
Abstract
Headache diagnosis and treatment is the most important focus or concentration area for practising neurologists in America. The American Headache Society, formerly the American Association for the Study of Headache, is made up predominantly of neurologists. Recognition of the importance of the teaching and practice of headache medicine, especially migraine, is still incomplete at many academic teaching institutions. Suggestions that this results from inadequate academic hierarchies and education at graduate and post-graduate levels have been made. We therefore undertook a survey of academic practitioners of headache medicine in departments of neurology with membership of the American Headache Society. Subjects and addresses were identified using the 1999-2000 membership directory of the American Headache Society. Practice characteristics and time distribution were assessed. Teaching in undergraduate and resident programmes was also assessed. Fifty-five surveys from 46 institutions in 25 states were judged as adequate for this report. Academic neurologists with interest in headache medicine spent most of their time in clinic, with less than 25% spent doing either research or teaching. Medical schools had an average of 1 h of preclinical and 2 h of clinical teaching in headache. Neurology residents received an average of 3 h of didactic instruction in headache. This report is the first of its kind to review the practice characteristics and culture of headache medicine in the setting of academic departments of neurology. It describes a clinical practice similar to those of other non-academic American neurologists.
Introduction
A major barrier to the best care of patients with headache results from inadequate academic hierarchies dedicated to headache medicine, and the lack of authoritative subspecialists (1). Compelled by the discovery of effective acute treatments for migraine, improvement in preventive and chronic management strategies for headache, and the continuing explication of processes underlying the primary headaches, academic headache medicine would appear to be a legitimate area of study and practice. The impact of headache medicine in the academic arena has not been assessed.
The membership of the American Headache Society (AHS), formerly the American Association for the Study of Headache, consists predominantly of neurologists. In recent decades, Neurology has been faced wth special challenges. An initial fear of over-supply (2) was followed by managed care and its attendant demands for quality assurance (3, 4). Yet neurology trainees continue to see academic careers as desirable. Only orthopaedic and radiology residents compare with neurology trainees in this preference (5, 6). To that end, 75% of neurology residents pursue fellowships (7), and 44% that plan academic careers realize their intention (5). As in other residencies (8), Neurologists-in-training will locate at institutions where there is an established subspecialty presence or known mentor (5).
In the recently published practice survey from the American Academy of Neurology (AAN), 50.5% of American neurologists identify caring for patients with headache as their primary practice focus or concentration. Epilepsy and cerebrovascular disease were listed numbers two and three (9, 10). This would imply, ideally, that the academic commitment to headache practice, research and teaching is already well established. We therefore attempted to assess the practice characteristics and educational culture of academic neurologists with membership of AHS, designated for purposes of this report as American Headache Specialists in Neurology (AHSNs).
Methods
Since no formal list of headache specialists in academic departments of neurology was available, visual inspection of the 1999–2000 Membership Directory of the AHS was performed. Inclusion was determined based on academic address or recognized expertise and academic affiliation. A total of 181 surveys were mailed with self-addressed stamped envelopes and return fax numbers. Questions included geography, institutional affiliation and department in addition to academic rank. Those identified as neurologists were then reviewed. Practice characteristics included division of time amongst Clinic, Research and Teaching. Per cent time was divided into groups: 0–<25, 25–49, 50–74, 75–99, and 100. Clinical practice was described according to the number of new and follow-up patients seen per week, and average time per visit. Medical school teaching was reported on the basis of the presence or absence of a medical school lecture, the year or years in which they occurred, the number of hours dedicated to headache teaching. The presence or absence of a medical student elective in headache was also requested. Didactic resident teaching was assessed on the basis of the presence or absence of a headache lecture in the individual's department of origin. A sample of respondents claiming 100% academic time who practice headache medicine at least 75% of the time was also described.
Results
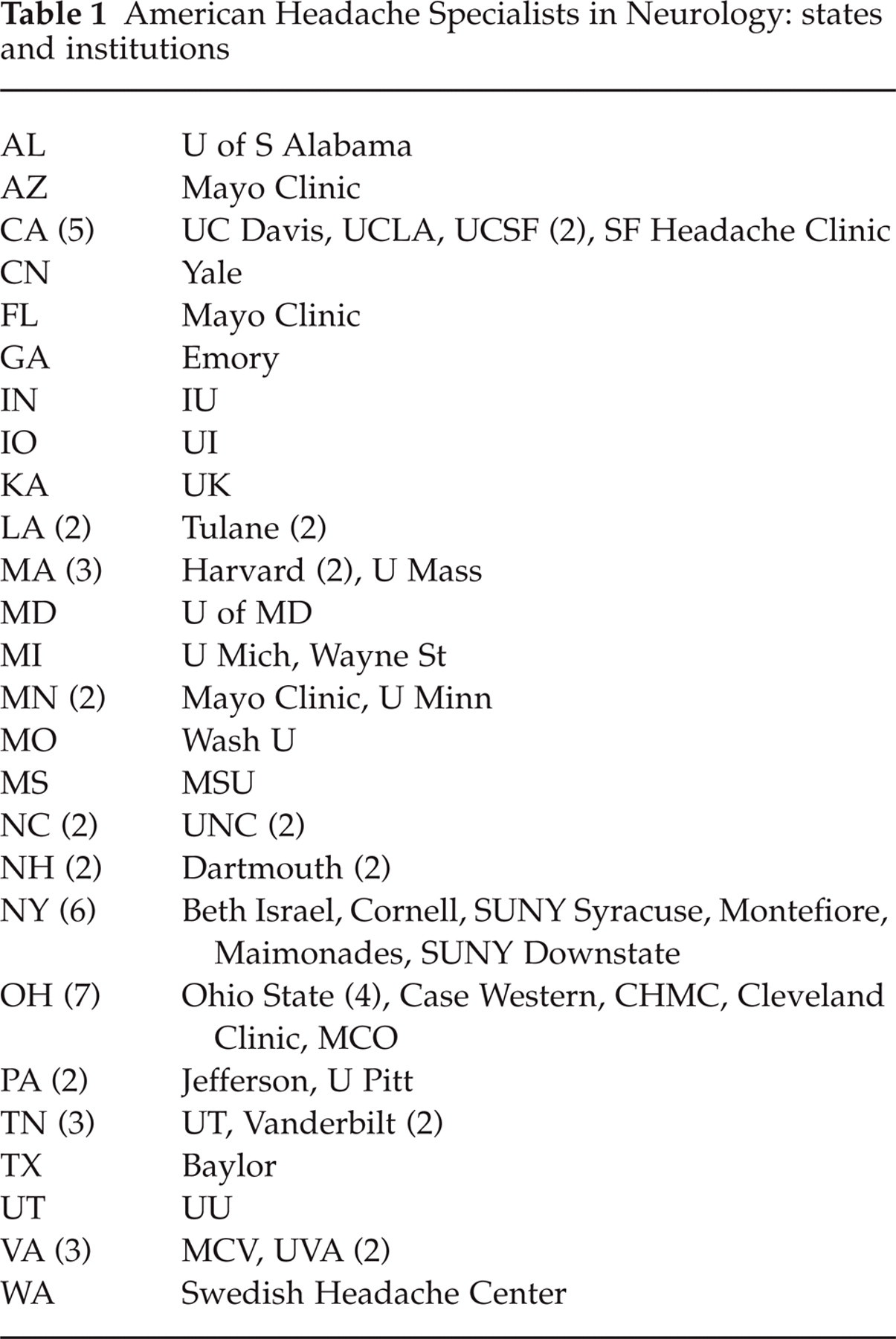
Fifty-five neurologists returned the questionnaire with one living outside of the USA. Fifty-four AHSNs represented 45 institutions in 26 states (Fig. 1; Table 1).

American Headache Specialists in Neurology attended at 45 institutions in 26 states. Eighteen (33%) of respondents live in Ohio, New York or California.
American Headache Specialists in Neurology: states and institutions
Academic practice
Amongst AHSNs there were 18 full professors (33%), 19 Associates (35%), nine assistants (17%), and four clinical instructors. Four listed themselves as department chair, director or division chief. Thirty-six of 44 were full-time academics, with an additional 7/44 part-time or appointed, and 11 not reporting per cent time academic. Thirty-eight of 49 identified themselves as ≥ 75% of time academic with 22/49 describing ≥ 75% of time specifically dedicated to headache.
Time distribution
Forty-five of 50 spent at least half (mean 56 ± 15%) of their time in clinic. Thirty-seven of 48 stated that they spent < 25% of their time in research. Teaching occupied < 25% of academic time for 43/49 (Fig. 2).

Time distribution: American Headache Specialists in Neurology spent at least half (mean 56 ± 15%) of their time in clinic (); 57.6% spent < 25% doing research (□); 80% spent < 25% teaching (▪).
Clinical practice
Clinical practice occurred predominantly in hospital clinics (34/43), followed by free-standing clinics (5/43) and private clinics (4/43). The average number of new patients seen per week was 7.0 ± 4.4 (median nine, range 1–60), with an average new patient visit lasting 53.3 ± 11.5 min (median 60; range 30–120). Clinicians saw 31.6 ± 30 (median 20; range 2–150) patients for follow-up per week, with the average visit lasting 22.5 ± 8.7 min (median 22.5; range 15–60).
Research
The majority of AHSNs (37/48) spent < 25% of their time in research endeavours while 7/48 (14%) spent 50% or more (Fig. 2). The content of this research was not explored.
Teaching–medical school
Institutionally, 36/43 medical schools responding contained a lecture in headache. For schools with one lecture, 10/19 occurred in the second year. Thirteen of 34 had more than one lecture, with 5/34 having more than two. Headache medicine electives were available at 15/44 schools. These occurred predominantly in the 4th year (Fig. 3). Didactic hours of headache medicine teaching by AHSNs at the represented institutions were two or less for 27/34 of respondents (mean 1.3 ± 0.6; median 1).
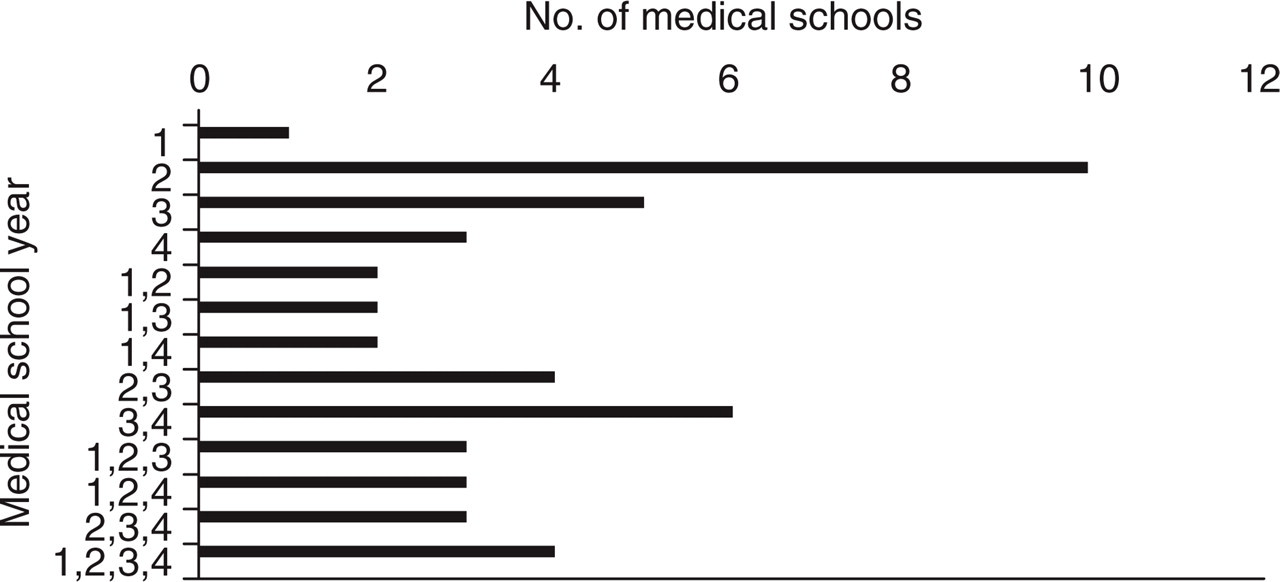
Medical school lectures by year. Eighty-four per cent contained a lecture in headache. The majority occurred in the second year. Seven of 42 had no scheduled lecture.
Teaching–neurology residents
Neurology resident lectures were given at 38/43 of the surveyed schools. Thirteen of 38 gave yearly lectures across all the house staff years. Lecture hours averaged 3 per training experience (median 3, mode 4, range 1–4+). Clinical headache time for residents was not recorded.
Full-time AHSNs
Fifteen respondents claimed to be 100% academic, with at least 75% of their time dedicated to headache. This group spent an average of 60 ± 16% of their time in clinic. Three of 15 reported that they spent > 25% of their time in research endeavors. Thirteen of 15 reported the presence of a medical school headache lecture. Medical school electives in headache were available at 6/15 (40%). By contrast, in the group with < 50% time in headache, a medical school elective was available at 7/20 (35%) of schools. Three of 15 full-time AHSNs reported no resident headache lecture for their department.
Discussion
Neurologists account for approximately 2% of American physicians (11). The membership of the AAN was 11 300 for the years 1999–2000 (9). The American membership of the AHS in 1999–2000 was 1270. Our surveyed cohort represented 4% of the total membership of AHS. We found the highest concentration of neurologists in academic headache practice in New York, Ohio and California (Fig. 1). This did not parallel the concentration of all neurologists except in New York (5.2/100 000). Ohio (3.0/100 000) and California (3.2/100 000) had the second lowest neurologist to population ratio (3–3.9/100 000). Both fell into the lower end of the middle third of American neurologists per capita per state (9).
Of the respondents to the AAN practice survey (9), 41.3% were full-time academic faculty, while our review of the membership directory of the AHS showed that approximately 10% of the membership are academic neurologists (data not shown). Of the membership of the AAN, 39.1% were fellowship trained. The number of fellowship-trained subspecialists in our survey was not known, and no American Board of Medical Specialist-approved fellowship in headache medicine exists.
Practice activity was defined in the three domains of Patient Care, Research or Education. The amount of time spent in each domain by academic neurologists in headache medicine was similar to that of other practising neurologists (Fig. 4). AHSNs saw approximately the same number of new patients as other academic neurologists, both seeing fewer than all neurologists combined. But AHSNs saw as many follow-up patients as all neurologists and many more than AAN full-time academic neurologists (Fig. 5).
Comparison of time distribution per activity for all American Academies of Neurology (AAN) vs AAN full-time academic vs American Headache Specialists in Neurology (AHSN). □, Research; ▪, teaching; , clinical practice.
New and follow-up patients seen by all neurologists, American Academy of Neurology (AAN) academics and American Headache Specialists in Neurology (AHSNs). □, AAN–all; ▪, AAN–university; , AHSN.
In ten neurology departments containing AHSNs ranging in size from 10 to 82 faculty members, full-time headache specialists ranged between 2% and 13% (mean 9%) of the total. The range for epilepsy was 4–24% (mean 14%) and for neuromuscular disease was 3–20% (mean 12%) (data not shown, AHSNs personal communications). From Neurologist 2000 (9), 50.5% of American neurologists listed headache as their number one focus area, closely followed by epilepsy (46.4%). Neuromuscular disease was listed as number 9 (31.1%). Of neurologists, 77.4% reported that they provided extended or long-term care for headache patients with 25.6% providing the same form of care for epilepsy patients. It should be noted that since 1998 the percentage of neurologists providing long-term care for headache increased from 68.6 to 77.4%, whereas those numbers for epilepsy dropped from 78.4 to 25.6% (9).
The mission of academic medicine is to provide the highest quality clinical, educational and research opportunities. This descriptive study offers some insight into the practice of academic headache medicine in a select small group of neurologists in the USA. The practice culture for AHSNs appears to parallel that of non-academic neurologists. The clinically demanding schedule they describe has the potential to threaten their ability to compete for increasingly scarce departmental and extramural funding resources (11). Extended patient visits (1 h new and 30 min follow-up) combine with the paucity of procedures available to the typical headache specialist to thus mandate attendance at busy clinics in order to generate income. With the additional levies on income imposed by the medical school complex (12, 13), there is a perception amongst AHSNs of lower income potential compared with headache specialists in private practice. Coupled with the higher level of illness that is typically referred to academic medical centres (14), the day-to-day clinical practice of AHSNs may limit their ability to participate in teaching, research and publication. AHSNs therefore may represent an example of two-tiered academic practice (12), where the demand for patient care proscribes all other activity. Only 12 AHSNs in our survey were spending more than a quarter of their time doing research, making it even less likely that a first-tier academic community of neurology-trained headache specialists can grow and be maintained. This is also reflected in the academic rank of those in this ‘best case scenario’ study (15), where younger, less experienced, but perhaps more creative and energetic members are not the majority of AHSNs.
The major problems with a study such as this are its small sample size, selection and response bias, and incomplete data. Given the clinical experience of most headache specialists in academia, though, this may also have resulted in an underestimate of time distribution, since the group who did respond may represent a ‘best case scenario’ (15). Assuming this, AHSNs as pertains to research resemble other neurologists in America. Our survey used < 25% as the lower end cut-off, leaving the lower limit unavailable for comparison. This environment for research is also muddled for the AHSN by the observation that no specific calls for migraine or headache research are currently available via the National Institutes of Health (16). In response to this, many academicians have courted pharmaceutical industry clinical trials unsuccessfully, losing to more expedient systems where Investigational Review Boards are centralized, and highly developed data collection systems are available (17, 18). These systems are not well developed in the typical department of neurology (19, 20), resulting from the need to interact with the larger academic institution, longer and more detailed review processes and patients requiring complex and integrated disease management strategies (21). Making academic neurology more research friendly (8, 22, 23) for AHSNs may involve an increase in both clinical and basic research in headache, although the level of advocacy for this subspecialty in departments of neurology remains unknown (13).
Lastly, the domain of education also presents significant challenges to AHSNs. Of medical schools with headache lectures, 61% have only 1 h dedicated to this subject. That about half of the lectures occur in preclinical (1 h) and half in clinical years (2 h) suggests that some schools get lectured in the basic science curriculum, and others during clinical rotations. Does this allow enough exposure to correlate the didactic and clinical aspects of patient care? (24). That this same question exists in the area of stroke education should not give much comfort (15). Also, the finding that amongst the most dedicated AHSNs there are two institutions without a medical school lecture raises additional questions of the ability of the curriculum to keep pace with medical knowledge and advances.
The paucity of elective headache training for medical students denies the opportunity for mentoring from a specialist dedicated to the field. Career choice amongst medical students is defined by the attitude of mentors (5). The experience in family practice has highlighted the importance of positive mentoring (25) and the powerful influence of negativity on career choice (26–28). Whether those students interested in headache are receiving negative messages about the care of headache patients is not as well delineated as the ‘maligning’ of those interested in family practice (29), but anecdotally, many AHSNs report that within and without their department they are given less ‘capital’ than those in other neurological subspecialties. The opportunity then for positive mentoring of students interested in headache medicine may be lost to the sparse exposure, few course options and perceived negativism towards their area of interest. This may also be reflected in the relatively small number of assistant professors.
Lastly, the presence of a full-time and dedicated headache specialist does not guarantee that the institution of practice provides a headache lecture or elective for matriculating medical students. Three neurology programmes with full-time AHSNs did not have a lecture for their own residents in training.
In conclusion, this descriptive study was not intended to disprove the null hypothesis: ‘Academic neurologists in headache subspecialty are not the same as other neurologists in general or specialty practice’. Therefore, and because of diverse and highly selected sources of data, it should be viewed as a first look at an important area of activity, i.e. academic headache practice in departments or divisions of neurology. Future areas of research should include more comprehensive surveys of American departments of neurology, and assessment of strategies for improving headache education for students and residents and effecting change in the culture of academic headache practice.