
Abstract
The purpose of this study was to evaluate whether a particular genotype of the dopamine D2 receptor (DRD2) gene would affect the clinical features of migraine. In a group of 118 migraineurs (55 migraine with aura and 63 migraine without aura patients), we tested the association of the biallelic C/T NcoI DRD2 polymorphism with several characteristics of the disease. Genotype and allele frequencies resulted similarly distributed in migraine with aura and migraine without aura patients (χ2 = 1.58, P = 0.45 and χ2 = 0.09, P = 0.77, respectively). The different DRD2 genotypes (C/C, C/T and T/T) had no significant effects on age at onset of migraine, presence of premonitory phenomena, frequency of headache attacks, associated symptoms, psychological features and quality of life of our migraine patients. The results of our study do not support a role for the DRD2 gene in modifying the clinical features of migraine.
Introduction
Several studies support a strong genetic basis for migraine but, at present, the type and the number of genes involved in the pathogenesis of the disease are still unclear (1, 2).
A growing body of data suggests that dopaminergic systems are involved in the pathogenesis of migraine. Various anti-dopaminergic drugs abort migraine attacks, while dopamine agonists may be useful for prophylaxis (3–5). Pharmacological studies with dopaminergic agents like apomorphine suggest that migraineurs present, even in the interictal phase of the disease, an hypersensitivity of the dopaminergic receptors (6, 7). Finally, patients with migraine show an increased density of dopamine receptors on lymphocytes (8). Hence, genes that code for enzymes and receptors modulating dopaminergic activity are good candidates for investigation of the molecular genetic basis of migraine.
The dopamine D2 receptor (DRD2) gene is one of the most extensively investigated gene in neuropsychiatric disorders. Several studies analysed the possible association between polymorphisms in the DRD2 gene and migraine. In 1997, Peroutka et al. reported that DRD2 NcoI alleles significantly modify the clinical susceptibility to migraine with aura (9). In addition, the same authors reported that the DRD2 NcoI C allele frequency was significantly higher in individuals with migraine with aura, anxiety or major depression than in individuals who had none of these disorders (10). However, Dichgans et al. and Lea et al. were unable to confirm the association between migraine with aura and DRD2 NcoI alleles (11, 12). Using the Transmission Disequilibrium Test, Del Zompo et al. found no association between the dinucleotide repeat alleles within intron 2 of the DRD2 gene and migraine without aura. However, in a subgroup of patients, selected for the presence of both nausea and yawning immediately before or during the pain phase of migraine (so called ‘dopaminergic migraineurs’), the allele 1 appeared to be in disequilibrium with the disease (13). Finally, no association was found between the −141C Ins/Del polymorphism of the DRD2 gene and migraine (14). So, the precise role of DRD2 gene in migraine is, at present, unclear.
To further investigate this issue, we compared the clinical and psychological characteristics of a large group of migraine patients, recruited from a Headache Clinic, with DRD2 NcoI genotypes. The objective of our study was to evaluate whether a particular allele or genotype of the DRD2 gene would affect the clinical features of migraine.
Methods
Subjects
One hundred and eighteen patients with migraine (104 female, 14 male; mean age ±
Assays
Genomic DNA was extracted from whole blood samples using the QIAamp® DNA Mini Kit (Qiagen, Valencia, CA, USA). Primers 5′-TTGTCCGGCTTT ACCCA-3′ and 5′-ATCCTGCAGCCATGG-3′ were used to amplify a DNA fragment of 453 bp. We used 40 ng of genomic DNA in 50-µl reaction volume with concentrations of 0.4 mol/µl each of primers, 0.2 m
Statistics
Statistical analyses were performed using SigmaStat, version 1.0 (Jandel Corp., 1994, San Rafael, CA, USA). χ2 test and Fisher exact test were used to compare allele (AF) and genotype frequency (GF) between migraine with aura and migraine without aura patients. Differences in clinical features were compared using
Results
Demographic and clinical data regarding the migraine patients included in this study are shown in Table 1. The frequency of headache attacks was significantly (P < 0.01) lower in migraine with aura patients than in migraine without aura patients. No significant difference in the remaining clinical features examined was found.
Demographic and clinical characteristics of migraine patients

P = 0.002 in comparison with migraine with aura patients.
Table 2 shows both genotype and allele frequencies of the DRD2 gene in patients with migraine and in the subgroups. The genotype distributions were in Hardy–Weinberg equilibrium for both migraine with aura and migraine without aura groups. The overall frequencies of the DRD2 NcoI alleles in our dataset (236 chromosomes) were 0.66 for allele C and 0.34 for allele T. These values are similar to what has been reported in other European populations (20). No significant difference both in genotype (χ2 = 1.58, P = 0.45) and allele (χ2 = 0.09, P = 0.77) frequencies between migraine with aura and without aura patients was found.
Genotype (GF) and allele (AF) frequencies of the DRD2 gene polymorphisms in migraine patients

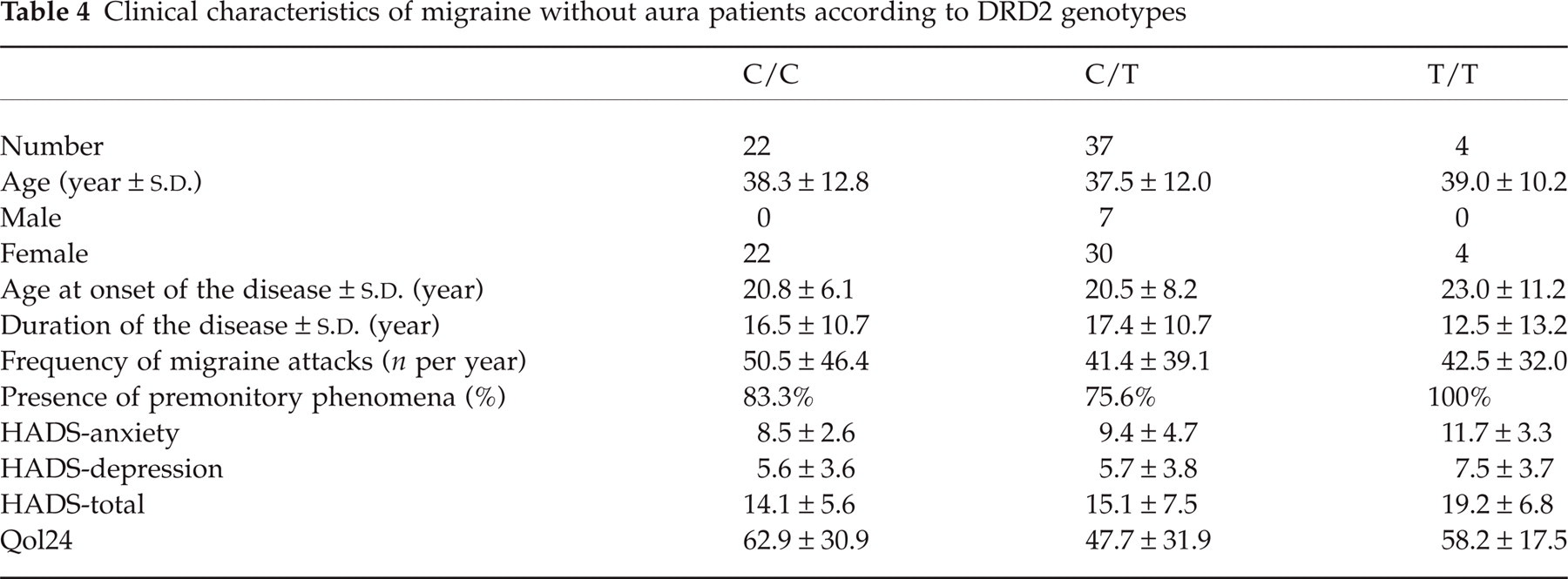
Tables 3 and 4 show the clinical features of the disease according to DRD2 genotypes (C/C, C/T and T/T) in migraine with aura and migraine without aura patients. The comparison of all the clinical and psychological features showed no significant difference.
Clinical characteristics of migraine with aura patients according to DRD2 genotypes

Clinical characteristics of migraine without aura patients according to DRD2 genotypes
Discussion
The human DRD2 gene is located on chromosome 11q22–23 and consists of eight exons separated by seven introns (20). By a mechanism of alternative splicing, the gene encodes two molecularly distinct isoforms, D2S and D2L, that have distinct functions in vivo (21). Shortly after the DRD2 gene was cloned, several polymorphisms were discovered. These polymorphisms have been associated with a large number of neuropsychiatric disorders, like alcohol abuse, cocaine abuse, schizophrenia, bipolar disorder, Parkinson's disease, tardive dyskinesia, etc. (22, 23). However, no conclusive linkage or association was found. So, at present, there is no clear-cut case in which polymorphisms in the dopamine D2 receptor gene are clearly related to a neuropsychiatric disorder, or even to a specific phenotype (23).
The results of our study do not support a significant role for the DRD2 gene in modifying the phenotypic characteristics of migraine. Migraine patients with different DRD2 genotypes showed similar clinical and psychological features. Genotype and allele frequencies resulted similarly distributed in migraine with aura and migraine without aura patients. Finally, different genotypes had no significant effect on the quality of life of our patients.
The findings of our study are not in accord with the results of previous studies showing that genetic markers within the DRD2 gene may modify the clinical features of migraine. Different factors may explain these discrepancies. First of all, the study strategies are quite different. Peroutka et al. (10) examined a group of unselected subjects and found that DRD2 NcoI C/C genotype was associated with a distinct clinical syndrome characterized by migraine with aura, depression and anxiety. Del Zompo et al. (13) studied an isolated genetic populations (Sardinia) and found a disequilibrium in the DRD2 genotypes only in a subgroup of patients presenting nausea and vomiting during the prodromic phase of the migraine attack. Therefore, it is possible that DRD2 alleles may modify the clinical features of the disease only in a subgroup of migraineurs. However, the DRD2 NcoI polymorphism involves a silent change at amino acid His313 and the expression of different alleles results in identical receptor molecules. So it seems unlikely that a non-functional variant of a gene may modifies the clinical features of a disease.
Footnotes
Acknowledgements
This research was supported by a 2000 grant from M.U.R.S.T., Italy.