
Abstract
The aim of the present study was to report on the utility of continuous Pcsf monitoring in establishing the diagnosis of idiopathic intracranial hypertension without papilledema (IIHWOP) in chronic daily headache (CDH) patients. We report a series of patients (n = 10) with refractory headaches and suspected IIHWOP referred to us for continuous Pcsf monitoring between 1991 and 2000. Pcsf was measured via a lumbar catheter and analysed for mean, peak, highest pulse amplitude and abnormal waveforms. A 1-2 day trial of continuous controlled CSF drainage (10 cc/h) followed Pcsf monitoring. Response to CSF drainage was defined as improvement in headache symptoms. Patients with abnormal waveforms underwent a ventriculoperitoneal (VPS) or lumboperitoneal (LPS) shunt insertion. All patients had normal resting Pcsf (8 ± 1 mmHg) defined as ICP < 15 mmHg. During sleep, all patients had B-waves and 90% had plateau waves or near plateau waves. All patients underwent either a VPS or LPS procedure. All reported improvement of their headache after surgery. Demonstration of pathological Pcsf patterns by continuous Pcsf monitoring was essential in confirming the diagnosis of IIHWOP, and provided objective evidence to support the decision for shunt surgery. Increased Pcsf was seen mostly during sleep and was intermittent, suggesting that Pcsf elevation may be missed by a single spot-check LP measurement. The similarity between IIHWOP and CDH suggests that continuous Pcsf monitoring in CDH patients may have an important diagnostic role that should be further investigated.
Keywords
Introduction
Chronic daily headache (CDH) affects 4–5% of the population (1, 2) and encompasses a number of different diagnoses, including chronic (transformed) migraine (CM), chronic tension-type headache (CTTH), new daily persistent headache (NDPH), and hemicrania continua. Although there is no current International Headache Society classification for CDH, one proposed definition is based on the persistent experience of head pain for at least 4 h in duration for more than 15 days/month (3).
In the last few years, several studies have shown that a number of CDH patients actually have idiopathic intracranial hypertension without papilledema (IIHWOP) when investigated with a lumbar puncture (4–7). Ramadan reported transformation of episodic migraine into CDH in a patient who developed IIHWOP (4). Marcelis and Silberstein (5) described 10 patients with IIHWOP who presented with CDH. Mathew et al. (6) found 12/85 patients with IIHWOP in a study of patients with refractory transformed migraine. Silberstein and Corbett emphasize the importance of performing lumbar puncture in patients with intractable CDH to rule out IIHWOP (8).
The clinical presentation of IIHWOP consists of refractory headache in the setting of elevated CSF pressure (Pcsf) and the absence of papilledema, making it difficult to differentiate clinically IIHWOP from CDH syndromes. In the absence of papilledema, the significance of Pcsf measured via lumbar puncture (LP) is uncertain, especially when the presence or absence of elevated Pcsf is the rationale for deciding whether to recommend shunt surgery as therapy. The practice of diagnosing or excluding IIHWOP by measuring Pcsf momentarily at the time of LP (essentially, a spot-check) presumes that the momentary Pcsf predicts the 24-h Pcsf profile. False-negative and false-positive LP results have been reported for pseudotumour cerebri (9), and variability of Pcsf has been described in other CSF circulation disorders, such as normal pressure hydrocephalus (NPH), where continuous Pcsf monitoring demonstrates that Pcsf elevation and instability is present mostly during sleep (10).
Continuous Pcsf monitoring may overcome the limitations of momentary Pcsf measurement via LP in diagnosing IIHWOP, but its role is not fully established (11). We report on the utility of continuous Pcsf monitoring in establishing the diagnosis of IIHWOP in a series of 10 patients initially diagnosed with CDH.
Methods
This is a case series of CDH patients (n = 10) in whom IIHWOP was suspected, based on elevated LP CSF pressure. CDH were defined as headaches lasting for at least 4 h in duration for more than 15 days/month (3). All patients were referred to our clinic between 1991 and 2000 for continuous Pcsf monitoring and CSF drainage trial. They all underwent complete general and neurologic examinations, and were seen by a neuro-ophthalmologist to confirm the absence of papilledema. All patients had an MRI scan of the head to rule out possible intracranial pathology. We recorded age, sex, weight, ophthalmoscopic findings, visual fields, evidence of head trauma and presence of sleep apnea. Lumbar puncture opening pressure (OP) was defined as abnormal for values greater than 250 mm H2O (12). Body mass index (BMI) was calculated. Body habitus was described according to the Center for Disease Control (CDC) and World Health Organization (WHO) definitions (13, 14): (i) 20 < BMI < 25: normal; (ii) BMI > 25: overweight; (iii) BMI > 30: obese.
Pcsf monitoring and controlled CSF drainage were accomplished via a lumbar catheter (Codman, Johnson and Johnson, USA). The catheter was inserted percutaneously into the lumbar subarachnoid space using a 14-Ga Touhy needle under local anaesthesia at the bedside. Pcsf and other variables (O2 saturation, pulse rate, respiratory excursion) were recorded continuously for 1–2 days on a Macintosh computer using a commercially available analogue-to-digital signal converter and software (MacLab, AD Instruments, Inc., Milford, MA, USA). An external strain gauge transducer was levelled to the external acoustic meatus. Pcsf was analysed for mean, peak, highest pulse amplitude, and abnormal waveforms.
Abnormal Pcsf waveforms were identified according to criteria adapted from Lundberg's original description (15). A-waves or plateau waves were defined as sustained elevation of Pcsf > 50 mmHg (680 mm H2O) for 5–20 min. Near plateau waves are similar in morphology and duration to plateau waves with the exception that Pcsf does not reach 50 mmHg. B-waves are rhythmic or semi-rhythmic waves occurring at a faster rate of 0.5–2 cycles per min with Pcsf elevations from 5 mmHg to 50 mmHg. Although Pcsf was recorded continuously, parts of the recording were unsuitable for Pcsf analysis because of movement artifact. Therefore Pcsf was analysed only during artifact-free epochs, when the record indicated the transducer was properly levelled and the patient was quiet. In most circumstances, this resulted in Pcsf analysis only during sleep or quiet rest.
A 1–2 day trial of controlled continuous CSF drainage followed Pcsf monitoring to assess patients’ response to shunt-like conditions. The CSF drainage rate was controlled to approximately 10 cc/ h (240 cc/day). Patients were clinically examined for their response at least once daily. Response to drainage was defined as subjective improvement in headache symptoms. Patients who had an abnormal Pcsf waveforms and those who responded to CSF drainage trial (n = 8) were referred for ventriculoperitoneal (VPS) or lumboperitoneal (LPS) shunt insertion. Two patients did not have a CSF drainage trial and were referred for shunt surgery based solely on Pcsf monitoring results.
Results
Patient characteristics and their presenting symptoms are described in Table 1. Mean age was 36 ± 3 years (mean ±
Patients’ demographics and headache characteristics

CM, chronic migraine; NDPH, new daily persistent headache; CTTH, chronic tension-type headache; BMI, body mass index; CDH, chronic daily headache; Sx, symptoms.
As per examining physician.
Some patients had other illnesses. Patients 1 and 10 had history of a Chiari malformation, which had been surgically decompressed prior to our evaluation. Patients 2 and 4 had been diagnosed with depression. Patient 5 had multiple sclerosis. Patient 8 had end-stage kidney disease treated with renal transplantation.
All patients were examined by a neuro-ophthalmologist. The ophthalmological exams are summarized in Table 2. One patient (♯2) had a small left visual field defect. Spontaneous retinal venous pulsation was present in 50% of cases. Results of MRI scans and LP are also shown in Table 2. All MRI scans were normal with the exception of patients 1, 4, 5 and 10. Mean lumbar puncture opening pressure (LOP) performed on nine patients prior to referral was 300 ± 26 mm H2O (22 ± 2 mmHg). Five patients (50%) had an LOP > 250 mm H2O (18 mmHg). The range of LOP was 210–398 mm H2O (15–29 mmHg).
Summary of neurological evaluation

Nl, normal; LVFD, left visual field defect; SV, slit ventricles; MS, multiple sclerosis; SH, subcortical hyperintensities; OB, oligoclonal bands.
Opening pressure for patient 1 was not found upon chart review. Elevated opening pressures are highlighted in bold.
Continuous Pcsf monitoring was performed for 2.1 ± 0.2 days, and the results are shown in Table 3. Resting Pcsf was 8 ± 1 mmHg (109 ± 14 mm H2O). All patients had normal awake resting Pcsf defined as Pcsf < 15 mmHg (204 mm H2O). Due to frequent movement when awake, the only artifact-free results were seen during sleep or quiet rest. B-waves (Fig. 1) were present in all recordings, and 90% of patients had plateau waves and near plateau waves. All 8/8 patients who underwent continuous CSF drainage reported improvement in their headache. There were no complications associated with Pcsf monitoring.

A Pcsf recording demonstrating B-waves (arrows) and normal Pcsf baseline.
Pcsf monitoring results

ND, not done; +, present.
All patients were treated either with a ventriculoperitoneal (VPS) or lumboperitoneal (LPS) shunt. Four had VPS and six had LPS. All reported improvement of their headache after shunt surgery (Table 4). Mean follow-up (F/U) duration was 24 ± 7 months. Fifty per cent of LPS were revised due to shunt obstruction. One VPS was revised for low-pressure HA (patient ♯ 1) and was later disabled.
Types of shunt and follow-up
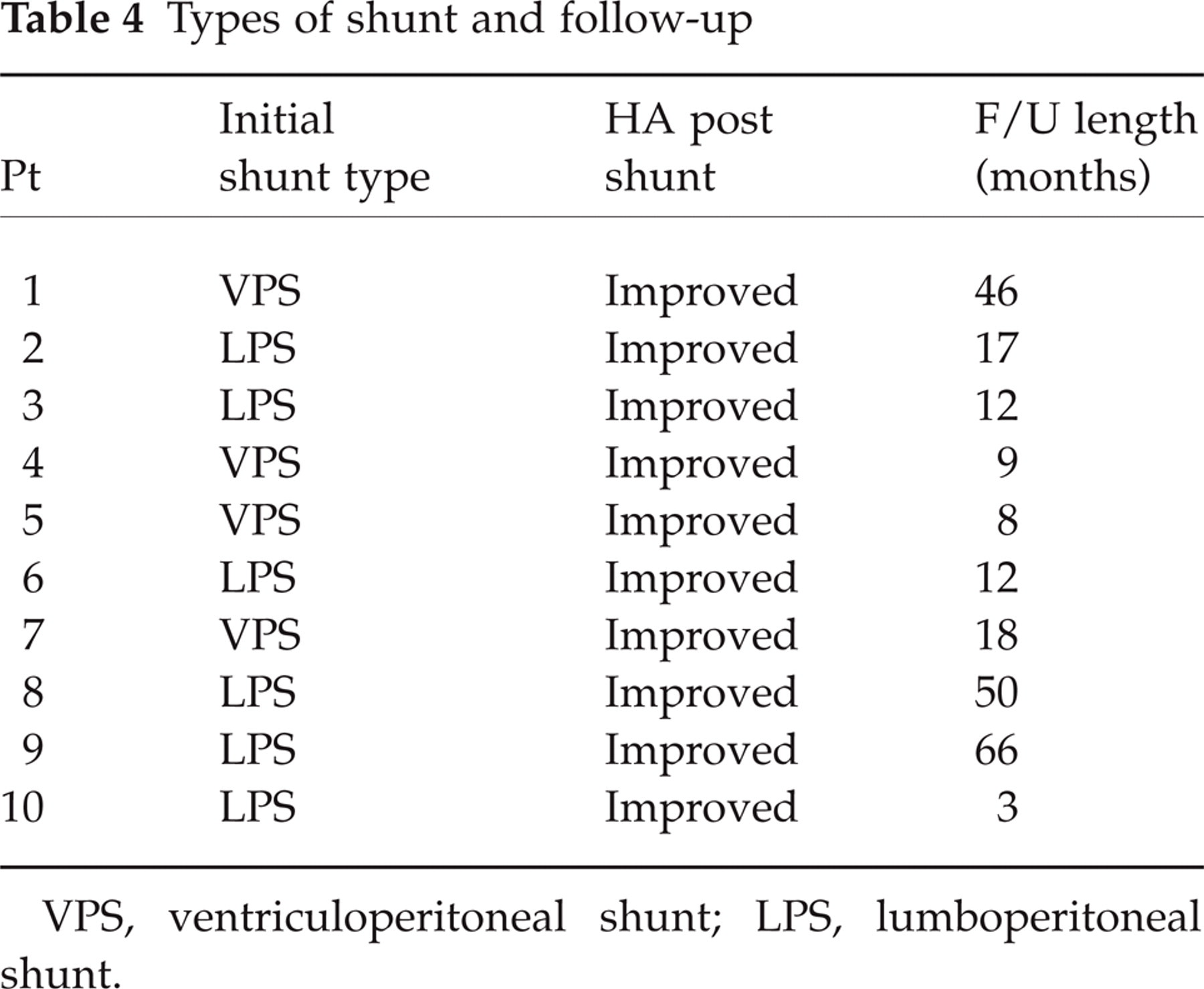
VPS, ventriculoperitoneal shunt; LPS, lumboperitoneal shunt.
Discussion
Our case series demonstrates the utility of Pcsf monitoring and controlled continuous CSF drainage in demonstrating the disordered Pcsf physiology present in a subset of CDH patients who have IIHWOP. We observed a normal resting Pcsf associated with intermittent elevation of Pcsf in the form of B-waves, plateau waves and near plateau waves during sleep. The presence of abnormal Pcsf waveforms, and the relief of headache with controlled continuous CSF drainage were considered evidence of perturbed Pcsf physiology sufficient to recommend and proceed with shunt surgery. Patients reported improvement in their headaches following shunt surgery.
In the last few years, several studies have shown that a number of CDH patients have IIHWOP when investigated with a lumbar puncture (4–7). Headache is the most common symptom, occurring in 90% of IIHWOP patients (16), and the headache profile is difficult to differentiate from CDH. There is no striking difference in patient characteristics between IIHWOP and CDH, except that IIHWOP is seen more frequently in obese women (4–6, 17). In a multivariable regression analysis, Wang et al. (7) found pulsatile tinnitus and obesity as independent predictors of IIHWOP. None of our patients reported pulsatile tinnitus and only 50% were obese.
Until a recently published report described a series of 10 patients with IIH with a higher proportion of men (64%) who were less likely to be obese (18), idiopathic intracranial hypertension (IIH) was thought to be mainly a disease of obese women of childbearing age with a female : male ratio of 8 : 1 (19–21). Patient characteristics in IIHWOP differ from IIH, with a lower female/male ratio, and obesity prevalence varying from 58 to 80% (5, 6). Obesity is even less common in CDH, with a prevalence of 45% (7). Our patients appear to have characteristics closer to CDH than to IIHWOP.
The non-specific headache presentation and the lack of papilledema make the diagnosis of IIHWOP dependent on LOP measurement, a point that Silberstein and Corbett emphasize in distinguishing IIHWOP from CDH (8). There is a wide range of LOP (230–450 mm H2O, or 17–33 mmHg) in IIHWOP (6, 7). In normal patients, whether obese or not, LOP between 200 and 250 mm H2O (15–18 mmHg) measured in the lateral decubitus position is not necessarily abnormal (12, 22, 23). Five patients (50%) in our series had LOP < 250 mmHg; hence making the diagnosis of IIWHOP less conclusive if LOP was the only criteria.
Lundberg's was the first to describe the different abnormal Pcsf waveforms (15). Plateau waves or near plateau waves are usually associated with symptoms of intracranial hypertension. Near plateau waves are similar in morphology and duration to plateau waves with the exception that Pcsf does not reach 50 mmHg. B-waves are believed to be an indication of poor intracranial compliance. So higher B-waves amplitude is associated with poor brain compliance. Little is known of the characteristics of normal Pcsf during sleep. Normal primates have low amplitude plateau waves reaching 12–13 mmHg (163–177 mm H2O) during desynchronized sleep, but no B-waves (24). Alterations in Pcsf during sleep are well known in patients with NPH and other intracranial pathology, typically with the B-waves (10, 25–27). These ICP changes during REM sleep in hydrocephalus may be related to increased cerebral blood flow and impaired CSF resorptive mechanisms (28–30). Continuous Pcsf monitoring has been proven useful in the diagnosis of NPH. Only 65% of patients diagnosed on clinical criteria alone improved with shunting compared with 96% of patients with abnormal Pcsf waveforms and high amplitude Pcsf pulse pressure (31–36).
Resting Pcsf during continuous monitoring is often normal in IIH (9, 37, 38) and IIHWOP (11, 39). In both IIH and IIHWOP, resting Pcsf has been found to be below 15 mmHg (204 mm H2O) (11, 38), or not significantly elevated (9), although Gjerris reported a mean ICP of 22.5 mmHg (306 mm H2O) with a range of 8–45 mmHg (109–612 mm H2O) in 14 patients with IIH (37). Our results show that both a normal baseline Pcsf and patterns of unstable, elevated Pcsf waveforms often co-exist.
None of these studies compared LOP and Pcsf. In our series, we found that LOP was higher than the resting Pcsf. A possible explanation for this difference may be stress, anxiety or pain associated with the LP that could falsely elevate the LOP, whereas resting Pcsf was recorded during quiet rest or sleep. Thus, the LOP, a ‘spot-check’ of Pcsf, may not be an accurate marker of Pcsf perturbation in patients in whom Pcsf happens not to be elevated at the time of LP (9), or in whom it is falsely elevated.
In our series, the unequivocal demonstration of abnormal Pcsf waveforms during Pcsf monitoring played a vital role in confirming the diagnosis of IIHWOP and in supporting the decision to proceed with shunt surgery. Our findings have possible diagnostic and therapeutic implications for patients with CDH. The proportion of patients with CDH who actually have IIHWOP is unknown, and it is difficult to differentiate between CDH and IIHWOP based on the headache history or the presence of normal LOP. Hence, our results suggest that 24–48 h continuous Pcsf monitoring and a controlled continuous CSF drainage trial is a useful tool for distinguishing IIHWOP from CDH, and should be studied prospectively.
The question that remains unanswered is how should we classify patients with CDH in which LOP was normal or slightly abnormal and Pcsf monitoring demonstrate abnormal wave forms? Should these patients be classified as IIHWOP or should we classify these syndromes according to the common pathophysiologic mechanism (intracranial hypertension) and further described by aetiology (idiopathic or symptomatic) and clinical presentation (e.g. chronic daily headache, presence or absence of papilledema)? The only way that this question would be appropriately answered is by designing a prospective evaluation of CDH patients with Pcsf monitoring. In Figs 2 and 3 we suggest an algorithm for management of patients with refractory CDH
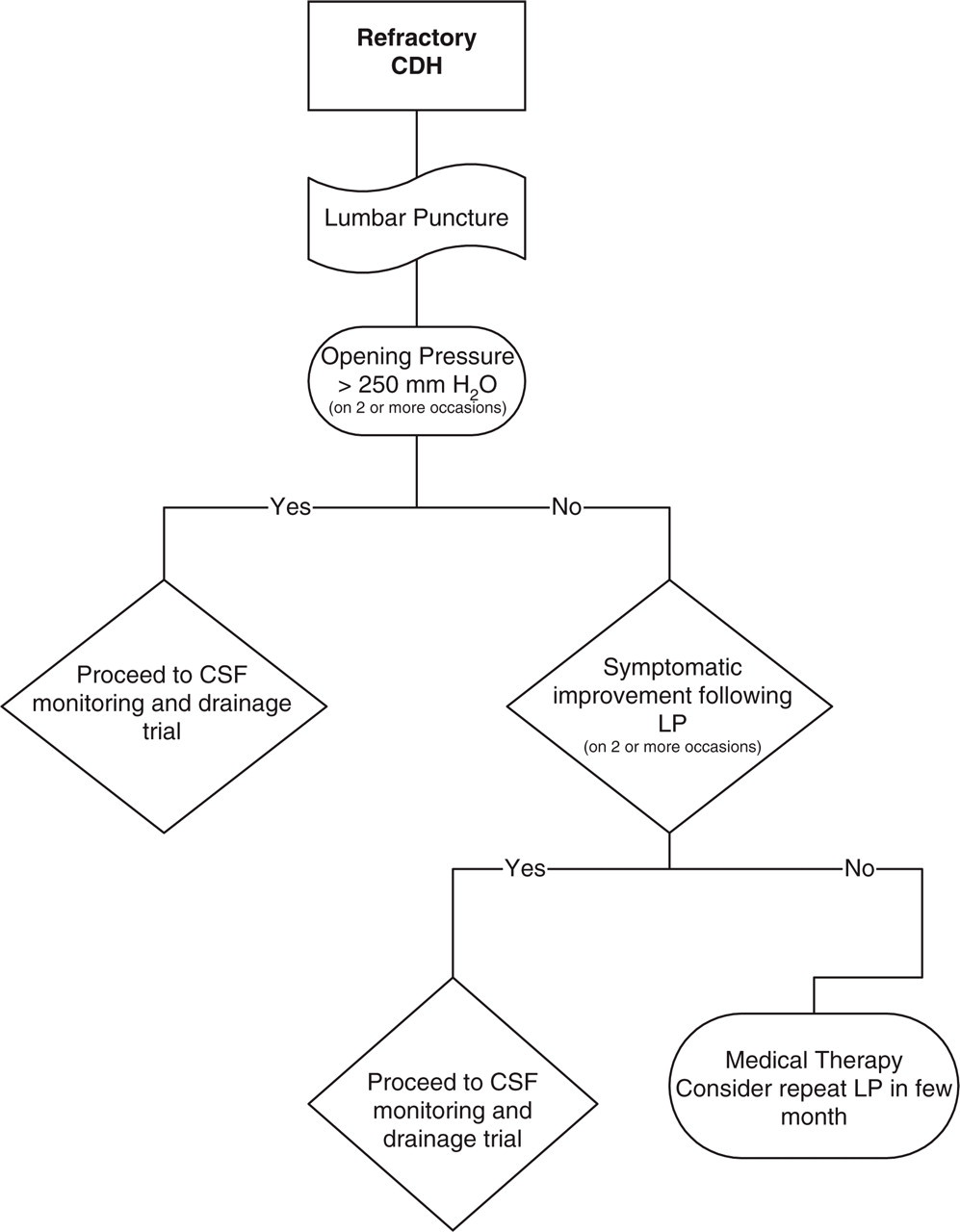
Algorithm for CSF monitoring and drainage trial in patients with refractory CDH.

Algorithm for shunt surgery following CSF monitoring and drainage trial in patients with refractory CDH.
This study has some limitations. First, it is retrospective and may be subject to referral bias. Secondly, several different referring physicians performed the initial LP. This may predispose to variability in reported opening pressures. Thirdly, the LOP and Pcsf monitoring were performed weeks or months apart. Thus, it is possible that the underlying Pcsf pathophysiology may have changed between LOP measurement and Pcsf recording, thereby limiting the strength of any conclusions about the LOP. Fourthly, details about the clinical improvement following shunting is subjective due to the retrospective nature of the study. Nonetheless, continuous Pcsf monitoring demonstrates that there are significant differences between awake and asleep Pcsf that are likely to be reflected in the LOP obtained in awake patients.
Demonstration of pathological Pcsf patterns by continuous Pcsf monitoring was essential in confirming the diagnosis of IIHWOP, and provided objective evidence to support the decision for shunt surgery. Increased Pcsf was seen mostly during sleep and was intermittent, suggesting that Pcsf elevation may be missed by a single spot-check LOP measurement. Shunting was beneficial in IIHWOP. The clinical similarity between IIHWOP and CDH suggests that continuous Pcsf monitoring may have an important diagnostic role that should be further investigated.
Footnotes
Acknowledgements
We wish to thank Dr Neil Miller for his thoughtful review and suggestions for this manuscript. Dr Geocadin is supported by the Corporate Roundtable Clinical Training Fellowship Award of the AAN Educational Research Foundation. This work was presented at the 53rd Annual Meeting of the American Academy of Neurology, May 5–11, Philadelphia, PA.