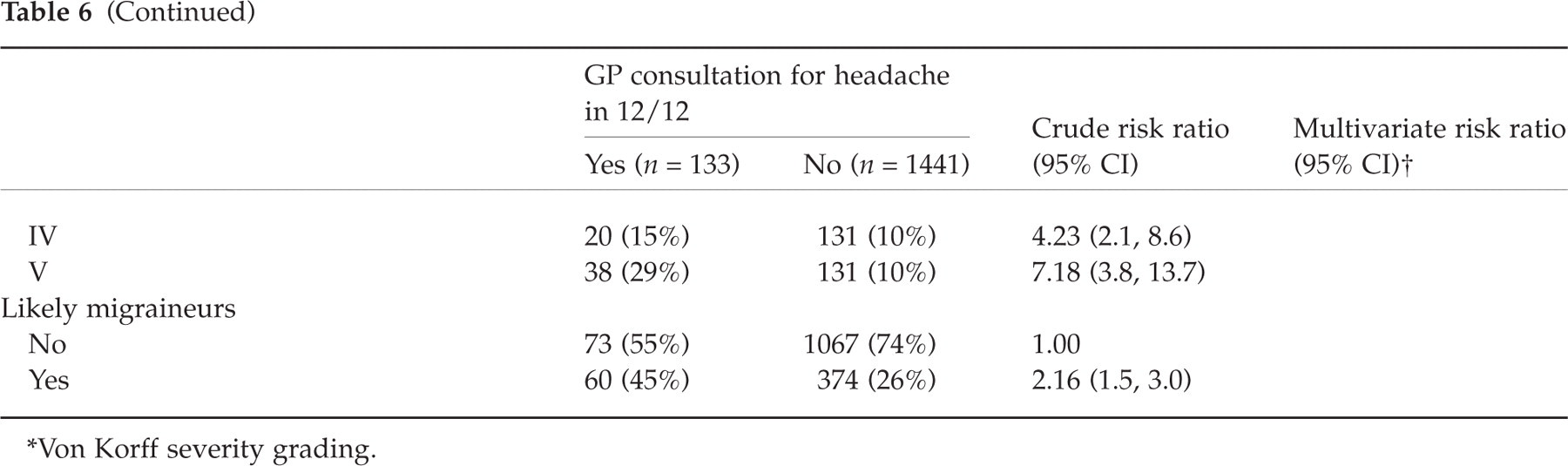
The prospective analysis produced similar results to the cross-sectional data though, for a particular relationship, the risk ratios calculated tended to be reduced compared to the corresponding baseline prevalence odds ratio. In the multivariate modelling procedure three baseline factors (headache frequency, headache pain severity, and MIDAS grade) were independently associated with the occurrence of a headache consultation occurring in the 12-months subsequent to the survey (Table 6).
Amongst those with a recent headache at baseline, comparison of those who did and did not have a recorded GP consultation for headache during the 12-month period subsequent to the survey
Von Korff severity grading.
Likely migraineurs
Sub-group analysis was carried out on those headache sufferers classified as ‘likely migraineurs’. Similar findings regarding predictive factors were found for likely migraineurs as those in for all headache sufferers (Table 2). Specifically, a higher percentage of migraineurs rated ‘relief of pain’ as important in a GP consultation and ‘advice on medication’ and ‘explanation of medication’ in a consultation with a pharmacist. The percentage of likely migraineurs consulting for headache in the 12-months following the survey was 14%, a similar figure to those sufferers with a severe headache grade (von Korff grade III–V, Table 5).
In a complementary analysis to that presented in Table 4, comparing the likely migraineurs to those reporting no recent headache at baseline, stronger relationships were seen with consulting for headache (risk ratio; 95% CI = 7.16; 3.6, 14.2), mental disorders (2.68; 1.8, 4.0), digestive disorders (1.94; 1.3, 2.9), and circulatory diseases(0.50; 0.4, 0.7).
Phase 3: validation of self-reported consultations for headache
Computerized records for all 50 respondents were searched for the 3-month period prior to the survey. Of the 25 respondents who reported they had not consulted, none had a record of a headache consultation. Of the 25 respondents reporting a consultation occurring in 3 months prior to the survey, 6 had evidence in the computerized records of a consultation for headache in that period. In a further search, extended to the 12-month period prior to the survey, evidence of a headache consultation was found for an additional 3 respondents. Hence a total of 9 respondents (from 25 who reported a recent consultation) had a record of a consultation for headache within the past year.
Discussion
Seeking advice for headaches is common, with half of sufferers reporting that they had ever sought help from others. The commonest sources for advice and care were GPs, opticians, and family and friends. Reporting a recent consultation with a health care professional because of a headache was more common amongst women and the younger age-group. Higher anxiety and depression scores were also associated, cross-sectionally, with recall of recent consultation. Not surprisingly, severity of recent headache, i.e. within the previous three months, in terms of frequency, pain, and associated disability, were also associated with recalling a consultation.
In terms of prospective health care-seeking behaviour, participants who reported a recent headache were at increased risk of subsequently consulting their GP during the following 12 months because of headaches, and also because of mental disorders and symptoms and diseases of the respiratory, nervous, and musculoskeletal systems. By contrast headache sufferers had a reduced risk of consulting for circulatory system diseases. Headache characteristics were the strongest predictors of subsequent consultation for headache among those with a recent headache at baseline.
In consultations with GPs, sufferers rated an explanation for the headache and advice on pain relief as the most important factors. These findings from primary care are similar to those in a study in a neurology outpatient department in which patients first wish was to know the cause of their headaches, followed by pain relief, findings contrary to the beliefs of the physicians surveyed in the same study (21). These are consistent with other findings suggesting that patients are as interested in having the opportunity to ask questions about headaches and medications as they were in obtaining pain relief (22, 23).
Large numbers of respondents reported seeking advice about their headaches from opticians, which may be related to the location of the headache or worry about their vision. This finding is worth highlighting since it means that opticians represent a potentially important source for headache advice, and, given the high prevalence of the condition, headache sufferers may constitute a significant proportion of their caseload. A much lower number of sufferers sought advice from a pharmacist with the main driver for advice being medication. Sufferers appear to expect doctors to explain headaches and pharmacists to medicate.
An increased likelihood of consultation in women has been reported in other headache studies (2–4, 9, 24) and studies of other pain syndromes such as low back pain (7), chronic widespread pain (25), and shoulder pain (26). Our finding that consultation decreases with age was also reported in a UK study of consultation for migraine (5). However studies of headache or migraine outside the UK have, by contrast, found consultation rate increases with increasing age (8, 9, 11, 24). Anxiety and depression scores were strongly associated cross-sectionally with the recalling of a recent consultation. However, the prospective association between pre-existing anxiety/depression and subsequent consultation was weaker and the multivariate analysis suggests these were not important, independent predictors.
Although severity of symptoms was related to the recall of a consultation for headache, as also found in many other studies (8, 9, 24, 27), most respondents neither recalled a consultation nor had a consultation for headache recorded prospectively. Hence, in those with the most severe symptoms (von Korff grade V), only 1 in 4 respondents recalled a consultation with a GP in the 3-month period prior to the survey and only 1 in 5 had a recorded consultation with a GP for headache in the 12 months subsequent to the survey. These figures reflect findings from migraine studies where large numbers of sufferers have never consulted anyone for their symptoms, despite suffering from a condition associated with severe pain and related disability (28–31). To fully understand the relationship between headache and health-care seeking, the reasons why sufferers do not consult for symptoms need to be investigated. This was an area that our study did not cover, although available evidence from migraine studies suggests that inconvenience, believing doctor could not help, and the availability of effective treatment without prescription are reasons for not seeking advice (32, 33). The reporting of a recent headache was only modestly associated with a consultation for any reason in the subsequent 12-months, but was strongly associated with consultations for headache in that period. Moreover, consultations for several of the specific Read code chapters were also associated with the presence of a reported recent headache. Findings for the subgroup classified as ‘likely migraineurs’ were consistent with this. The Read codes used to define a consultation for a headache include several diagnosis codes from the nervous system diseases and mental disorders chapters. Hence, some increase in risk of consultations within these chapters would be expected. Moreover, when respondents were stratified into ‘anxious’ and ‘nonanxious’ using the Hospital Anxiety and Depression scale (19) in the baseline survey, the association of consultation for a mental disorder and recent reporting of headache was found only in those who were classified as having possible or definite anxiety (2.22; 1.2, 4.4) and not in the noncases (0.88; 0.5, 1.6).
One putative explanation for the increased risk of digestive disorders and decreased risk of circulatory disorders could be related to medication use. Certain medications taken to relieve pain in general (aspirin and ibuprofen containing medications, and other nonsteroidal anti-inflammatory drugs) are associated with increased gastric symptoms (34) and reduced risk of circulatory conditions (35). In a stratified analysis, headache sufferers were split into those who did and did not report taking any of the above named medicines for their headache and then compared with the headache-free group. The risk of consulting for circulatory disorders was reduced in both headache groups compared to those with no headache, but was lower in the ‘medication’ group (0.62; 0.4, 0.9) than in those not taking these medicines (0.88; 0.7, 1.1). The risk of consulting for digestive disorders was increased in both headache groups, but was higher in the ‘medication’ group (2.08; 1.2, 3.5) than in those not taking these medicines (1.55; 1.0, 2.3). These are interesting findings, but would require further investigation in order to demonstrate a causal relationship.
The study practices were chosen because they are fully computerized and have good record keeping, with the latter being monitored though annual audits to assess the proportion of consultations that are coded to the Read system. Despite this, the agreement between self-reported consultation and the information from their medical records was poor, although good for respondents reporting no consultation. This finding has been reported previously in other pain conditions such back pain (36) and knee pain (37). There are several potential reasons for this disagreement. Firstly, the self-reported data could be affected by recall bias, including the tendency to ‘telescope’ illness events into the recent past. The disparity between the two sources of data in the present study was reduced after the time-period of the record review was extended from 3 to 12-months, although discordance was still greater than 60%. Jinks et al. (37) showed that by extending both the time-period (from 1 to 3 years) and the anatomical area (from knee to leg or knee) discordance in knee-pain sufferers was reduced substantially from 50% to 6%. Secondly, in consultations where multiple complaints are discussed, there is evidence to suggest that GPs record only what they perceive to be the main complaint of the consultation. It may be that the headache symptoms were a secondary complaint or were side-effects from medication. However, this perception may be at odds with the patients’ perceptions of the content of the consultation. In general it is unlikely that this issue would affect the associations we have reported, particularly in the prospective study, although the actual GP consultation frequency for headache remains uncertain.
This study was designed to capture data on all headache types combined and the potential to categorize headache sufferers as ‘migraineurs’ is limited. However, in order that we may compare our study data to that currently available in the literature, we felt it was necessary to be able to obtain a crude, epidemiological definition. Although in using our definition we cannot say that all accompanying symptoms were experienced in the same headache episode, those with five or more symptoms could be described as ‘likely migraineurs’. Compared to other European studies using the complete IHS criteria to assess the prevalence of migraine (1, 11, 38) our method produces an estimate (18.2% of the survey responders cf 10–13%) that is higher.
Whilst headache severity was associated with subsequent primary care consultation, most sufferers across all degrees of severity did not seek professional help for their symptoms. However, headache sufferers do appear to have increased rates of consultations for nonheadache conditions. Health care professionals who are seeing patients with headache need to be aware of sufferers’ desire to understand the cause of their headaches and should provide advice appropriately. Results from the comparison of self-reported and recorded consultations for headache suggest that patients’ medical records and patients’ own recall of consulting are providing rather different measures of access to health care.
Footnotes
Acknowledgements
We would like to thank the North Staffordshire GP Research Network for their assistance with the study. We would also like to thank the network team and administrative staff from the Primary Care Sciences Research Centre and administrative staff from the Department of Medicines Management, Keele University for their help and support with the study. Baseline survey costs were funded by the Proprietary Association of Great Britain. The costs of the follow-up surveys and consultation data follow-ups were funded by the North Staffordshire Primary Care Research Consortium.
Appendix A
List of Read codes (Version 5) used to define headache from general practice records