
Abstract
During 1981–96 a series of 60 consecutive out-patients was examined in relation to an assumed first period of cluster headache (CH). On follow up in 1998 we found that six were deceased at a mean age of 56.5 years (range 45–74 years), of whom one had a definitive CH diagnosis and five had one documented headache period only. Six patients were lost to follow up because they could not be reached. In the final group for evaluation (n = 49) it was found that 13 (26.5%) patients had had one cluster period only during a mean observation time of 8.9 years. Out of 36 patients with a definitive CH diagnosis according to International Headache Society (IHS) criteria, 31 patients had episodic CH, four patients had primary chronic CH and one patient had secondary chronic CH. Of the patients with a definitive CH diagnosis, 83% on follow up had had a recurrence of a second period of CH within 3 years or continuous attacks (chronic/semichronic CH) from the onset. Evidently some patients may suffer from one cluster period only. In our patient material only 17% had a second cluster period after 3 years.
Introduction
Cluster headache (CH) is characterized by recurrent, unilateral, short-lasting attacks of severe headache. Attacks most commonly occur in clusters, so called cluster periods. According to the International Headache Society (IHS) (1), two or more cluster periods are required for a definitive CH diagnosis (2, 3). Several studies have been performed concerning the natural history and the prognosis of CH, but as far as we know there are no previous studies following patients prospectively from the onset (4–9). It is not known whether some patients get one single period only of CH during their lifetime. The aim of this study was to evaluate the prognosis after one typical cluster period as regards the risk of catching a second cluster period and the time to recurrence.
Patients and methods
During 1981–96 a consecutive series of 60 patients was examined at the Department of Neurology at Söder Hospital, Stockholm in relation to an assumed first period of CH (1, 10). In 1998 the clinical data recorded at their first event were reviewed according to IHS criteria, and it was again established that they had CH except that periodicity could not be defined. The follow up case records of these 60 patients showed that 28 patients (group 1) had received a definitive CH diagnosis over the years. For 32 patients, however, there was no documentation in the records as regards the subsequent course of their headaches and the aim was to contact these patients (group 2).
All patients were checked against the National Registry of Population as regards life status and present address. The patients in group 2 were to be reached by a letter of information telling them that they would be contacted by telephone for a structured interview as regards the possible recurrence of headache attacks of a similar type to which they had previously been examined for. The letter would present a number of structured diagnostic questions to be answered in the telephone interview. If not reached by the first letter or by telephone, a second letter with the same questions was mailed, with the instruction to return the questionnaire by mail. A flow chart of the procedure is shown in Fig. 1 and demographic data of the patients are shown in Table 1.
Age at onset in 60 patients to be followed up after a first period of cluster headache (CH)

1: Definitive CH according to case histories.
2: Only one cluster period documented, patients to be contacted.
Group 1: 21, 22, 22 and 63 years, respectively.
Group 2: 50, 57 and 66 years, respectively.
Twenty-one, 22, 22, 50, 57, 63 and 66 years, respectively.

Flow chart of the follow-up procedure. Thirty-one patients were found to suffer from episodic cluster headache (CH) (group 1 + 2), five patients had chronic CH (group 1).
The study was approved by the local Ethics Committee.
Results
Altogether six patients were found to be deceased. One patient had several documented cluster periods but for five of the six patients there was only documentation of the initial headache period. Age at onset, age and cause of death are shown in Table 2.
Demographic data of six deceased patients in a series of 60 patients followed up after an assumed first period of cluster headache (CH)

Six patients from group 2 were lost to follow up because they could not be reached by telephone or by letter. The final group for evaluation of prognosis as regards CH thus included 49 patients, including the deceased patient with CH diagnosis from group 1.
Patients with one CH period only
In total 13 (26.5%) out of 49 patients had not suffered any further cluster periods during a mean observation period of 8.9 years (median 8.0 years, range 2.5–17 years). The only female had her first cluster period at the age of 66 years, and she had no further bouts during the following 9 years. The mean age at onset among the 13 patients was 40.8 years (median 40 years, range 23–66 years) and the mean duration of the first period was 3.7 weeks (median 4 weeks, range 1–8 weeks) as shown in Table 3.
Age at onset, duration of first period and time to recurrence in 60 patients, on follow up subdivided into groups of patients with one period only, episodic cluster headache (CH), primary and secondary CH, deceased and patients lost to follow up

One week duration of first cluster period, second period after 3 months (duration 1 month). Thereafter remissions 2–4 weeks between bouts. Four years after onset beginning of chronic pattern and regarded as secondary chronic.
The patient with the shortest observation period, 2.5 years, had been prescribed isosorbide nitrate for angina pectoris 3 months before onset of the headache attacks. He had one to three severe right-sided CH attacks daily for 1 month, and the pain was associated with nasal congestion, ptosis and conjunctival injection. When he was told to discontinue the medication the attacks stopped and have not returned.
Another male patient (age 23 years at onset) had fallen in a stairway and had a mild head injury 1 week before the onset of cluster attacks. The pain occurred while he was drinking alcohol, and he then suffered typical short attacks with severe pain and lacrimation for a single period of 8–9 days. The patient was then free of headaches for an observation period of 7 years.
All patients could easily describe their symptoms although their headache attacks had occurred several years before the telephone interview. They remembered the headaches as very painful, like no other headache. Two patients said that they had their headaches during a period with severe psychological stress.
Patients with a definitive CH diagnosis according to IHS criteria
In group 2 eight male patients verified at the telephone interview that they had suffered two or more further periods of CH and thus they fulfilled the IHS criteria for episodic CH. Five of these patients could tell when they had got their second period: after 4.5 months, 6 months, 1 year, 2 years and after 3 years, respectively. Three patients had had several periods of headache, but could not specify when the second period had occurred. They all believed that they had had their second period within 3 years after the first period. One of them had had recurrent attacks of pain, especially when drinking alcohol, but for short time periods, 3–4 days only.
Four of the eight patients who had suffered more than one period had personal contact with a local doctor. They were helped by sumatriptan subcutaneously. Four other patients had no contact with a doctor. They said that they were familiar with the pain, they knew that it is transient and they handled the pain by over the counter analgesics such as acetylsalicylic acid and paracetamol. One patient knew the symptoms well because his mother had suffered from CH.
Altogether 36 patients in groups 1 and 2 had a definitive CH according to the IHS criteria on follow up. Four of them had primary chronic and one had secondary chronic CH. The remaining 31 patients suffered from episodic CH. On follow up it was possible to ascertain the approximate time to recurrence in 25 patients. It was found to average 2.25 years (median 2 years, range 0.25–11.4 years). For six patients (three from group 1 and three from group 2) there are no exact data about the time to recurrence. However, they had a recurrence no longer than approximately 3 years after onset according to case records and telephone interviews, but more exact data were difficult to obtain. Thus 30 (83.3%) out of 36 patients with a definitive CH diagnosis on follow up either had suffered from continuous attacks from the onset or had got a second period within 3 years. Thirty-four patients (94.4%) had a recurrence within 5 years, as shown in Table 4. One patient had an 11-year-long remission between onset and the second cluster period, without any obvious trigger factor for this late recurrence. The incidence of a second period of CH after 3 years in our material was about 17%.
Approximate time to recurrence for 36 patients with a definitive cluster headache (CH) diagnosis on follow up
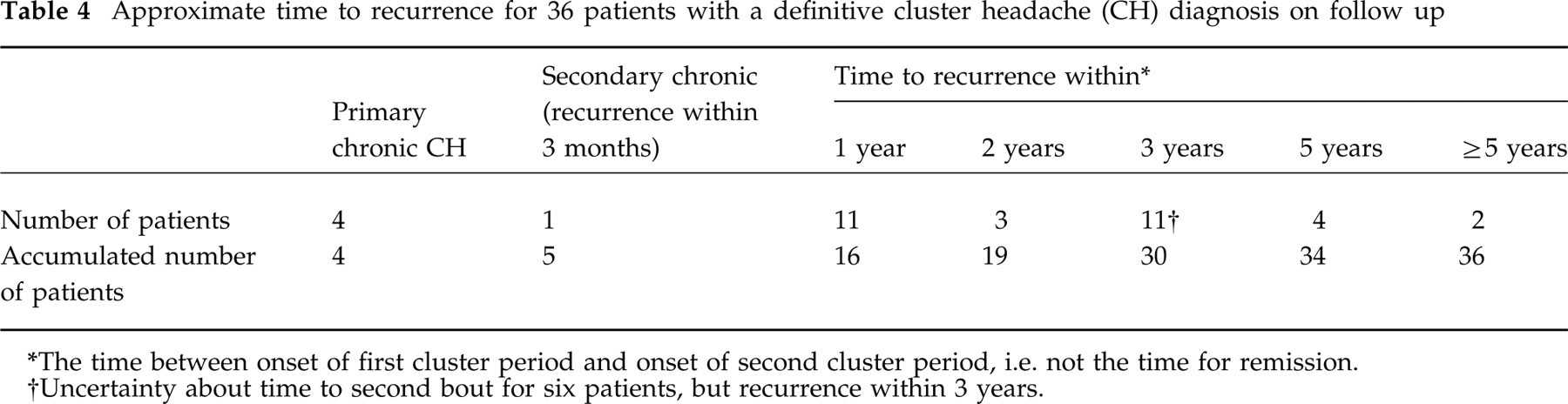
The time between onset of first cluster period and onset of second cluster period, i.e. not the time for remission.
Uncertainty about time to second bout for six patients, but recurrence within 3 years.
We observed that the patients with only one period on follow up had a shorter duration of the first period (mean 3.7 weeks) than the deceased patients with only one documented period (mean 9.5 weeks) and the patients with episodic CH on follow up (mean 7.6 weeks), as seen in Table 3. Furthermore, the patients with one period only were slightly older at onset but otherwise the symptomatology was similar to those with a definitive CH diagnosis.
Discussion
Most commonly patients come to the neurologist for a confirmation of the diagnosis after several cluster periods. To our knowledge this is the first follow-up study of consecutive CH patients examined during an assumed first period of headaches. According to the IHS criteria two headache periods are required for a definitive diagnosis of episodic CH. After a mean observation period of 8.9 years 27% (13/49) of our patients still had had only one cluster period. Our study also showed that 83% of the patients with a definitive CH diagnosis had their second cluster period within 3 years and 94% within 5 years. The time to recurrence for those 31 patients who had definitive episodic CH varied from a few months to about 11 years, while the observation period for those with one period only varied between 2.5 and 17 years. It is therefore likely that some of the patients with the shortest observation times still may show up with a second cluster. On the other hand, most patients with a definitive CH had their second period within 3 years as mentioned above. In a forthcoming revision of the IHS criteria the diagnosis ‘CH periodicity undetermined’ should be discussed in more detail. In the IHS classification episodic CH is characterized by periods lasting from 7 days to 1 year. Sjaastad has suggested that headache periods lasting for 3–6 days might be termed ‘mini-bouts’ and those of ≥1 week ‘regular bouts’ (11). It is not known whether there are any differences in the long-term course between these two varieties of the disorder.
The issue of recall bias should be taken into consideration, since some patients were asked to recall retrospectively when the second cluster period occurred in relation to the first period.
Interestingly, some patients with such a severe periodical pain as CH do not consult a doctor at recurrence of headache attacks. The patients explained that since they were familiar with the pain there was no need to see a doctor continuously. They had received careful information in conjunction with their first visit to our Department and knew that the pain could recur
One patient got his first cluster period shortly after oral medication with isosorbide nitrate, and the pain totally disappeared after discontinuation of this medication. There might be a connection with his medication, since nitro preparations may provoke cluster attacks during an active period of CH. This is also interesting since Kunkel & Frame reported on two patients with chronic CH who had no further cluster attacks after coronary by-pass surgery (12). Could there be a relation to the cure of angina pectoris as such, for instance by diminished release of vasodilatating peptides counteracting the previous coronary ischaemia and perhaps predisposing to CH? Another possible reason for CH remission is that the patients stopped medication with nitroglycerin after surgery.
There is a remarkably high mortality at a relatively young age in the group with only one cluster period documented. The mean time between time of onset of CH and time of death for these five patients was as long as 11.6 years, but since we do not have any case records after the initial visits it is not possible to draw any conclusions as regards any connection between CH and death in these patients. CH patients are known to have a high tobacco consumption (13). The causes of death in our patients may be related to lifestyle factors, since three patients had bronchial carcinoma and one died from intoxication.
We have noticed that the patients with one period only were slightly older at onset, but our material does not allow any conclusions about the prognosis in relation to age.
In conclusion, we found that some patients with cluster headache may suffer from only one period during many years or even in their lifetime, and that most patients with a definitive CH diagnosis probably recur within 3 years. The incidence for a second period after 3 years in our material was about 17%.
Footnotes
Acknowledgement
This study was supported by a grant from Glaxo Wellcome, Sweden.