
Abstract
Migraine and tension-type headache (TTH) can increase in frequency and transform from episodic to chronic forms. The process of transformation of these primary headaches is complex and involves multiple risk factors. In this cross-sectional and longitudinal population study, we aimed to investigate the relation of clinical characteristics of primary headaches to poor outcome: new-onset or persistent chronic headache (≥180 days/year). Individuals who had migraine + / − TTH and those who had pure TTH were studied separately. Of 740 individuals who entered this study in 1989, 673 were eligible for follow-up in 2001, and a total of 549 individuals participated in the follow-up study. At baseline in 1989, no difference was found between episodic and chronic migraine headache ( + / − TTH). Duration of headache episodes >72 hours (p = .002) was associated with pure chronic TTH at baseline in 1989 whereas aggravation of headache by physical activity (p = .045) was associated with pure frequent episodic TTH. Of 64 subjects with migraine + / − TTH, 12 had a poor outcome in 2001. For pure TTH, of 116 subjects at baseline, 11 had a poor outcome in 2001. Using multivariate logistic regression analysis with adjustment for medication overuse and use of preventive medications, poor outcome of migraine + / − TTH tended to be associated with a baseline pulsating quality and severe intensity of migraine, photophobia and phonophobia, as well as longer duration of an individual headache attack. For pure TTH, unilateral headache, nausea and individual headache attack duration greater than 72 hours was associated with poor outcome. Pooled data univariate analysis revealed that nausea, daily use of acute headache medications, use of headache preventive medications and coexistent headaches were significant predictors of chronic headache in 2001(p<.05). In conclusion, our study demonstrates that certain clinical characteristics of headaches are associated with poor outcome but alone may not predict the chronification of migraine or TTH.
Introduction
Both migraine and tension-type headache (TTH) can increase in frequency and transform from episodic to chronic form. The prevalence of chronic migraine (CM) and chronic tension-type headache (CTTH) are estimated at approximately 1%–3% (1,2). Although the prevalence of these chronic headaches is low compared to the prevalence of episodic migraine and TTH, both of these chronic headache types are associated with a higher degree of burden on the individual and society (3–5). The pathophysiology of the transformation of migraine and TTH to chronic forms has not been fully clarified, but development of central sensitization or increased excitability of the trigeminal nociceptive pathways may play a major role in the pathophysiology of both primary headaches (6,7).
Recent epidemiological research has focused on factors that are associated with transformation from episodic to chronic forms. Risk factors have been divided in to two groups: modifiable and not readily modifiable (8,9). Not readily modifiable risk factors include age, female sex, white race, low educational level or socioeconomic status, genetic factors and head trauma (10–12). Modifiable risk factors include psychiatric comorbidities, sleep disturbances, overuse of headache abortive medications and obesity (11–13). It was our hope that, by identifying and preventing risk factors, we would be able to halt the process of transformation of migraine and TTH to chronic forms in patients.
It is unknown whether clinical characteristics of migraine and TTH, which constitute headache features and associated symptoms, may be of prognostic value in the transformation of both conditions. In a recent study (14) severe baseline pain and nausea were reported to be independent predictors of poor pain and functional outcomes 24 hours after emergency department discharge in both patients with migraine and patients with TTH. In this study, severe baseline pain intensity was a predictor of moderate or severe headache in the 24 hours after discharge from the hospital. Severe headache pain and the presence of photophobia, phonophobia and nausea have been demonstrated to be predictors of failure to achieve a two-hour pain-free response in migraineures after the administration of triptan (15,16). Moreover, severe headache intensity and longer duration of headache have also been shown to be risk factors for the recurrence of migraine after treatment with triptan (17,18). These studies suggest that baseline headache characteristics may predict the future outcome of migraine and TTH. In this epidemiological study, we aimed to compare clinical characteristics between episodic headache (migraine with/without TTH) and chronic headache (migraine with/without TTH), and between pure frequent episodic TTH and CTTH. We also aimed to investigate the relation of clinical characteristics of episodic migraine and TTH to poor prognosis or chronification of migraine and TTH later in life.
Methods
Sample
In 1989, 1000 residents in the County of Copenhagen, aged 25 to 64 years, were randomly chosen from the Danish Civil Registration System. All residents in Denmark are registered in the Danish Civil Registration System with a unique 10-digit code. Therefore, this sampling method ensured the selection of a random sample of the general population. Two medical doctors conducted all headache-diagnostic detailed clinical interviews. Of 975 eligible subjects, 740 (76%) participated. The age and gender distribution of the participants was representative of the cohort and the background population. Both methods and results of the 1989 study are described in detail elsewhere (1).
In 2001, a follow-up study of the cohort from 1989 was conducted, including all subjects who in 2001 were alive, residing in Denmark and capable of answering written and verbal questions. No intervention was made during the follow-up period. All eligible subjects in the 1989 cohort, now aged 37 to 76 years, were identified through the Danish Civil Registration System and invited to participate in an extensive investigation with an emphasis on primary headaches, including a detailed clinical headache interview. If subjects did not respond to the invitation, they were contacted and asked to complete a headache interview by telephone. All interviews and examinations during the follow-up study, including the telephone interviews, were conducted between May 2001 and April 2002 by one medical doctor (AL).
The study was carried out at the Research Centre for Prevention and Health at Glostrup Hospital, University of Copenhagen, and approved by the Ethical Committee for Copenhagen County and the Danish Data Protection Agency. Informed consent was obtained from each participant before the interview.
Survey and headache diagnosis
In 1989, each distinct form of headache was diagnosed according to the International Headache Society’s 1988 classification and diagnostic criteria for headache disorders (ICHD-1) (19). The survey included questions on headache features (attack duration, localization, intensity and aggravation by physical activity) and associated symptoms (nausea/vomiting, photophobia, phonophobia and osmophobia). The 1989 survey also included questions on demographic data (age and gender), daily use of abortive or acute headache medications and use of headache preventive medications. The 2001 study used similar procedures, questions and wording as did the 1989 study. The headache interviews included an extensive description and diagnosis based on the ICHD-I criteria of each different form of headache. All participants were questioned specifically about headache with migraine and TTH features. The interviewer had no knowledge of the headache diagnoses from 1989. The telephone interviews were conducted with the same ICHD-I diagnostic criteria, interviewer, data collection period, interview questions and sequence as the face-to-face interviews, including all interview questions necessary for diagnosing migraine and TTH.
Headache group definitions
Two groups were identified:
Group 1. Migraine with/without TTH. Episodic headache was defined as migraine with/without TTH occurring <180 days/year. Episodic migraine and TTH in 1989 and 2001 were diagnosed according to ICHD-II (ICHD, 2nd edition) (20). Diagnosis of CM based on recently revised ICHD-II appendix criteria for CM (21) could not be made by using our questionnaire in 1989. Instead, individuals who had ≥180 headache (both migraine and TTH) days/year in 1989 and 2001 were given a diagnosis of chronic headache. Individuals with infrequent TTH were diagnosed as subjects with no headache.
Group 2. Pure TTH. Using ICHD-II, pure TTH was subdivided into infrequent episodic TTH (1–14 headache days/year), frequent episodic TTH (15–179 headache days/year) and CTTH (≥180 headache days/year).
Data analysis
Statistical analyses were performed using SPSS software, version 16.0 (SPSS Inc. Chicago, IL, USA). Five percent was accepted as the level of significance. Data from individuals in group 1 and group 2 were summarized using frequency counts with percentages and descriptive statistics such as means and standard deviation (SD). Subjects’ age (ordinary variable) was coded in five categories: 25–34; 35–44; 45–54; and 55–64.
Cross-sectional analysis
Cross-sectional analysis included the χ2 test for comparison of headache characteristics in 1989 among episodic and chronic subgroups. The infrequent episodic TTH group was not used in the analysis. The logistic regression model was used for analyses of ordered categorical variables such as age ranges, headache frequency, duration and intensity of headache attack. In addition, migraine frequency was divided into groups: low (<14 headache days/year) and high (≥14 headache days/year).
Longitudinal analysis
The prognosis of migraine with/without TTH (group 1) was assessed for subjects with migraine attacks within the last year before the 1989 baseline interview (one-year prevalence period). Poor outcome or chronification of migraine with/without TTH was defined as ≥180 headache days/year at follow-up in 2001, due to either increased frequency since 1989 or persisting high frequency of headache. The remaining group was defined as having a good outcome in 2001, with unchanged low frequency since 1989 or decreased headache frequency to <180 days/year or remission, that is, no migraine or TTH attacks (infrequent episodic TTH allowed) in the preceding year. Subjects who reported no migraine and/or infrequent episodic TTH in 2001 and did not recall their last migraine (nine subjects) were assumed to have experienced remission.
For pure TTH (group 2), prognosis was assessed for subjects experiencing frequent episodic TTH or CTTH at baseline in 1989. Poor outcome or chronification of TTH was defined as ≥180 TTH days/year at follow-up in 2001 due either to increased frequency from episodic TTH at baseline into CTTH or to unremitting CTTH. The remaining group of subjects with good outcomes included participants with frequent episodic TTH or with remission (no or infrequent TTH at follow-up in 2001). Subjects who did not report TTH in 2001 and did not recall their prior frequent episodic TTH (eight subjects) were assumed to have experienced remission.
Prognostic variables for poor outcome for groups 1 and 2 were clinical characteristics of migraine and TTH in 1989, respectively. The univariate and multivariate logistic regression models were used to evaluate the ability of independent variables, that is, prognostic variables, to predict dependent variable, poor outcome of migraine with/without TTH and pure TTH. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. In the multivariate model, ORs were adjusted for daily use of acute headache medications and use of prophylactic medications.
The association between prognostic variables and poor outcome was also analyzed using pooled data from both groups. In this analysis, poor outcome was defined as chronic headache or headache occurring ≥15 days/month at follow-up in 2001. Prognostic variables included headache characteristics, age, gender, daily use of abortive headache medications (paracetamol, aspirin and combination analgesics containing codeine), use of headache preventive medications and type of primary headache (pure migraine, pure TTH or coexistent headache).
Results
Population
In 2001, 673 of the 740 participants in the 1989 study were eligible. Of the 67 non-eligible subjects, 42 were deceased, 9 had emigrated, 6 were missing in the address list, and 10 were unable to answer verbal or written questions. In total, 549 subjects (81.6%) participated in the follow-up: 285 females and 264 males. The mean age of subjects was 55.5 years. Subjects aged 65 years or older were less likely to participate. As previously reported, when assessed by logistic regression, the participants were representative of the eligible study population with regard to gender and, for subjects younger than 65 years old in 2001, also with regard to age. In addition, the participants in the 2001 survey did not differ from non-participants with regard to headache status in 1989, and no difference in mortality according to headache status in 1989 was observed. The statistical analysis and results of these data are described in detail elsewhere (12).
Migraine with or without TTH: Cross-sectional data
Comparison of clinical characteristics of migraine in individuals with episodic (< 180 headache days/year) and chronic (≥180 headache days/year) headache (migraine + / − TTH) in 1989

TTH = tension-type headache.
Migraine with or without TTH: Longitudinal data
Distribution of clinical characteristics of migraine in individuals with migraine + / − TTH in 1989 according to good and poor outcome of headache in 2001
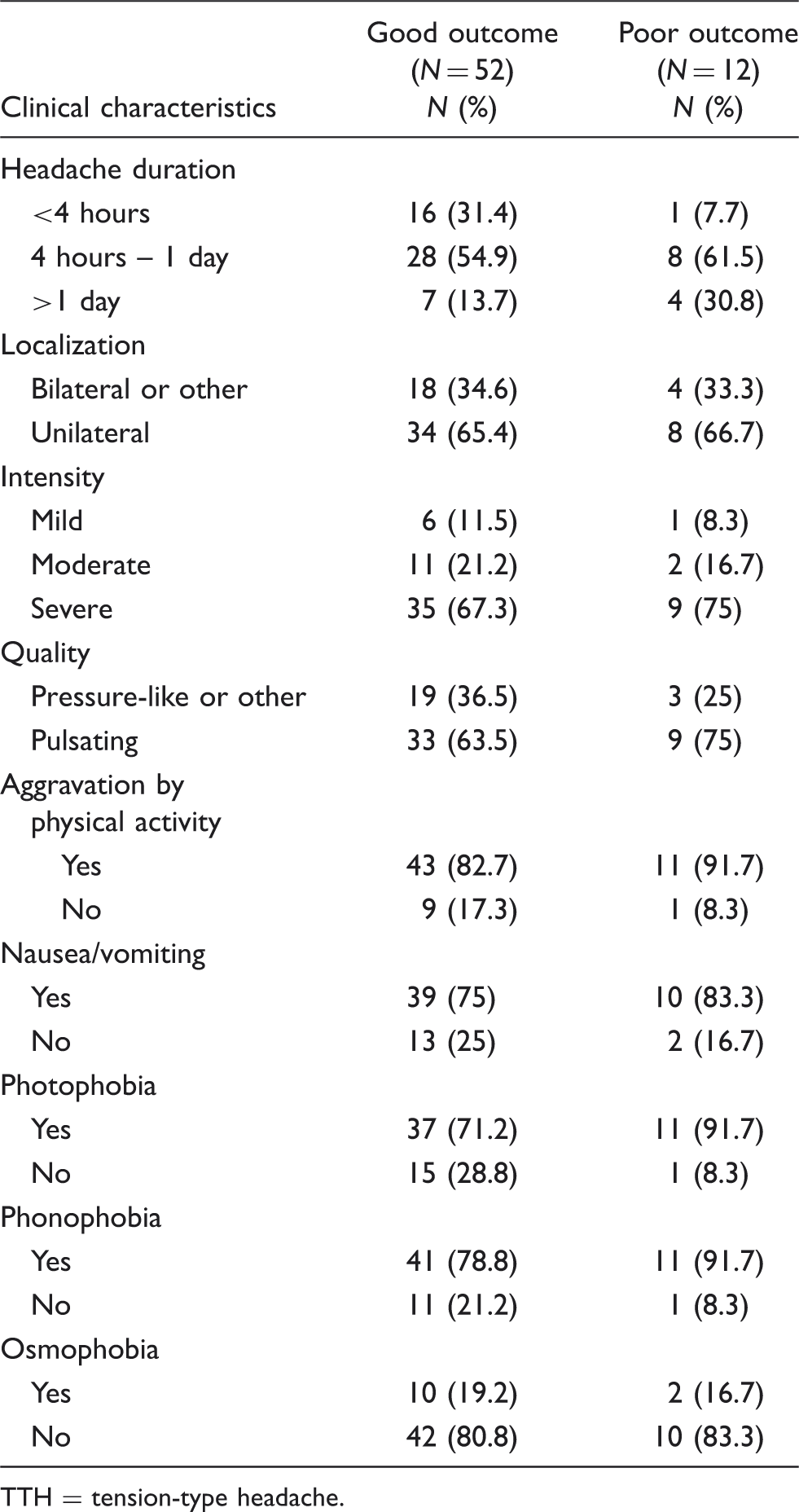
TTH = tension-type headache.
ORs for predictive factors (clinical characteristics of migraine, 1989) for poor outcome of migraine + / − TTH in 2001

CI = confidence interval. OR = odds ratio. TTH = tension-type headache.
Adjusted for use of acute headache medications and use of prophylactic medications.
Pure tension-type headache: Cross-sectional data
Comparison of clinical characteristics in individuals with pure frequent episodic (15–179 headache days/year) and chronic (≥180 headache days/year) TTH in 1989

CTTH = chronic tension-type headache. TTH = tension-type headache.
Indicating p < .05 level.
Pure tension-type headache: Longitudinal data
Distribution of clinical characteristics in individuals with TTH in 1989 according to good vs. poor outcome of pure TTH in 2001

TTH = tension-type headache.
ORs for predictive factors (clinical characteristics of TTH in 1989) for poor outcome of pure TTH in 2001

CI = confidence interval. OR = odds ratio. TTH = tension-type headache.
Adjusted for use of acute headache medications and use of prophylactic medications.
Pooled data
Univariate analysis of pooled data did not demonstrate any association between age, gender and poor outcome. Daily use of acute headache medications (OR = 6.78, 95% CI = 2.56–17.94, p ≤ .001), use of headache preventive medications (OR = 7.70, 95% CI = 1.45–40.77, p = .016) and coexistent headache (OR = 2.89, 95% CI = 1.19–7.04, p = .019) were significant predictors of poor outcome. In univariate analysis, only nausea was a significant predictor of poor outcome (OR = 2.48, 95% CI = 1.02–6.01, p = .045). After adjustment for daily use of acute headache medications, use of headache preventive medications and coexistent headache, only nausea, unilateral localization of headache and pulsating quality of headache tended to predict poor outcome, but associations did not reach statistical significance. When adjusted for use of headache preventive medications and coexistent headache, only paracetamol (OR = 7.34, 95% CI = 2.09–25.74, p = .002) was a significant predictor of poor outcome.
Discussion
In the present study we found that individuals with episodic and chronic headaches, which included migraine with and without TTH, did not differ in clinical characteristics of migraine. For pure TTH, the duration of headache episodes longer than 72 hours was more prevalent in the CTTH group at baseline, whereas headache in individuals with frequent episodic TTH at baseline was more frequently aggravated by physical activity. To our knowledge this is the first study to compare the clinical characteristics of episodic TTH and CTTH. Differences between clinical features of episodic migraine and transformed migraine or chronic daily headache have previously been studied in patients from tertiary headache centers (22,23). In contrast to our findings, Rothrock et al. (22) found that pulsating quality and unilateral localization of headache, photophobia, nausea and vomiting were more prevalent in the episodic group. In that study, patients with chronic headache were classified as having transformed migraine, defined by Mathew et al. (24), and presented with features of both migraine and TTH. In another study by Galego et al. (23) photophobia, phonophobia and vomiting were also found to be more prevalent in episodic migraine than in transformed migraine. However, this was not the case for nausea, which was reported to be more prevalent in transformed migraine. The conflicting results between our study and previous studies may be related to the different methodologies and definitions of headache cases used. Another major limitation of the previous studies was the lack of a population-based sample.
The role of clinical characteristics in the chronification of migraine and TTH has not been previously investigated in a longitudinal study. In our study, association of poor outcome or increased frequency of coexistent migraine and TTH with pulsating quality and severe intensity of migraine headache, photophobia, phonophobia and longer duration of an individual migraine attack was demonstrated. We also found that unilateral headache, nausea and individual headache attack duration of 72 hours or more were associated with poor outcome or chronification of pure TTH. However, these associations did not reach statistical significance. In the pooled data analysis we found that nausea was a statistically significant predictor of chronic headache. However, after adjustment for medication overuse, use of preventive medications and coexistent headache, only nausea, unilateral localization of headache and pulsating quality of headache tended to predict chronic headache but associations did not reach statistical significance. Our findings suggest that certain headache features and associated symptoms may be either directly or indirectly involved in the pathophysiology of transformation of migraine and TTH but alone may not predict the transformation or chronification. Identification of risk factors involved in chronification of primary headache such as migraine and TTH has been a subject of extensive research in the recent years. Only few prospective population-based studies have studied predictive factors for poor outcome of migraine and TTH. In a prospective population-based study, Lyngberg et al. (12) demonstrated that predictive factors for the poor outcome or increased frequency of migraine were age younger than 20 years at the onset of migraine, being younger than 20 years of age, and having high migraine frequency at baseline. In addition, sleeping problems, increasing age and frequent or CTTH tended to be associated with the poor outcome of migraine. For TTH, predictors of poor outcome were found to be baseline CTTH, active migraine, not being married and sleeping problems (12). Medication overuse, smoking, lack of physical activity and poor self-rated health were also associated with the chronification of TTH but did not reach statistical significance. In another important population-based study, Scher et al. (11) reported that obesity and high baseline headache frequency predicted new-onset chronic daily headache in subjects with ages between 18 and 65. In that study chronic daily headache was defined as ≥180 headaches/year, without separation between migraine and TTH, and likely inclusion of subjects with possible medication overuse. Other factors, which tended to predict the new-onset chronic headache in this study, were diagnosis of arthritis and diabetes, non-Caucasian race and being previously married. In adolescents, acute medication overuse and major depression were shown to be independent predictors of persistence of chronic daily headache in this age group in a two-year longitudinal study (25). In the elderly population, only medication overuse was shown to be predictor of persistent chronic daily headache (26). Following these studies, Bigal et al. (13) demonstrated that use of barbiturates and opiates in subjects with episodic migraine was associated with increased risk of developing transformed migraine at one-year follow-up. Interestingly, in our study we found that only paracetamol was a significant predictor of chronic headache in the adjusted model. Our finding of association between poor outcome and use of headache preventive medications is probably explained by the fact that people who have frequent and severe headaches are likely to use prevention.
In the present study, high-frequency migraine also tended to predict poor outcome of coexistent headache. In addition, coexistent headache was a significant predictor of chronic headache in the pooled data analysis. There is clinical evidence suggesting that chronification of migraine does not occur abruptly and that transformation rates may vary by individual. A transition staging model for migraine has recently been proposed based on epidemiological and experimental studies as well as on clinical observations (27). In this model, individuals with migraine can transition between three states: low-frequency episodic migraine (0–9 headache days/month), high-frequency episodic migraine (10–14 headache days/month) and CM. The rates of transition could be determined by various risk factors. The transformation from low-frequency episodic migraine to high-frequency episodic migraine may be risk factors for later transformation to CM.
Thus, the process of chronification of migraine and TTH is complex and possibly involves genetic, psychological, environmental and biological risk factors. Our study addresses only the biological or pathophysiological risk factors for the chronification. Pain perception studies have demonstrated that hyperexitability of nociceptive pathways—that is, central sensitization—may play a role in the chronification of both migraine and TTH (7,28–31). In a population-based study (31) Buchgreitz et al. were able to demonstrate that mechanical pain perception in individuals with poor outcome was normal at baseline in 1989 whereas both cephalic and extracephalic pain thresholds were decreased at follow-up in 2001, indicating that increased pain sensitivity may be a function, and not a cause of chronification of TTH. However, pathophysiological mechanisms leading to chronification of migraine and TTH may differ. The presence and severity of cutaneous allodynia, a marker of central sensitization of nociceptive pathways in migraine, has been shown to be associated with pain features and associated symptoms in patients with episodic migraine in a recent population-based study (32). The odds of having severe allodynia more than doubled in migraineurs with throbbing quality of headache, unilateral headache, headache aggravated by physical activity, photophobia, phonophobia or nausea (32). Another population-based study by Bigal et al. (28) found that cutaneous allodynia was more prevalent in transformed migraine (68.3%) compared to episodic migraine (63.2%). These interesting findings have raised the question of whether cutaneous allodynia may predict chronification of migraine. In a recent longitudinal population-based study (33) cutaneous allodynia was reported to be a risk factor for new-onset CM even after controlling for demographics, headache-related disability, comorbid depression and anxiety.
The pathophysiological mechanisms leading to certain headache features and associated symptoms in primary headaches are likely complex and are not fully clarified. Photophobia and phonophobia are symptoms of neuronal excitability to sensory stimuli. It is not clear how these symptoms and nausea may be related to development of central sensitization. Although nausea cannot be present in TTH per classification criteria, it can be associated with pain of severe intensity (14). Locus ceruleus, located in the brainstem, may play a role in development of photophobia and phonophobia in migraine (34). Dysfunction of the locus ceruleus, which is in the vicinity of trigeminal nucleus caudalis and has connections to the cerebral cortex, may lead to increased cortical excitability and greater sensitivity to sensory stimuli in migraineurs (34–37). The pulsating headache, which is associated with increased levels of calcitonin gene–related peptide, may activate and wind up sensory signals from perivascular nociceptors and lead to sensitization of nociceptive trigeminovascular pathways, and subsequently contribute to chronification (38–40). Further studies with a focus on the pathophysiological mechanisms involved in the development of headache features and associated symptoms in migraine and TTH are needed to support our findings.
Some methodological considerations need to be addressed. The major limitation of our study was the small sample size, reflected in large confidence intervals of odds ratios. In addition, intermediate depression and disability of individuals was not measured in the current study. Increased disability from headache and presence of depression during the interval between the interviews in 1989 and 2001 could have influenced the results of the study. The advantage of the present study was the use of longitudinal and prospective design without intervention in the follow-up period. Moreover, the detailed interviews were conducted by physicians who were blinded for the initial diagnosis of migraine or TTH.
In conclusion, chronification of primary headaches is complex and involves various risk factors. Combining these risk factors with certain clinical characteristics of migraine and TTH may predict increased frequency and therefore chronification of these primary headaches. Our findings suggest that physicians treating patients with episodic headaches should be aware of these risk factors. Identification of risk factors for increased frequency of headache may prompt initiation of early prophylactic intervention in patients with migraine and TTH. Future longitudinal studies using larger population samples are warranted.