
Abstract
Genetic epidemiological twin studies have demonstrated a significant heritability for migraine, with >60% of liability to migraine either with or without aura coming from additive genetic factors. Because of the essential role of serotonin in the pathophysiology and treatment of migraine, genes of the serotonin system are candidates for involvement in migraine. Consequently, we examined two functional VNTR polymorphisms in the serotonin transporter gene, the 5-HTTLPR and the intron 2 VNTR, in a sample of 212 family trios each with a proband with childhood migraine, 153 with migraine without aura (MoA) and 59 with migraine with aura (MA). For the first time, we used transmission disequilibrium test analysis with the program TDTPHASE to examine the transmission of these two markers and their haplotypes to offspring affected by migraine. We found no significant transmission distortion of any marker, with the common L allele of the 5-HTTLPR transmitted 170 times and not transmitted 178 times, and the S allele 130 vs. 122 times. Likewise, the common 12 allele of the intron 2 VNTR was transmitted 201 times and not transmitted 188 times, and the 10 allele 107 vs. 120 times. The markers were not associated with MoA and MA and none of the haplotypes was associated with overall migraine, MoA or MA. The 5-HTTLPR and the intron 2 VNTRs do not play a major role in susceptibility to migraine.
Keywords
Introduction
Genetic epidemiological twin studies have demonstrated a significant heritability for migraine (1, 2), with 61% of liability coming from additive genetic factors and 39% from non-shared environmental factors in migraine without aura (MoA) (3, 4) and 65% additive genetic effects in migraine with aura (MA) (5). In these two subtypes of migraine a complex genetic pattern of inheritance has been suggested (6) involving several susceptibility genes, most consistent with a polygenic multifactorial model involving both genetic and environmental factors (7–9).
Serotonin (5-HT), a neurotransmitter in the central nervous system, is involved in the regulation of a variety of behavioural and visceral functions, including mood, anxiety, aggression, gastrointestinal motility and vascular resistance. Serotonergic activity appears to be involved in many physiological functions (sleep, appetite, pain, etc.) as well as in pathological conditions such as anxiety, depression and schizophrenia (10, 11). 5-HT plays an important role in migraine pathophysiology (12–15). Evidence has been found for lower plasma levels of 5-HT between migraine attacks and contemporary treatment is most effective using triptans which are highly selective agonists of 5HT1B and 5HT1D receptors (16, 17). The comorbidity of migraine and psychiatric disorders such as depression and anxiety (18) may be explained by a common dysfunction in the serotoninergic system.
Thus, the 5-HT transporter (5-HTT) gene is regarded as a good candidate for migraine. The most commonly studied susceptibility loci of the 5-HTT gene are two variable numbers of tandem repeats (VNTR): (i) a 44-base pair insertion/deletion within the promoter region, termed the 5-HTT gene-linked polymorphic region (5-HTTLPR), with two allelic forms, the long variant (L) and the short variant (S), and (ii) a VNTR in the second intron (intron 2 VNTR) with three alleles (Stin2.9, Stin2.10 and Stin2.12). Both of these VNTRs are functional, with the S allele of the 5-HTTLPR having lower transcriptional activity (10, 19, 20) and the intron 2 VNTR having differential enhancer activity (21).
So far, 12 studies on 5-HTT polymorphisms in migraine are available (Table 1). All but one linkage study (22) used a case–control design and the total number of patients included ranged between 52 and 296, with a mean (± SD) of 130 ± 70 (MoA 29–173, 94 ± 47; MA 10–96, 52 ± 36). Nine of the studies analysed MoA and MA separately, the others did not. The 5-HTTLPR was examined in eight studies and the intron 2 VNTR in six. Three studies analysed both functional 5-HTT VNTR polymorphisms and four examined in addition the association between genetic markers and clinical data (23–26).
Studies on 5-HTT polymorphisms in migraine


M, Migraine; MoA, migraine without aura; MA, migraine with aura; MVA, migraine with severe vomiting and abdominal pain; Co, controls; Co2, unaffected relatives as second control group; 5-httpLR, 5-HT transporter gene linked polymorphic region; VNTR, variable numbers of tandem repeat; S, short allele of the 5-httpLR; s/s, genotype; 10, Stin2.10 allele; 12, Stin2.12 allele of the intron 2 VNTR; 10/12, 12/12, genotypes.
Findings as reported by the authors, no correction for multiple testing in any study; χ2 test results (P-values not reported).
The 5-HTTLPR S allele and the s/s genotype, respectively, were associated with migraine in three of the eight studies (Table 1) (24, 27, 28). Two of these studies (24, 27) found a specific association with MA. Correlating genetic and clinical findings revealed negative results, with a single exception, i.e. a higher migraine frequency in s/s carriers (Table 1) (25). In addition, there was no association between platelet 5-HT concentration and 5-HTTLPR variants in one study (29). Regarding the intron 2 VNTR, four studies (26, 30–32) have revealed a few, but conflicting, statistically significant results (Table 1) and two (33, 34) have shown no significant difference from controls.
In summary, the studies available provide only modest evidence for a role of the two most common 5-HTT polymorphisms in overall migraine, MoA or MA. None of the studies used correction for multiple testing, none analysed the haplotypes and none used family-based methods, such as the transmission disequilibrium test (TDT).
The TDT approach has two major advantages over case–control studies: (1) the absence of population stratification bias, and (ii) the possibility of showing linkage in the presence of association. Consequently, in the present study, for the first time, we aimed to investigate the familial transmission of both functional 5-HTT VNTR polymorphisms, the 5-HTTLPR and the intron 2, in a large sample of young patients of both gender with MoA and MA.
Subjects and methods
Subjects
We included 212 family trios, each with a patient with childhood migraine. Forty-eight percent were boys and 52% girls. Ages ranged from 6 to 19 years, with a mean of 10.8 ± 2.8 years. All patients had a clinical interview and a physical and neurological examination (35). The diagnoses were established by one experienced child neurologist based on the criteria of the second edition of the International Classification of Headache Disorders (ICHD-II) (36). The frequency of headache was scored on a scale of 1–5, where 1 was headache at least daily, 2 at least weekly, 3 at least monthly, 4 at least once per year and 5 less than once per year.
The project was approved by the Ethics Committee of the Medical University of Vienna. We obtained written informed consent from all participants and parents and data were kept anonymous to ensure subject confidentiality.
DNA and genotyping
DNA was prepared using established methods from buccal swabs, as described (37, 38). The samples were taken by the subjects themselves and were either immediately left at the clinic or sent to our centre by mail. Samples were coded and anonymized before DNA extraction and storage at the Social, Genetic and Developmental Centre (SGDP) molecular genetic laboratory of the Institute of Psychiatry. All markers were VNTRs and genotyping was performed by polymerase chain reaction followed by agarose gel electrophoresis and staining with ethidium bromide according to established procedures (19, 20).
Statistical analysis
Linkage disequilibrium (LD) between the single nucleotide polymorphisms was estimated using the LDMAX program (39). The statistical association R 2 was used to measure LD between markers (40). The program suite UNPHASED was used to test the LD between the individual marker locus or haplotypes and the hypothetical disease locus (41). UNPHASED can be used for association analysis of multilocus haplotypes from unphased genotype data. Statistical analysis of family trios was performed using the TDTPHASE from UNPHASED. TDTPHASE performs TDT analysis and haplotype-based haplotype relative risk calculations (HHRR) for nuclear families using the TDT; it is robust to families where genotypes are not available from both parents. Analysis was performed both for single marker and their haplotypes. We also analysed frequency of headaches, using non-parametric regression analysis in Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA; release 13, September 2004) using Spearman's correlation coefficient in the cases only.
Power analysis
For 200 family trios with migraine analysed by the TDT (total sample), assuming prevalence of migraine to be 14% in the general population (42), and using the 5-HTTLPR S allele as a nominal risk allele (allele frequency 0.42), the sample has a non-centrality parameter (NCP) of 5.52 and 65% power at α 0.05 to detect a strong genetic risk factor (recessive relative risk 4; homozygote relative risk 2). For a more modest risk factor (recessive relative risk 2; present in 30% of the population) the sample has 37% power and an NCP of 2.64. Power was calculated using the genetic power calculator (http://statgen.iop.kcl.ac.uk/gpc/index.html). A 5% level was accepted as significant.
Results
All patients met ICHD-II criteria for MoA (n = 153) or MA (n = 59). Both markers were in Hardy–Weinberg equilibrium (5-HTTLPR χ2 = 1.84, d.f. = 2, NS; intron 2 VNTR χ2 = 2.09, d.f. = 2, NS) based on analysis of the unrelated parents of the probands. Linkage disequilibrium between the two markers was moderate, with Lewontin's D′ 0.37 and R 2 0.25, as calculated by LDMAX using unrelated parental data. Genotype frequencies in the unrelated parents were very similar to other European populations with the L allele of the 5-HTTLPR having an allele frequency of 0.56 (compared with previous reports of 0.54 in German and UK populations) and the 12 allele of the intron 2 VNTR a frequency of 0.61 (compared with 0.58–0.60 in previous studies of the German population; see (43) for summary of allele frequencies).
TDT analysis was performed both for the two single markers and their haplotypes. The results of the TDT analysis are shown in Table 2. Neither the long nor short allele of the 5-HTTLPR showed any evidence of transmission distortion. Likewise, for the intron 2 VNTR, alleles 9, 10 and 12 showed no significant evidence of global or individual transmission distortion. When we examined haplotypes of the two markers we saw no significant association with either polymorphism in overall migraine, MoA or MA (Table 3). The results of analysis for headache frequency (data not shown) were also negative. We used 137 cases with both genotype and data on frequency. For the 5-HTTLPR Spearman's correlation coefficient was 0.06, P = 0.46 (two-tailed), for the intron 2 VNTR Spearman's correlation coefficient was 0, P = 1 (two-tailed).
Results of the transmission disequilibrium test analysis of single markers for all patients with migraine and separately for patients with MoA and MA
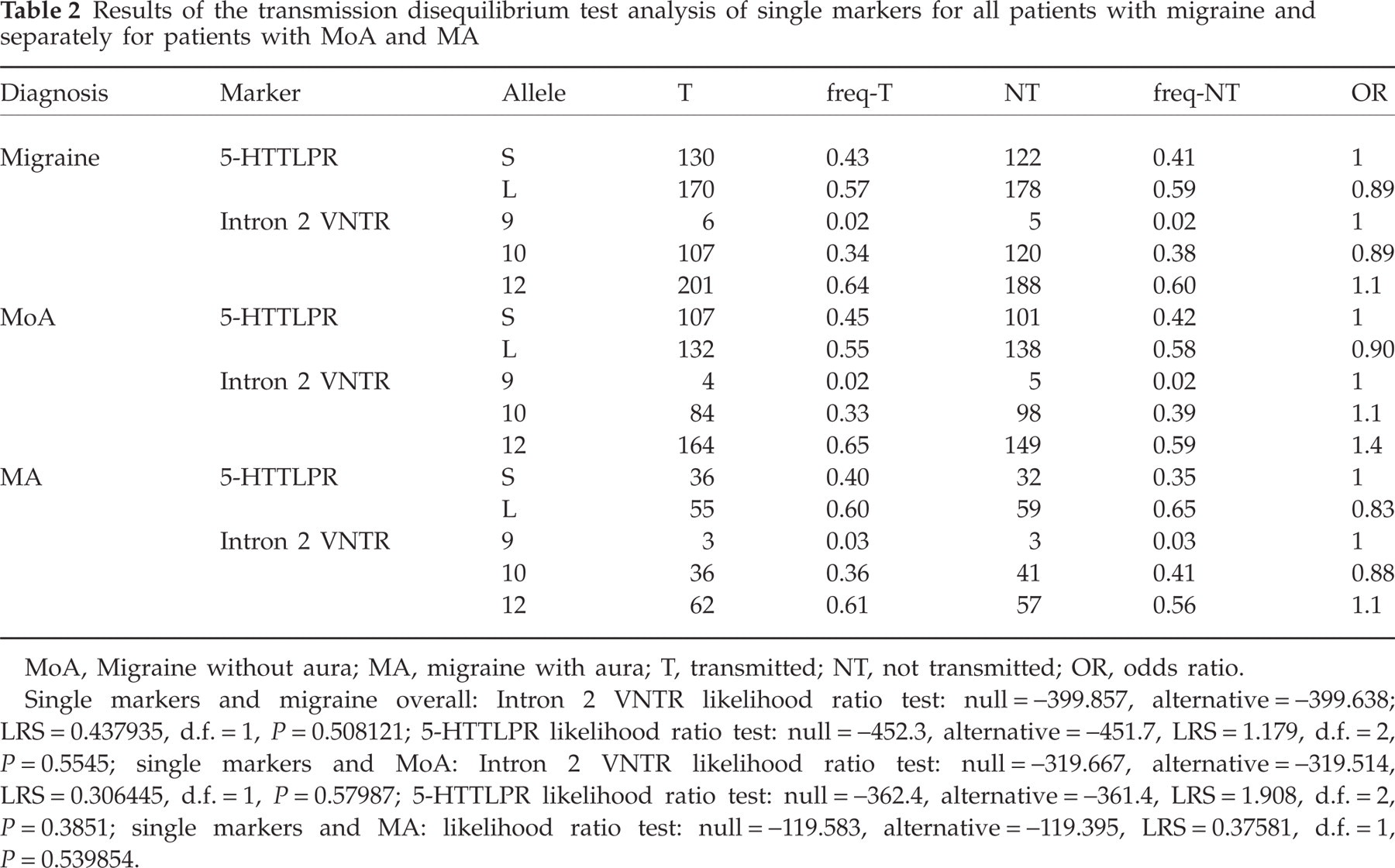
MoA, Migraine without aura; MA, migraine with aura; T, transmitted; NT, not transmitted; OR, odds ratio.
Single markers and migraine overall: Intron 2 VNTR likelihood ratio test: null = −399.857, alternative = −399.638; LRS = 0.437935, d.f. = 1, P = 0.508121; 5-HTTLPR likelihood ratio test: null = −452.3, alternative = −451.7, LRS = 1.179, d.f. = 2, P = 0.5545; single markers and MoA: Intron 2 VNTR likelihood ratio test: null = −319.667, alternative = −319.514, LRS = 0.306445, d.f. = 1, P = 0.57987; 5-HTTLPR likelihood ratio test: null = −362.4, alternative = −361.4, LRS = 1.908, d.f. = 2, P = 0.3851; single markers and MA: likelihood ratio test: null = −119.583, alternative = −119.395, LRS = 0.37581, d.f. = 1, P = 0.539854.
Results of the transmission disequilibrium test analysis of the haplotypes for all patients with migraine and separately for patients with MoA and MA

MoA, Migraine without aura; MA, migraine with aura; T, transmitted; NT, not transmitted.
Migraine overall: likelihood ratio test: null = −718.496, alternative = −717.304, LRS = 2.38375, d.f. = 5, P = 0.793891; MoA: likelihood ratio test: null = −578.066, alternative = −575.321, LRS = 5.49009, d.f. = 5, P = 0.359033; MA: likelihood ratio test: null = −229.127, alternative = −227.789, LRS = 2.67573, d.f. = 4, P = 0.613467.
Discussion
We analysed two functional VNTR polymorphisms in the 5-HT transporter gene, the 5-HTTLPR and the intron 2 VNTR, in a sample of 212 family trios each with a proband with childhood migraine, 153 with MoA and 59 with MA according to ICHD-II. Using the family-based association method TDT, we found neither a significant transmission distortion of the two markers or their haplotypes in overall migraine, MoA or MA, nor an association with the frequency of migraine attacks. Accordingly, our findings do not support previous positive case–control studies suggesting an association with the 5-HTTLPR S allele or s/s genotype (25–28) or an association with the intron 2 VNTR (26, 29, 31, 32).
Review of the previous studies in detail reveals several contradictory findings regarding the 5-HTTLPR S allele and the s/s genotype as well as the intron 2 VNTR 10/12 and 12/12 genotypes (Table 1). In one study, the S allele was detected more often in MA (n = 96) than in controls (n = 115) and MoA patients (n = 101) (27), whereas in another study (n = 126, 92% MoA, 8% MA) a borderline association (P = 0.049; odds ratio 1.45, 95% confidence interval 1.00, 2.12) between the S allele and the pooled data of MoA and MA was found (27). The s/s genotype was associated with MA in two European studies (24, 27) showing that 33% of the MA patients, but only 15–19% of the MoA patients and controls were s/s carriers. In contrast to these findings, three studies from eastern Asia (23, 25, 32) revealed that 60% of the healthy controls were s/s carriers. Ogilvie et al. (30) have reported that the 10 allele of the intron 2 VNTR is less common in patients with MoA and coexisting MoA and MA compared with controls, but this finding was not replicated (26, 31–33). The 12/12 genotype was most common in (i) MoA according to Ogilvie et al. (30) and Park et al. (32), (ii) MA and migraine associated with severe vomiting and abdominal pain according to Szilagyi et al. (26), and (iii) healthy controls according to Yilmaz et al. (31).
In conclusion, the inconsistent evidence from case–control studies suggesting a possible role of the two most common 5-HTT polymorphisms in overall migraine, MoA or MA, is not supported by our family-based study using TDT analysis. The 5-HTTLPR and the intron 2 VNTRs do not play a major role in susceptibility to migraine. For power reasons, a study with a much larger sample would be needed to investigate a putatively small effect of the 5HTT polymorphisms, in particular when looking at migraine subtypes. Genes from a variety of other systems, such as the dopamine and noradrenaline transporters and receptors (44), should also be considered as candidates for migraine pathophysiology.
Competing interests
None declared.
Acknowledgements
Supported by the Jubiläumsfonds of the Austrian National Bank given to Ç.W-B. (grant no. 10645).