
Abstract
Five hundred and fifty-four patients with episodic cluster headache (ECH) and chronic cluster headache (CCH) were examined between 1963 and 1997. Mean age at onset was significantly higher in women with CCH compared with women with ECH and in men with ECH or CCH. In women with CCH age at onset was evenly distributed from 10 to 69 years, whereas in men with CCH and in both sexes with ECH, there was a peak when they were in their 20s. In women with ECH a second peak of onset occurred in their 50s. Although not statistically significant, primary CCH started later in women (mean 50.8 years) than secondary CCH (mean 35.5 years). There was a significant variation in the male : female ratio with respect to age at onset, being largest between 30 and 49 years of age (ECH 7.2 : 1; CCH 11.0 : 1) and lowest after 50 (ECH 2.3 : 1; CCH 0.6 : 1). During the observation period of more than 30 years there was a trend towards a decreasing male preponderance; the male: female ratio was significantly higher among patients with onset before rather than after 1970. The proportion of episodic vs. chronic CH did not change during the study period. The nature of the sex- and age-related pattern of cluster headache onset remains to be elucidated but mechanisms associated with sex hormone regulation, perhaps of hypothalamic origin, may be involved, as well as environmental factors related to lifestyle.
Introduction
For unknown reasons cluster headache (CH) is a typically male ailment. More than 8 out of 10 afflicted patients have been reported to be males and the mean age at onset is generally between 20 and 40 years. In 18 series of altogether 3182 patients published between 1952 and 1983 (1) 84% were males (mean of means). If only series with at least 60 patients were considered there was an even higher mean of 88% males.
It was therefore most interesting when Manzoni (2) reported a decreasing trend of the male preponderance over time in a series of 482 patients consecutively referred to the University of Parma Headache Centre between 1976 and 1995. The ratio of males to females was shown to decrease successively from 6.2 : 1 in those patients who had an onset before 1960, to 2.1 : 1 in those with an onset between 1990 and 1995. It was suggested (3, 4) that changes in lifestyle factors over the years, such as employment rate and smoking habits, in both sexes might have played a major role in changing the gender ratio of cluster headache.
The mean age at onset as derived from several papers is around 31.5 years. CH may begin at any age up to around 70. In Manzoni's study (5) approximately 80% had their onset in the second to the fourth decade. There was no significant difference in the age at onset between episodic cluster headache (ECH) and chronic cluster headache (CCH) (6).
There are only few reports that specifically discuss cluster headache in females (7, 8). The clinical symptoms do not seem to differ significantly between men and women. CH in women has been reported to start earlier than in men in two reports (6, 9) and later in one (10). There is a tendency towards a bimodal age at onset-distribution in women, with a number of sufferers having their first attacks after the menopause (7, 11). In his monography Kudrow (12) reported that ‘peculiar to the female distribution an increased frequency occurred between the ages of 50 and 60 years’, referring to our series and his own material of 70 female patients. This observation is still not understood and deserves further studies.
There are few epidemiological studies in cluster headache. In 9803 18-year-old Swedish army conscripts cluster headache was found in 0.09% (13). A population study of 21 792 inhabitants in the Republic of San Marino (14) yielded an overall prevalence of 0.07%. Although these investigations were published before introduction of the classification criteria of the International Headache Society (15), the results accord fairly well with those of Krogh Rasmussen et al. (16). In a Danish urban population of 740 subjects they found one case of cluster headache, i.e. yielding a prevalence of 0.14%. Summarizing available data Manzoni and Prusinski (17) assumed that the prevalence in the general population is about one per thousand. In Olmsted County, Minnesota, the overall age- and sex-adjusted incidence was 9.8 per 100 000 person-years or approximately 1/25 that of migraine (18).
Cluster headache is a rare disease. In order to study the epidemiology of cluster headache it is necessary to collect the case materials needed over long periods of time. In the present study we have analysed a personally examined series of cluster headache sufferers collected consecutively over more than three decades with special reference to any change in sex ratio over time and in relation to age at onset.
Patients and methods
Between 1963 and 1997 a total of 554 patients with cluster headache were seen personally on a consecutive basis at the Outpatient Departments of Neurology at Karolinska Hospital (1963–71), Söder Hospital in Stockholm (1972–96) and Huddinge University Hospital (1997). We included patients from the Stockholm County Council (n = 538, or 97.1%) and from outside this region (n = 16, or 2.9%). Nine of the latter lived in other distant parts of Sweden (seven male, two female) and seven came from abroad (six male, one female). Patients were referred to the Karolinska Hospital mainly from the northern parts of Stockholm, while Söder Hospital (medical area about 380 000 inhabitants) and Huddinge University Hospital mainly covered the southern parts of Stockholm County Council.
All patients that were referred to the clinic because of a strongly suspected or a definite case history of cluster headache were examined, irrespective of sex or age. Patients underwent a careful history taking and a thorough physical and neurological examination. Almost all were interviewed during the actual course of a headache period (cluster), usually only a few hours after a preceding attack. Furthermore, the interviews were repeated during clusters in most of the patients. Patients kept careful daily records of their attacks and most of them were continuously followed through two or more clusters of headache. In the 1960s one-third of the patients were directly observed once or several times during spontaneous or induced attacks.
Before 1988 ECH was diagnosed according to the criteria of Ekbom (9) and CCH according to Ekbom and Olivarius (19). After 1988 we used the criteria of the International Headache Society (IHS) (15), which, in fact, are in good agreement with the former criteria (20). All patients referred before 1988 also met the IHS criteria for cluster headache. Patients should have had at least two typical headache periods separated by free intervals of at least 4 weeks to obtain a definite diagnosis of ECH.
Patients were further subdivided with respect to sex, age at onset, decade of onset, age at first visit to our Outpatient Department of Neurology and time interval from age at onset to first visit to our Outpatient Department. All data were assigned to consecutive 5- or 10-year periods between 1963 and 1997.
Statistics
To analyse differences in the female proportion of cluster headache sufferers between various subgroups, χ2 test of equality between proportions and Fisher's exact test for contingency tables were used. Normality of the age at onset data was tested. To analyse differences of the mean and the variance of the age at cluster headache onset, between the sexes and between subtypes of CH, one-tailed tests at the 5% significance level were used. Parametric and non-parametric (Wilcoxon's rank sum test) methods were used to test sex differences of the mean. The equality of variances between men and women was tested with the following statistic: F (n1−1, n2−1) = s1 2/s2 2 where n1 and n2 are the sample sizes, s1 2 and s2 2 the corresponding sample variances, and with the larger sample variance placed in the numerator. Version 6.12 of the SAS statistical package was used to process the data (21).
Results
The results are shown in Fig. 1 and Tables 1–4. General characteristics of the patient material are summarized in Table 1.
Characteristics of 554 cluster headache patients referred between 1963 and 1997∗

∗Patients referred to Huddinge University Hospital in 1997 (n = 5).
†The time between the year at onset and the year at first visit at our department.
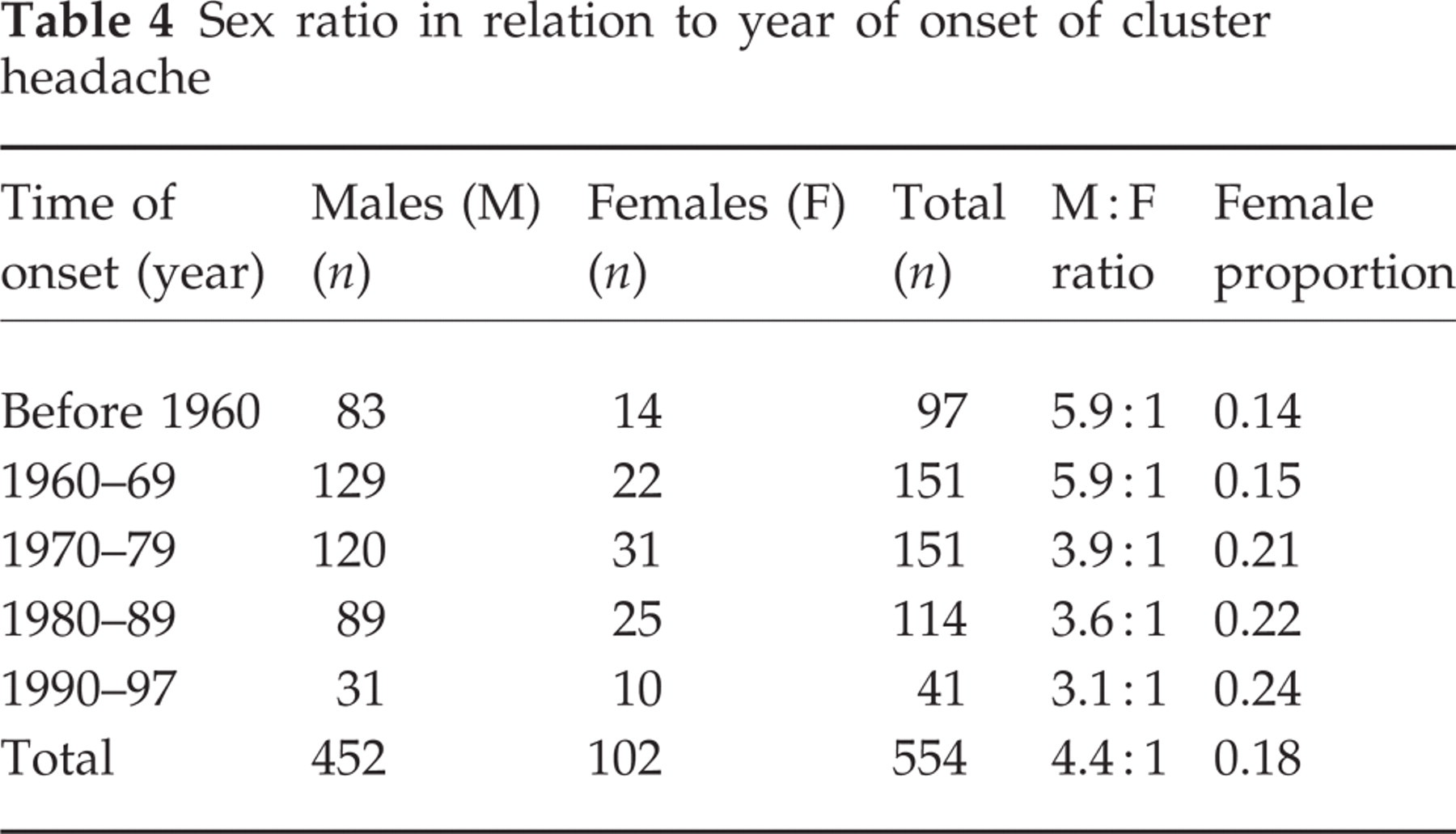
Sex ratio in relation to year of onset of cluster headache

Case material (n = 554). Distribution of sex and age at onset. male patients (n = 452), female patients (n = 102).
The study group comprized altogether 452 men (81.6%) and 102 women (18.4%). Age at onset, age at the first visit and time from onset to first visit were evaluated and compared decade by decade and there was no significant change over time with respect to these data. ECH occurred in 494 patients (89.2%) and CCH in 60 (10.8%). The ratio of ECH to CCH did not change over time. There were, however, no cases of CCH in women diagnosed before 1980. CCH was subdivided into primary (24 men and 5 women) and secondary CCH (25 men and 6 women).
Age at onset
The distribution of age at onset in the whole series of patients is presented in Fig. 1 and Table 2. The age at onset ranged from 10 to 68 years, with a peak between 20 and 29 years for both sexes. The frequency distribution of the age at onset for all CH was non-normal (P = 0.0001) and right skewed in males and in females, respectively. The mean age at onset did not differ between men and women but the variance was significantly larger in females than in males (Table 3). Onset of CH before age 50 was recorded in 85 out of 102 women (83.3%) and in 421 of 452 men (91.3%).
Sex, age at onset and male to female ratio in 494 patients with episodic and 60 patients with chronic cluster headache

The age at onset in 554 patients with cluster headache

Significant sex differences in: (a) the mean (P < 0.05; parametric and non-parametric tests) and (b) the variance of the age at onset (P < 0.05; parametric test). Significant difference in: (c) the mean of the age at onset between chronic and episodic forms of CH among females (P < 0.05; parametric test) and (d) the variance of the age at onset between chronic and episodic forms of CH among females (P < 0.05; parametric test).
In ECH the frequency distribution of age at onset exhibited similar characteristics as in the total group of CH, with an onset peak between 20 and 29 years of age (Tables 2 and 3). The mean age at onset did not differ between men and women but the variance was significantly larger in females than in males. In women there was also a slight increase in the number of new cases between 50 and 59 years of age.
In CCH (Tables 2 and 3) the frequency distribution with respect to age at onset was peaked for men, non-normal (P = 0.0270) and relatively symmetric. The onset was most frequent between 20 and 39 years of age. Only three of the 49 men (6%) with CCH had their onset after 50 and none after 60 years of age. In men the age at onset did not differ between ECH and CCH. Twenty-four men had primary CCH with a mean age at onset of 31.8 years (range 14–56) and 25 men had secondary CCH with a mean age at onset of 30.9 years (range 14–49). The age at onset did not differ significantly between the men with primary and secondary CCH.
In women with CCH the frequency distribution with respect to age at onset was flat and heavy tailed. There was no evidence to reject the null hypothesis of a normal age at onset distribution (P = 0.3259). In women the mean age at onset was significantly higher in CCH than in ECH (Table 3) and the distribution of the age at onset differed significantly between CCH and ECH (P = 0.02). Thus, six (7.1%) of 85 women with onset before age 50 had CCH compared with five of the 17 (29.4%) with onset after 50 (P < 0.01).
In a further analysis of the 11 female patients with CCH, five had the primary chronic variety and six had the secondary chronic variety. The primary chronic female patients displayed an onset ranging from 30 to 68 years with a mean of 50.8, whereas the secondary chronic females had an onset from 16 to 60 years with a mean of 35.5 years. However, this age difference was not statistically significant.
The mean and the variance of the age at onset for CCH was significantly larger in females than in males (Table 3). In primary CCH the mean age at onset was significantly larger in women than in men, whereas there was no significant sex difference with regard to the variance of the age at onset. In secondary CCH there was no significant sex difference of the mean age at onset, whereas the variance of the age at onset was significantly larger in women than in men.
Male to female ratio
The overall male to female ratio did not differ between ECH and CCH (Table 2).
The number of males and females with respect to age at onset is illustrated in Fig. 1 for the total material. The proportion of females shifted significantly with respect to age at onset (P = 0.002). The male to female sex ratio in relation to age at onset was 3.3 : 1 between 10 and 19 years, 4.8 : 1 between 20 and 29 years, 7.1 : 1 between 30 and 39 years, 8.4 : 1 between 40 and 49 years, 2.2 : 1 between 50 and 59 years and 1 : 1 between 60 and 69 years.
When subdividing the material into ECH and CCH the proportion of females still varied significantly with respect to age at onset (P < 0.02 and P = 0.004, respectively) (Table 2). The male to female ratio was largest in patients with an onset between 30 and 49 years (ECH 7.2 : 1; CCH 11.0 : 1) and lowest after 50 (ECH 2.3 : 1; CCH 0.6 : 1). In CCH it was as high as 14.0 : 1 in those with an onset between 30 and 39 years.
The number of new cases subdivided by year (decade) of onset is shown in Table 4. The male to female ratio was significantly higher before than after 1970 (P < 0.01) but the female proportion did not vary significantly between the onset decades (14–24%; P = 0.30). Pooling the present data with those published recently by Manzoni (2) showed, however, a significant increase in the female proportion over time when evaluated with respect to onset decade (n = 1036; P = 0.001).
During the whole inclusion period of 1963–97 the number of referrals to our clinics was relatively constant over time. The time from onset to first visit for both men and women averaged 9.9 years. The proportion of episodic to chronic CH did not differ significantly before 1970 compared with after 1970.
Discussion
Our main results show that the male to female ratio varied significantly with respect to age at onset, both in the episodic and chronic cluster headache. The male predominance was largest between 30 and 49 years of age but after the age of 50 the onset of cluster headache was as common in females as in males. In men with ECH and CCH and women with ECH there was an onset peak between 20 and 29 years. In women, particularly the chronic cases, there was a more even distribution of the age at onset across life and relatively more chronic cases after 50. The large variance of the age at onset in women has previously not been reported. In men there were no new cases of chronic CH after 60.
Contrary to reports by Kudrow (12) and Manzoni (5), the mean age at onset did not differ significantly between the chronic and the episodic form of CH in our series. When evaluating men and women separately, however, it was evident that CCH in women started later than in men and later than ECH in women. These results accord in part with those of Torelli et al. (22). They assumed that the second onset peak in their series was due to ECH evolving into the secondary variety of CCH. We found that almost 50% of the newly afflicted chronic females had their onset after 50 years of age, but the second peak in our series was mainly due to an increased number of new episodic cases. Female patients with secondary CCH had non-significantly lower mean age at onset than those who suffered from primary CCH. These observations may possibly speak against the hypothesis of Torelli et al. but our material is too small to allow any definite conclusions. We found no definite alterations over time in age at onset in the male patients, which agrees with the results of Manzoni (3).
Whatever the cause of cluster headache, our finding of an age-related difference as regards male and female morbidity is likely to be an important clue as to the pathogenesis of cluster headache. Which factors would affect the vulnerability to CH in young middle age more in men than in women? Which factors decrease the vulnerability to CH after 40 years of age? Why is the number of new patients equal between the sexes after 50? The apparent flat age at onset distribution of CCH in women is also intriguing but these data have to be interpreted with caution considering the small number of CCH females in this series. It is, however, tempting to speculate that the menstrual cycle or other endocrine factors may play a protective role against CCH in middle life in women.
In order to detect a possible decreasing male preponderance in cluster headache over the years we used two different methods of analysis, namely referring sex ratio (males : females) to year of onset of cluster headache, as did Manzoni, and to year of first visit of patients to our department. The inclusion period ranged over more than three decades, from 1963 to 1997. Utilizing both of these approaches we found a trend towards a reduced male to female ratio over the years. In our series the proportion of female patients having an onset before 1960, or between 1960 and 1969, was identical to the results presented by Manzoni (2). Patients with an onset of disease after 1970 displayed a somewhat decreased sex ratio but the changes in proportion of afflicted females over the years were not statistically significant in our own material. However, when pooling our data with those of Manzoni (2) a highly significant decrease in male preponderance was detected. The reason for this tendency to a change in gender ratio remains to be determined.
Is there a real decrease of the incidence of cluster headache among men, or is CH becoming more frequent in women? Manzoni seems to favour the latter view and our data may weakly support this assumption. From the late 1970s and onwards we recorded more female patients, especially those with chronic cluster headache, while there were no significant change in referrals of men with cluster headache.
Has there been any change over the years in the liability to diagnose female patients with recurring severe headaches as suffering from migraine instead of cluster headache? For many years cluster headache was regarded as a variant of migraine, one main reason being the presumed existence of intermediate forms with features of both disorders. It is well known that migraine is common in females, whereas, on the other hand, cluster headache has been known to be especially common in males, ever since the early reports by Horton (23, 24) and others (25–27). During recent decades patients suffering from cluster headache have been increasingly recognized. The literature on cluster headache has expanded considerably since the 1960s and we have got an increased knowledge of the clinical features, pathophysiology and treatment of the disease. It can therefore be discussed whether this has had any recent impact on detecting afflicted female subjects.
We made every effort to obtain a diagnosis, as correct as possible. All patients were personally examined, most of them were seen many times at the Outpatient Department and many were also directly observed during spontaneous or induced attacks. We did not include any patient who had experienced one period of headaches only (i.e. so called ‘cluster headache periodicity undetermined’, IHS 3.1.1). A few symptomatic cases have been reported in the literature with an underlying organic disease, e.g. a tumour or vascular malformation, and a diagnosis of primary headache may sometimes be somewhat uncertain. Our patient material therefore differs somewhat from that of Manzoni who included 38 patients (12 females) with a periodicity of headaches not being determined. To date there is one single clinical study that has detailed the characteristics and prognosis of this particular subgroup (28). A consecutive series of 60 outpatients was examined between 1981 and 1996 in relation to an assumed first period of cluster headache and it was shown at follow-up in 1998 that 13 (26.5%) still had had only one cluster period after a mean observation time of almost 9 years. It is interesting that only one of these patients was a female (7.7%).
Is our sample of cluster headache patients representative of the general population of cluster headache sufferers? Our investigation was clinically orientated and primarily aimed at comparing the total number of males and females with cluster headache having been referred to us during the years. We included patients both from the Stockholm County Council and outside this region. The small number of the latter patients (n = 16) displayed exactly the same sex ratio as the total patient material (13 male, 81.3%; 3 female, 18.7%) and there is no evident selection bias with respect to this particular recruiting procedure. Owing to the severity of pain there are reasons to believe that the majority of patients with cluster headache seek medical advice. A Danish study on living relatives of cluster headache sufferers showed that 92% (24 out of 26) at some time consulted a physician or a neurologist, or both, because of their cluster headaches (29). This is in contrast to migraine or tension-type headache, where patients display a much lower consultation rate. During the years we have had a close collaboration with primary care physicians and others who are referring to us patients with severe headache problems. By means of our repeated educational programmes and local medical agreements it has been fairly well-known that all CH patients should be seen by a neurologist and thus in turn preferably referred to us. Since 1972 we have mainly received our patients from the southern parts of Stockholm, with an estimated prevalence of barely 400 cluster headache patients living in the medical area of Söder Hospital. It can be roughly estimated that we have seen 90% or more of these sufferers.
Has there been any change in the referrals to our departments over the years? By way of comparison it can be mentioned that 1370 patients (698 males), excluding the acute cases, were referred to the Outpatient Department of Neurology at the Karolinska Hospital in the year 1968. Thirteen ‘new’ cases of cluster headache were detected among them, i.e. a relative frequency of 0.95%. The corresponding figures were remarkably similar for Söder Hospital. Among 2006 new referrals in 1993 we diagnosed 19 new cases of cluster headache, i.e. a relative frequency of 0.95%, and among 2165 new visits in 1994 we found 14 new cases, i.e. a frequency of 0.65%. In the present investigation we also tried to look for any changes in the rate of referrals over time. The number of ‘new’ cases was relatively constant for each 5-year period, which also suggests that no major change in the incidence or prevalence of cluster headache has occurred during the inclusion period. We believe that a significant selection bias, as seen from the aspects of a specialized headache unit, is of less importance in cluster headache than in other types of primary headaches.
Significant alterations in the lifestyle of both sexes over the past few decades have been suggested by Manzoni to affect the gender ratio (3, 4). It is well known that CH patients are heavy smokers. Levi et al. (30) compared the age at onset of smoking and the age of onset of ECH in a series of 53 consecutive male patients. Smoking was found to precede cluster headache by an average of 10 years, which may suggest that smoking is more than a secondary phenomenon. The same results have recently been reported by Torelli et al. (22), who found that a mean of 11 years elapsed between onset of smoking habits and onset of both episodic and chronic cluster headache. In a large case-control study Nappi et al. (31) have also clearly shown that smoking represents a significant risk factor for the disease.
In summary, we report that, although there is an overall male preponderance in cluster headache, the male to female ratio varies widely as a function of age at onset, both in episodic and in chronic cluster headache. The male preponderance with regard to onset of CH was most pronounced between 30 and 49 years of age and after 50 there were equal numbers of new male and female patients. The nature of the sex- and age-related pattern of cluster headache onset remains to be elucidated but sex-dependent endocrine and/or genetic regulatory mechanisms, possibly of hypothalamic origin, are likely to be involved. Although not statistically significant, there was also a tendency towards a decreasing male preponderance during the observation period of more than three decades. As the mean age at onset has not changed and the number of post-menopausal new female patients with chronic cluster headache is rather modest, there must be some other explanation for the decreasing male preponderance, which is most likely to be environmental and related to changes in lifestyle.
Footnotes
Acknowledgement
We would like to thank Dr Johan Träff MD for valuable help.