
Abstract
The aim of this study was to document the frequency and types of aura symptoms, to define the relationship between aura symptoms and to define the aura frequency in different migraine types. In 952 migraine patients, aura frequency, duration, time to headache, characteristics and percentage of headaches with aura were analysed. Thirty-eight percent of IHS 1.1-1.5 patients reported aura, 38.1% of females and 33.0% of males. Average percentage of aura occurrence with headache was 19.7% of headaches, average aura duration 27.3 min and aura was followed by headache in 10.4 min on average. Visual disturbances occurred in 92.1% and aura without visual aura was rare. Aura frequency was headache-type dependent. The highest frequency of aura was seen in the more ‘full-blown’ migraine attack. Visual aura is the overwhelming aura symptom. Even in patients with aura the percentage of aura with migraine attacks is limited.
Introduction
Aura in migraine has sparked important concepts in migraine pathophysiology. Fifteen years after the description of cortical spreading depression (CSD) by Leao in 1944 (1), attention was drawn to the similarity of aura to this phenomenon (2). Many similarities between these two processes have been demonstrated (3, 4). CSD has been demonstrated in vivo in a head injured patient while aura has been successfully imaged during migraine (5–7). CSD has been speculated to be the mechanism of the aura with occipital cortical depolarization causing the positive phenomenon of visual aura and the resultant depression being responsible for the scotoma. Experimental evidence has shown the potential mechanisms and pathways for CSD to activate the acute migraine attack (8, 9). However, the number of migraineurs manifesting aura is limited and calls into question the broader issue of the initiating site(s) of the acute migraine attack in patients without aura.
Aura and aura symptom frequency vary widely in the literature (10–18). The aura features themselves have been well characterized. Common to many migraine features the frequency probably depends on many factors, few of which have been defined in the literature.
This study is an attempt, using a large detailed clinical database in tertiary headache care, to better characterize aura symptoms in frequency, duration and character, to explore aura symptom interaction, and to relate aura frequency to headache type.
Patients and methods
Study population
The study population consisted of men and women suffering from the full range of the International Headache Society defined migraine with or without aura (19). These patients were treated by the author in his clinical practice and the data were obtained during the author's usual daily practice.
Patients were excluded from the study if they had:
no headache;
headaches thought to be related to trauma or injuries;
complicated neurological problems, i.e. underlying brain or systemic illness related to their headaches;
recent onset headaches, i.e. less than one month prior to study;
significant legal issues related to their headaches;
been seen prior to the initiation of the database;
declined to, or were cognitively not able to participate in the data base interview;
language or intellectual barriers.
Study design
Eligible headache patients at the author's clinic seen consecutively between July 2000 and December 2002 were included in a database. Patients were subjected to a headache evaluation, based on their past month typical headache characteristics, as well as a physical and neurological examination. A thorough medical history of these patients was also recorded. Headache and aura characteristics were recorded. Approval from an institutional review board was not sought. The study was a review of a clinical database. The personal identities of patients were discarded when the data were downloaded to the statistical package.
Patient symptom rating
Patients recorded the usual percentage of headaches with aura and percentage of aura with no headache. Typical aura duration and aura duration before headache were recorded in minutes. Visual aura, speech aura, numbness or tingling aura, dizziness aura and blackout with aura were recorded on a 0–3 scale. 0 = never; 1 = occasional (1%–33%); 2 = frequent (34%–66%); 3 = very frequent (67%–100%). Headache severity was rated 0–10.
Statistical analysis
The data were presented in descriptive form using SSPS statistical package (version 11.0 for Mac). Means comparison was made with independent Samples T-test with P < 0.05 regarded as significant.
Headache classification
The study was performed before the publication of IHS 2nd Edition. However, the 2nd Edition was used for reporting the data. Headache patients in this study were divided into all migraineurs 1.1–1.6 (definite and probable; formerly 1.1–1.7), only definite migraineurs 1.1–1.5 (formerly 1.1–1.6), transformed migraine (development of chronic daily headache evolving from migraine), migraine headache with associated medication overuse, and headache every day. In addition patients were analysed
with migraine 1.1–1.5 less than 15 days per month, nausea grade 3/3, headache average intensity greater than 6/10 and headache with unilateral grade 3/3;
with migraine 1.1–1.5 less than 15 days per month and headache with unilateral grade greater than 0/3;
with migraine 1.1–1.5 less than 15 days per month with unilateral headache grade 3/3.
Results
Demographic characteristics
Of the 952 patients seen by the author at the initial visit, 84.9% were females and 15.1% were males. The mean (± SD) age of patients was 37.6 ± 11.75 years (range 13.0–80.5 years).
Aura frequencies
General.
Thiry-eight percent of IHS 1.1–1.5 reported aura, 38.1% of females and 33.0% of males (Not significant). 35.5% of IHS 1.1–1.6 patients reported aura, 36.8% of females and 27.5% of males (P < 0.05).
Headaches types and aura frequency.
See Table 1 for details.
Number of patients with aura by headache type – IHS 2nd Edition

Data collected prior to IHS 2nd Edition.
All definite migraine and including probable migraine.
All definite migraine and excluding probable migraine.
Average percentage of aura with headache.
In patients reporting aura, the average percentage of aura occurrence with headache was 19.7% of headaches (1–25% of aura with headache reported in 37%, 25–50% in 25%, 50–75% in 9%, 75–99% in 8%; 100% in 21%). Also 1–10% = 68.6%; 11–29% = 8.4%; 30–69% = 9.4% and 71–100% = 13.6%. (Fig. 1)

Number of headaches with aura in patients reporting aura.
Average duration of aura.
The average aura duration was 27.3 min (<15 in 35%; 15–30 in 28%; 30–45 in 5%; 45–60 in 14%; >60 in 18%).
Timing of aura.
Aura was followed by headache in 10.4 min on average(0 in 76.0%; <15 in 5.1%; 15–30 in 9.5%; 30–45 in 0.6%; 45–60 in 6.5%; >60 in 2.2%). The aura occurred before the headache in 67.4%, before and during in 5%, before or during in 0.3%, during in 18.7%, during and after in 0.3%, after in 0.3%, and during all phases in 8.0%.
Aura symptom frequency.
Visual aura was absent in 7.9%, occasional in 20.7%, frequent in 19.5%, and very frequent in 60.8%. Aura with numbness or tingling was absent in 56.8%, occasional in 22.3%, frequent in 9.7%, and very frequent in 11.2%. Aura with speech difficulties was absent in 69.8% of headaches, occasional in 15.5%, frequent in 10.1%, and very frequent in 4.7%. Aura with dizziness was absent in 38.2%, occasional in 32.1%, frequent in 20.4%, and very frequent in 9.3%. Blackouts were absent in 91.6%, occasional in 7.3%, frequent in 0.4%, and very frequent in 0.7%. Aura without headache was absent in 66.5%, present in 1–25% in 12.3%, 25–50% in 7.9, 50–75% in 4%, 75–100% in 6.2%, and 100% in 3.1% (Fig. 2).
Frequency of aura symptoms; ▪ absent, occasional,  frequent, □ very frequent.
frequent, □ very frequent.
Aura symptoms
See Tables 2, 3 and 4 for aura symptoms as asked directly and graded 0–3. Visual aura is distinctive
Direct questioning: aura symptoms

Aura symptoms: occurrence of non-visual aura symptoms in absence of visual aura expressed as a percentage of total occurrence

Aura symptoms: occurrence of isolated individual aura symptoms expressed as percentage of total occurrence

in frequency, overall being present in 92.1% of patients with aura and often being present as the only aura symptom;
in severity, with high percentage of grade 3;
in dominance, with nonvisual aura rarely present without visual aura.
See Table V for aura symptoms obtained by asking for ‘other symptoms experienced before the start of the migraine attack’. Some of these may represent symptoms of the migraine attack.
Aura – other symptoms reported by patients∗
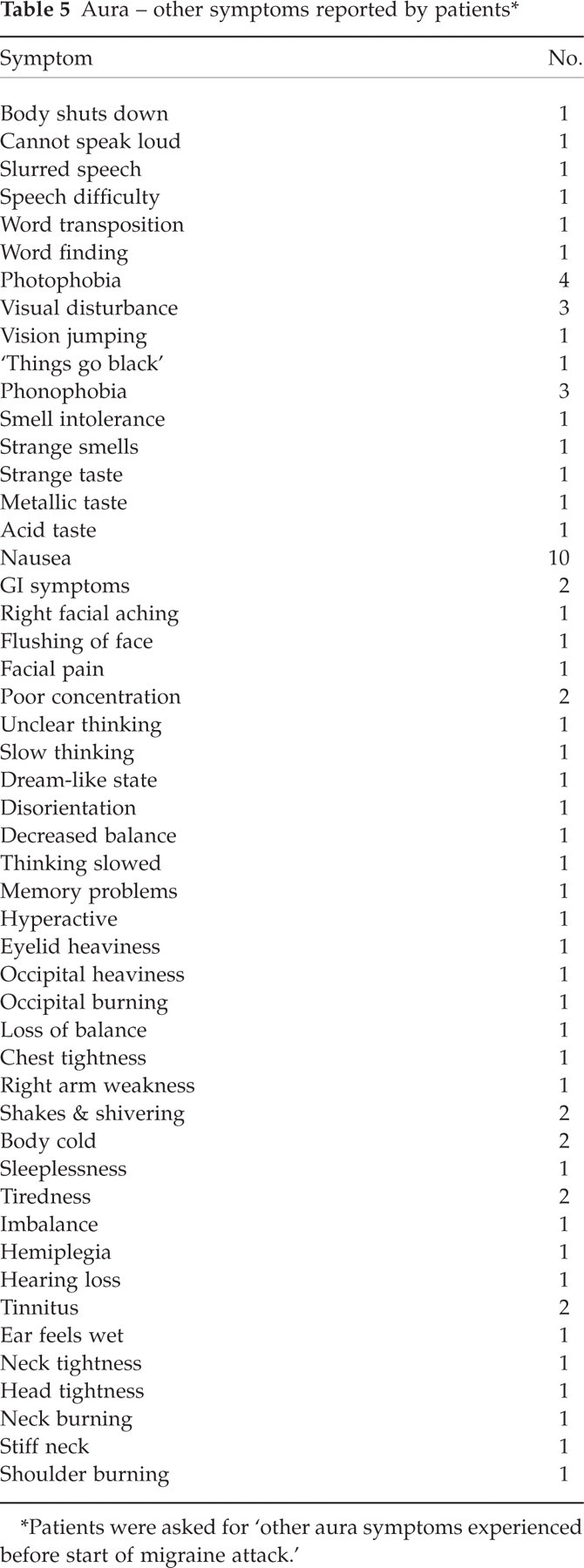
Patients were asked for ‘other aura symptoms experienced before start of migraine attack.’
Figure 3 shows the effect of increasing grade on the presence of other aura symptoms. Visual aura occupies a unique position, as increasing visual aura grade is associated with increasing grade of other symptoms. Figure 4 is an example of this not occurring with other aura symptoms. Increasing intensity of nonvisual aura symptoms does not increase the frequency of other aura symptoms.
The effects of visual aura severity on the prescence of non-visual aura; □ grade 1, ▪ grade 2, grade 3.
The effeects of numbness and tingling aura severity on the presence of non-numbness and tingling aura; □ grade 1, ▪ grade 2, grade 3.
Discussion
This study documents a 37.5% frequency of aura in migraine. This conforms with a frequency of 33% found in a headache clinic (13) and contrasts with 68% in a highly selected population (17). Large population studies document frequencies of 44.6% and 24.1% in physician and ‘no physician’ diagnosed migraine, respectively (20, 21). Females in the current study had a higher aura frequency than males, significant in probable migraine but not definite migraine. Population studies of definite migraine showed a significantly higher prevalence in females (12). Unilateral headache did not significantly affect aura frequency unlike a previous study (13). However, a recent prospective study did not show a unilateral preponderance of headache in migraine patients with aura (22). Migraine aura frequency in this study ranged from 25.3% in unremitting daily headache in the total migraine population to 37.5% in definite migraine and reached 50.8% in migraine with frequency less than 15 per month, nausea 3/3 rating, and headache average intensity rating greater than 6/10. These data show that the more full-blown the migraine attack is, the higher the aura frequency.
Aura occurred exclusively before headache in 67.4% of patients similar to the 57% reported in a tertiary care study (23). Headache followed aura on average in 10.4 min and immediately in 76% of patients compared to 61% in a prospective study (22). Headache occurred within 30 min of aura in 85% of patients similar to the 75% in another study (23). In the same study of 32 aura patients (12) nearly 20% had aura without headache, with 33.5% in the current study reporting aura without headache on occasion.
In patients reporting aura the average frequency was 19.7% of migraine attacks. This figure contrasts with higher frequencies (13) (1–10% = 30% of headaches; 11–29% = 14%; 30–69% = 16% and 71–100% = 40% compared with the current study of 68.6%, 8.4%, 9.4%, and 13.6%, respectively). The current study shows that 79% of patients with aura (35% of patients) had both migraine with aura and migraine without aura. This is also to be contrasted with population studies showing 4.3% and 1.2% of patients had both migraine with aura and migraine without aura (10, 18). These differences have been attributed to selection bias due to a selective population in tertiary care. Presented with a Yes/No choice only, the current study may have yielded very different results as most patients had aura with headache relatively infrequently and these patients may have said ‘No’ if not given the choice of ‘percentage of headache with aura’. The current study did not address changes in aura across age or longitudinally in time. Nor is this a diary-controlled study. Missing from this study is both population data and longitudinal data. The former, however, has little relevance to tertiary care of headaches.
The current study confirms previous observations of the dominance of visual aura (13, 16). Increasing visual aura rating by patients increases frequency of the other aura phenomenon. However, as is shown, this is not seen with other aura components. The occipital cortex clearly demonstrates dominance in aura. The cause for occipital dominance in migraine aura is not clear.
In practice one is impressed by the number of patients changing over time to include aura in their migraine manifestations, such as in perimenopausal situations and then reverting to less or no aura when these circumstances change back to baseline. Similar changes occur at times in patients’ migraine lifetime with regard to other features of migraine such as headache frequency, headache intensity, associated symptoms, and triggers due to changing circumstances. Aura is described in other primary headaches (24–26). Response to acute and prophylactic medication is the same in patients with aura and patients without aura (17). Furthermore, in this study even in the 35% of patients who report aura with headache, the average frequency of aura with headache was only 19.7% while 79% reported both migraine with aura and migraine without aura. Thus most patients with aura suffer from migraine without aura. This suggests that cortical activation may occur, randomly or under genetic influence, perhaps as in the activation of other brain structures like blood vessels, causing throbbing headache or pain with head movement, or activation of the ‘nausea centre’ causing nausea or vomiting. Perhaps the brainstem does indeed orchestrate the migraine attack (27). Therefore the author's bias is towards a dynamic process at times activating different components of headache including aura, rather than a unique ability of aura/CSD to initiate all migraine.
Conclusion
This study characterizes migraine aura in a tertiary outpatient headache practice. Differing aura frequency occurs in migraine types with the highest frequency seen in the more ‘full-blown’ migraine attack. Aura is more frequent in females. Visual aura is the overwhelming aura symptom. Even in patients with reported aura the overall percentage of aura with migraine attacks is limited, perhaps calling into question whether cortical activation is a necessary component of the migraine attack.