
Abstract
Large-conductance, calcium-activated potassium (maxi-K) channels regulate neurotransmitter release and neuronal excitability, and openers of these channels have been shown to be neuroprotective in models of cerebral ischemia. The authors evaluated the effects of postinjury systemic administration of the maxi-K channel opener, BMS-204352, on behavioral and histologic outcome after lateral fluid percussion (FP) traumatic brain injury (TBI) in the rat. Anesthetized Sprague-Dawley rats (n = 142) were subjected to moderate FP brain injury (n = 88) or surgery without injury (n = 54) and were randomized to receive a bolus of 0.1 mg/kg BMS-204352 (n = 26, injured; n = 18, sham), 0.03 mg/kg BMS-204352 (n = 25, injured; n = 18, sham), or 2% dimethyl sulfoxide (DMSO) in polyethylene glycol (vehicle, n = 27, injured; n = 18, sham) at 10 minutes postinjury. One group of rats was tested for memory retention (Morris water maze) at 42 hours postinjury, then killed for evaluation of regional cerebral edema. A second group of injured/sham rats was assessed for neurologic motor function from 48 hours to 2 weeks postinjury and cortical lesion area. Administration of 0.1 mg/kg BMS-204352 improved neurologic motor function at 1 and 2 weeks postinjury (P < 0.05) and reduced the extent of cerebral edema in the ipsilateral hippocampus, thalamus, and adjacent cortex (P < 0.05). Administration of 0.03 mg/kg BMS-204352 significantly reduced cerebral edema in the ipsilateral thalamus (P < 0.05). No effects on cognitive function or cortical tissue loss were observed with either dose. These results suggest that the novel maxi-K channel opener BMS-204352 may be selectively beneficial in the treatment of experimental TBI.
An estimated 1.5 to 2 million people in the United States suffer from a traumatic brain injury (TBI) each year. TBI is the leading cause of long-term disability among children and young adults (NIH Consensus Development Panel 1999). The lateral fluid percussion (FP) model of experimental brain injury in the rat is widely regarded as a reproducible, clinically relevant model of TBI. This model is known to produce cognitive and neuromotor impairments (McIntosh et al., 1989b; Pierce et al., 1998), as well as consistent clinically related patterns of cell dysfunction and death, including the formation of cerebral edema (Soares et al., 1992; Okiyama et al., 1995), cell loss in selectively vulnerable brain regions (Cortez et al., 1989; Toulmond et al., 1993; Dietrich et al., 1994; Hicks et al., 1996; Bramlett et al., 1997a,1997c), and tissue tears in the white matter (Graham et al., 2000; Bramlett et al., 1997b).
Similar to ischemic stroke, TBI results in a core of primarily injured tissue surrounded by an area of tissue at risk for secondary damage (the penumbra), as a result of an excessive release of neurotoxic excitatory amino acids (EAAs), membrane depolarization, and calcium influx (Shapira et al., 1989; Faden et al., 1989; Katayama et al., 1990; Nilsson et al., 1990). If left unchecked early in its progression, this cascade can lead to cell death, widespread edema, and expansion of the extent of injury. Several classes of compounds have been shown to ameliorate cellular damage and neurologic deficits, including cognitive decline and motor impairments, after experimental TBI. These include EAA antagonists, such as N-methyl-d-aspartate (NMDA) receptor antagonists (Hayes et al., 1988; Faden et al., 1989; McIntosh et al., 1990; Shapira et al., 1990; Smith et al., 1993; Okiyama et al., 1997,1998), and compounds that target calcium influx (Okiyama et al., 1992; Bodie et al., 1993; Cheney et al., 2000). However, many of these agents are associated with potential side effects and do not necessarily target those cells most at risk (Bullock, 1993; Maas, 2000).
Maxi-K (or BK) channels are large-conductance, calcium-activated potassium channels that are rapidly activated by depolarization and an increase in intracellular calcium (Latorre et al., 1989; Starrett et al., 1996; Gribkoff et al., 1997). When opened, they act quickly to restore membrane potential and reduce or block voltage-dependent calcium entry into the cell. Maxi-K channels are present in many brain regions, including the hippocampus, cortex, and various subcortical nuclei (Knaus et al., 1996), and have been found in many neuronal cell types, including hippocampal pyramidal cells (Yoshida et al., 1991), cortical neurons (Reinhart et al., 1989; Butler et al., 1993), cerebellar granule cells (Jalonen et al., 1990; Fagni et al., 1994), and sympathetic ganglia cells (Adams et al., 1982). These channels are believed to play an important part in neurotransmitter release through their control of intracellular calcium (Robitaille and Charlton, 1992).
Because of the demonstrable role of maxi-K channels in the regulation of intracellular calcium and membrane depolarization, newly synthesized openers of these channels afford an opportunity to target those cells most at risk after central nervous system (CNS) injury (that is, those that are exposed to potentially pathologic levels of intracellular calcium). Openers of these channels have been designed and synthesized, but their lack of specificity, or potency, or both, has made interpretation of results difficult at best (McKay et al., 1994; Strobaek et al., 1996; Gribkoff et al., 1997). BMS-204352 is a fluoro-oxindole BK channel opener with a high degree of potency and specificity at the maxi-K channel (Post-Munson et al., 2000; Starrett et al., 2000). This compound enters the brain at high levels after intravenous administration in rodents and has been shown to be experimentally effective in the treatment of acute stroke (Starrett et al., 2000). In an attempt to identify new therapeutic targets for the treatment of TBI, the authors evaluated the ability of BMS-204352 to attenuate neuromotor and cognitive deficits, the formation of regional cerebral edema, and cortical cell death associated with experimental TBI in rats.
MATERIALS AND METHODS
Surgical procedures and brain injury
Adult male Sprague-Dawley rats (n = 142) weighing 340 to 400 g were anesthetized (sodium pentobarbital, 60 mg/kg, intraperitoneally) and placed in a stereotaxic frame. The scalp and temporal muscle were reflected and a 5-mm craniotomy was made in the skull over the left hemisphere of the cortex between lambda and bregma. A modified plastic Luer-Lok cap was cemented over the craniotomy and filled with saline. For postinjury drug administration, the right femoral vein was exposed and the incision site was closed with a single suture before injury. Ninety minutes after anesthesia, a subset of the animals (n = 88) were attached to the FP device through the Luer-Lok fitting and subjected to lateral FP brain injury of moderate severity (2.6 to 2.8 atm) through the rapid delivery of a pressurized pulse of saline to the intact dura, as described previously (McIntosh et al., 1989b). The Luer-Lok cap then was removed and the skin was sutured. Sham animals (n = 54) received anesthesia and all surgical procedures, but did not undergo FP brain injury. Animals recovered after surgery/injury on heating pads to maintain normothermia.
Drug preparation and administration
Ten minutes postinjury, the single suture was removed and the right femoral vein was re-exposed for drug administration. Animals surviving surgery/injury (n = 132) were randomized to receive a bolus of one of the following treatments: 0.1 mg/kg BMS-204352 (high dose; injured, n = 26; sham, n = 18), 0.03 mg/kg BMS-204352 (low dose; injured, n = 25; sham, n = 18), or 2% dimethyl sulfoxide (DMSO) in polyethylene glycol (vehicle; injured, n = 27; sham, n = 18). The authors chose to evaluate two doses of BMS-204352 that previously have been shown to be efficacious in models of cerebral ischemia (Starrett et al., 2000).
Evaluation of cognitive function
One group of animals (n = 73) was tested at 42 hours after TBI/sham operation for cognitive memory deficits using a Morris water maze (MWM) and a previously described protocol (Smith et al., 1991). The maze consisted of a circular pool (1 meter in diameter) in which a fixed hidden platform was placed in 18°C to 20°C water. Before brain injury or sham surgery, animals (n = 84) underwent 2 days of training in the MWM, 10 trials a day, during which they learned to use external visual cues to find the submerged platform. Animals who met the learning criteria of an average latency to the platform of less than 12 seconds over the last 9 trials (n = 78 of 84) were anesthetized for surgery 90 minutes after the animal's last training trial. Forty-two hours postinjury/sham surgery, surviving animals (n = 73) were evaluated in the MWM for their ability to recall the previously learned task (memory test). Each animal was given 1 minute to swim in the maze with the platform removed while a computerized video system tracked its swim pattern. The MWM was divided into specified zones, mathematically weighted based upon their proximity to the location of the platform. A memory score was calculated for each animal by multiplying the amount of time spent in these zones by a weighting factor and summing the products according to a paradigm originally described by Smith et al. (1991).
Evaluation of regional cerebral edema
All animals were killed for evaluation of brain water content immediately after cognitive testing at 48 hours postinjury/surgery, because this time point has been shown to be the time at which edema is maximal after lateral FP brain injury (Soares et al., 1992). Animals were over-anesthetized (sodium pentobarbital, 200 mg/kg, intraperitoneally) and decapitated, and their brains were rapidly removed. At the occipito-parietal level, a 3-mm-thick coronal slice was cut from the brains, and both hemispheres were dissected on a cold plate into the following regions: (1) the parieto-temporal cortex (site of maximal cortical injury), (2) the parietal cortex (adjacent to site of maximal cortical injury), (3) the hippocampus, and (4) the thalamus (Fig. 1). Edema was determined by the wet weight/dry weight technique (Soares et al., 1992; Bareyre et al., 1997). Briefly, the fresh tissue was weighed on aluminum foil, dried for 24 hours at 100°C, then reweighed. Edema was defined as the percent of brain water content, as determined by the following equation: [(wet weight − dry weight)/wet weight] × 100.
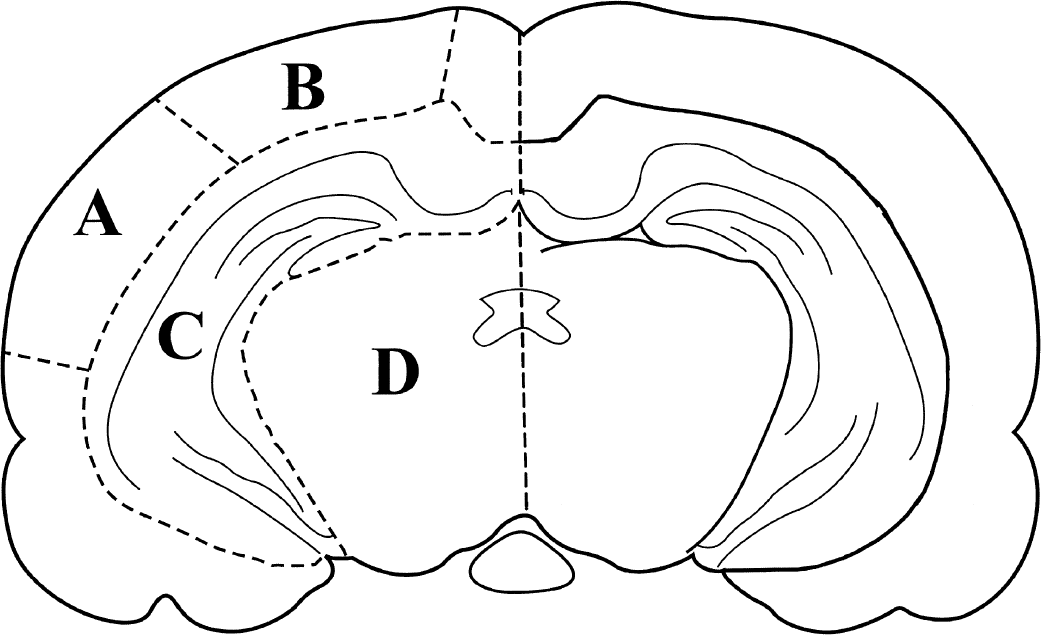
Schematic representation of a coronal section of rat brain illustrating the regions dissected for cerebral edema measurements: ipsilateral (A) parieto-temporal cortex, (B) parietal cortex, (C) hippocampus, and (D) thalamus. Hatched lines represent gross morphologic cuts made in the tissue. The same dissection was performed on the contralateral side.
Evaluation of neurologic motor function
Neurologic motor function was evaluated in a second group of animals (n = 59 of 64 surviving postinjury) at 48 hours, 1 week, and 2 weeks postinjury, using a previously described battery of tests (Saatman et al., 1997). All behavioral evaluations were performed by an experienced observer who was blinded to injury and treatment status. The composite of seven tests included: left and right forelimb flexion during suspension by the tail, left and right hindlimb flexion when the forelimbs remain on a surface and the hindlimbs are lifted up and back by the tail, the ability to resist left and right lateral pulsion, and the ability to stand on an inclined plane in the left, right, and vertical directions. Scoring was performed on an integer scale from 0 (severely impaired) to 4 (uninjured). Baseline evaluation of these tasks was performed 24 hours before injury. For the inclined plane tests, scores (0 to 4) were assigned in each direction based on the animal's performance at each time point relative to baseline performance. Then the 3 scores were averaged to be included in the composite motor function score (composite neuroscore), which included all 7 tests for a maximum score of 28.
Histopathologic evaluation of cortical lesion area
Immediately after the 2 weeks of neurologic motor testing, animals were over-anesthetized (sodium pentobarbital, 200 mg/kg, intraperitoneally) and transcardially perfused with 10% formalin. Brains were removed and postfixed in 10% formalin and then processed for paraffin embedding. In a subset of injured animals (vehicle, n = 8; 0.03 mg/kg, n = 7; 0.1 mg/kg, n = 7), a series of 6-μm coronal sections were cut on a rotary microtome at the levels of −3.3, −4.3, −5.3, and −6.3 mm bregma (Paxinos and Watson, 1990). One section at each level was stained with hematoxylin and eosin, and the area of the contralateral and ipsilateral cortices was then measured using a light microscope and image analysis system (MCID, Ontario, Canada), as previously described (Zhang et al., 1998). The cortex of both hemispheres was outlined by hand, by an evaluator blinded to injury and treatment status, and the total cortical area was calculated by the calibrated image analysis program. The lesion area then was calculated with the following formula: contralateral cortex - ipsilateral cortex.
Statistical analysis
Results of the neurologic motor tests are ordinal, nonparametric data and are presented as median values. A nonparametric Kruskal-Wallis analysis of variance (ANOVA) followed by individual Mann-Whitney U tests was used to evaluate these data. Memory scores and swim speeds in the MWM, regional cerebral edema, and lesion area are parametric data and were evaluated with a two-way ANOVA, followed by appropriate post hoc tests. These continuous variables are presented as mean ± SD. P < 0.05 was considered statistically significant.
RESULTS
Mortality
Ten of the 88 brain-injured animals died immediately after the injury, due primarily to respiratory arrest, resulting in an 11% injury mortality rate. These animals were not included in any data analysis.
Cognitive function
A highly significant cognitive deficit was observed in all brain-injured animals at 42 hours postinjury when compared with shams (P < 0.001) (Fig. 2). Among uninjured or injured animals treated with either dose of drug (0.03 mg/kg or 0.1 mg/kg) or with vehicle, no significant differences in MWM scores were observed, suggesting that BMS-204352 did not directly affect the cognitive ability of the sham or injured animals. Despite the nonsignificant decrease in memory scores seen in the sham high and low dose drug-treated animals, a slight trend toward improvement in cognitive function was observed in the brain-injured animals treated with low dose BMS-204352 (0.03 mg/kg). However, their scores were not statistically different from brain-injured, vehicle-treated animals.
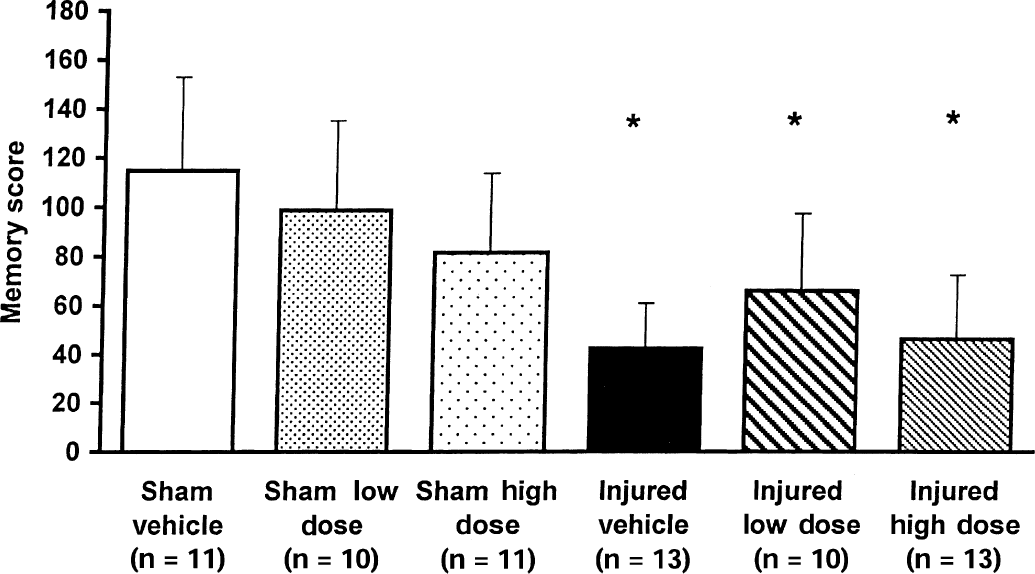
Memory scores of vehicle and low and high dose BMS-204352-treated animals tested in a Morris water maze at 42 hours after fluid percussion brain injury or sham surgery. *P < 0.001 when compared with sham animals. Bars represent mean for each group with standard deviation.
Swim speed also was calculated for each group during the MWM memory trial to assess motor function capability related to swimming. The mean speeds per group were as follows (cm/sec): sham vehicle = 58.6 ± 0.5; sham high dose = 58.5 ± 0.6; sham low dose = 58.4 ± 0.5; injured vehicle = 58.7 ± 0.6; injured high dose = 58.5 ± 1.3; and injured low dose = 58.7 ± 0.6. These speeds demonstrated that all animals had similar swimming abilities regardless of injury or treatment status.
Regional cerebral edema
Uninjured animals exhibited an average 79% water content in the hippocampus and cortical regions and 76% water content in the thalamus, values consistent with previously reported values for brain water content in uninjured Sprague-Dawley rats (Soares et al., 1992; Okiyama et al., 1995). By 48 hours postinjury, a significant increase in regional brain water content was observed in the ipsilateral injured and adjacent cortices and the ipsilateral hippocampus (P < 0.001), as well as in the ipsilateral thalamus (P < 0.01) in vehicle-treated, brain-injured animals (Fig. 3). Postinjury administration of high dose BMS-204352 (0.1 mg/kg) significantly reduced cerebral edema in the ipsilateral adjacent cortex (P < 0.05) (Fig. 3B), ipsilateral hippocampus (P < 0.05) (Fig. 3C), and the ipsilateral thalamus (P < 0.05) (Fig. 3D), whereas treatment with the lower dose (0.03 mg/kg) attenuated edema in the ipsilateral thalamus (P < 0.05) (Fig. 3D). No increase in edema was observed in any contralateral brain region in any of the injured groups, regardless of treatment (data not shown). However, a significant decrease in edema was observed in the contralateral adjacent cortex of brain-injured, low dose-treated animals (data not shown).
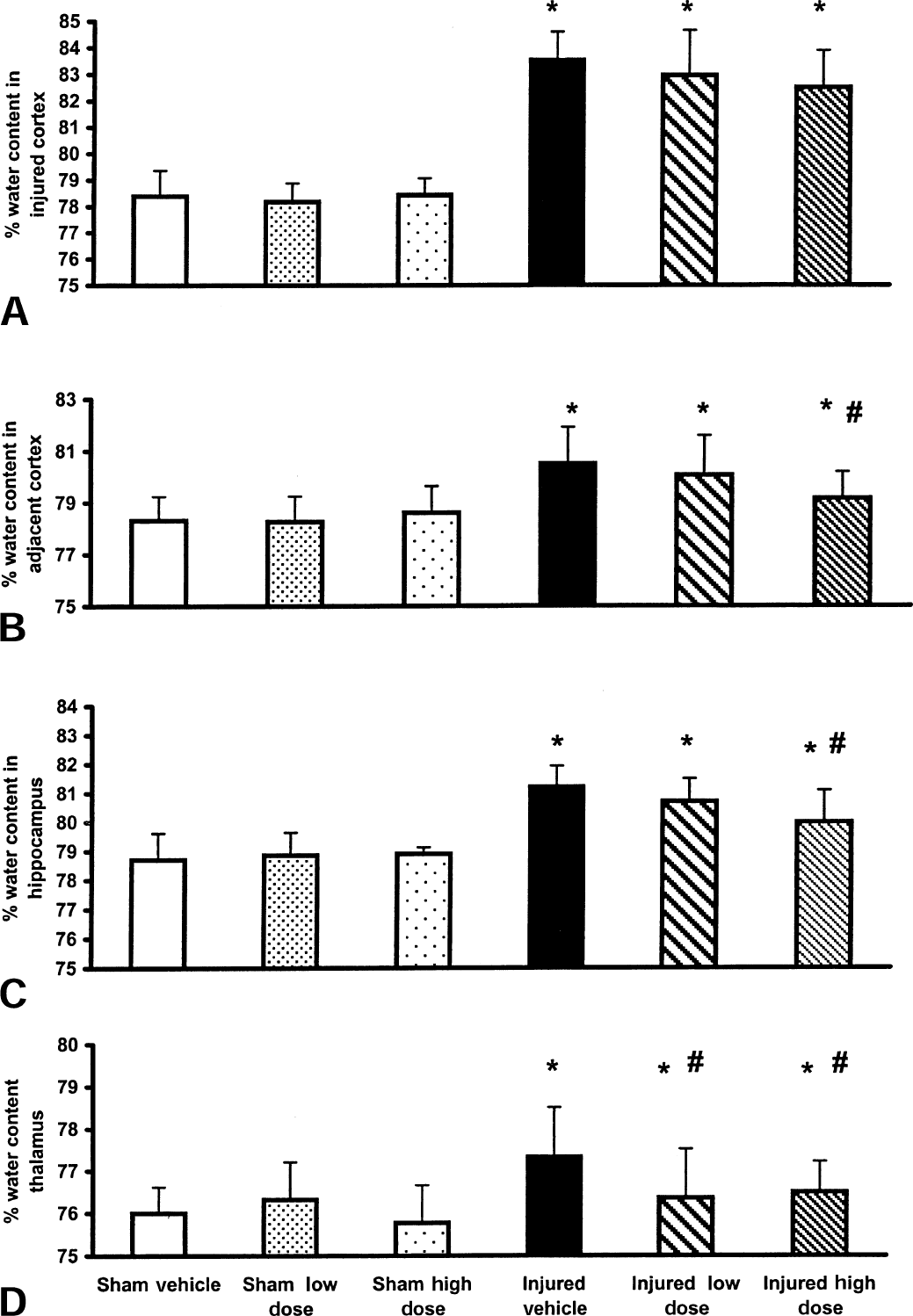
Regional cerebral edema measurements for the ipsilateral
Neurologic motor function
Compared with vehicle-treated sham (uninjured) animals, the neurologic motor function scores of the drug-treated uninjured animals was not significantly affected by either dose of BMS-204352 at 48 hours, 1 week, or 2 weeks postinjury. From 48 hours through 2 weeks postinjury, all brain-injured animals demonstrated significantly impaired neurologic motor function when compared with sham controls at each of the time points evaluated (P < 0.05) (Fig. 4). Postinjury administration of 0.1 mg/kg BMS-204352 significantly improved the composite neuroscore of brain-injured animals at 1 and 2 weeks postinjury when compared with brain-injured, vehicle-treated animals (P < 0.05, Fig. 4). No beneficial effects on neurologic motor function were observed after administration of 0.03 mg/kg BMS-204352.
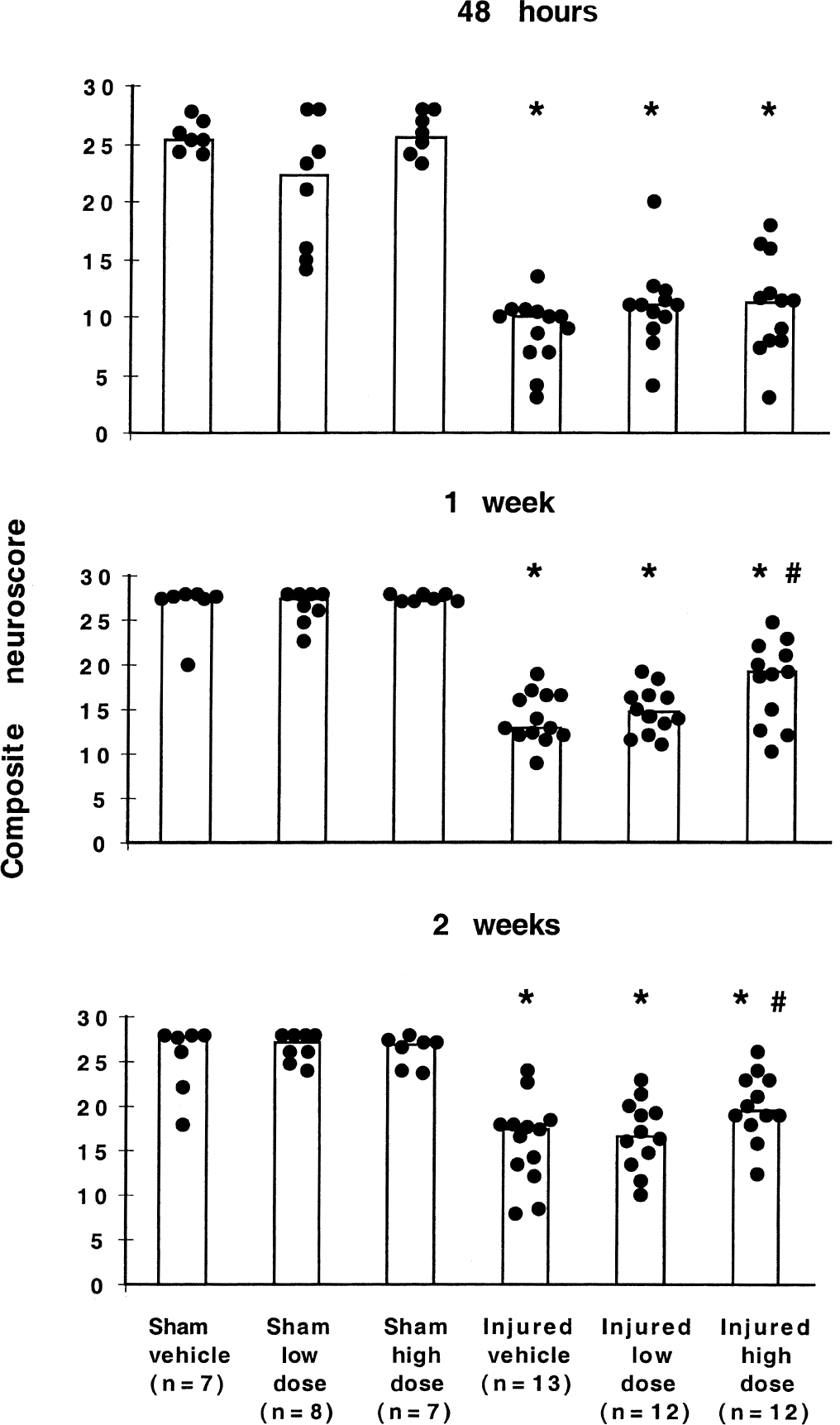
Assessment of neuromotor function in vehicle and low and high dose BMS-204352-treated animals at 48 hours, 1 week, and 2 weeks after fluid percussion brain injury or sham surgery. *P < 0.05 when compared with sham vehicle-treated animals. #P < 0.05 when compared with injured vehicle-treated animals. Bars represent median per group and circles represent the individual scores for each animal.
Histopathologic evaluation of cortical lesion area
By 2 weeks postinjury, a marked cortical lesion was observed in each of the tissue sections, from −3.3 mm to −6.3 mm bregma, in all brain-injured animals (Fig. 5). Postinjury administration of either dose of BMS-204352 did not significantly affect the size of the lesion area at any of the four rostrocaudal levels evaluated.
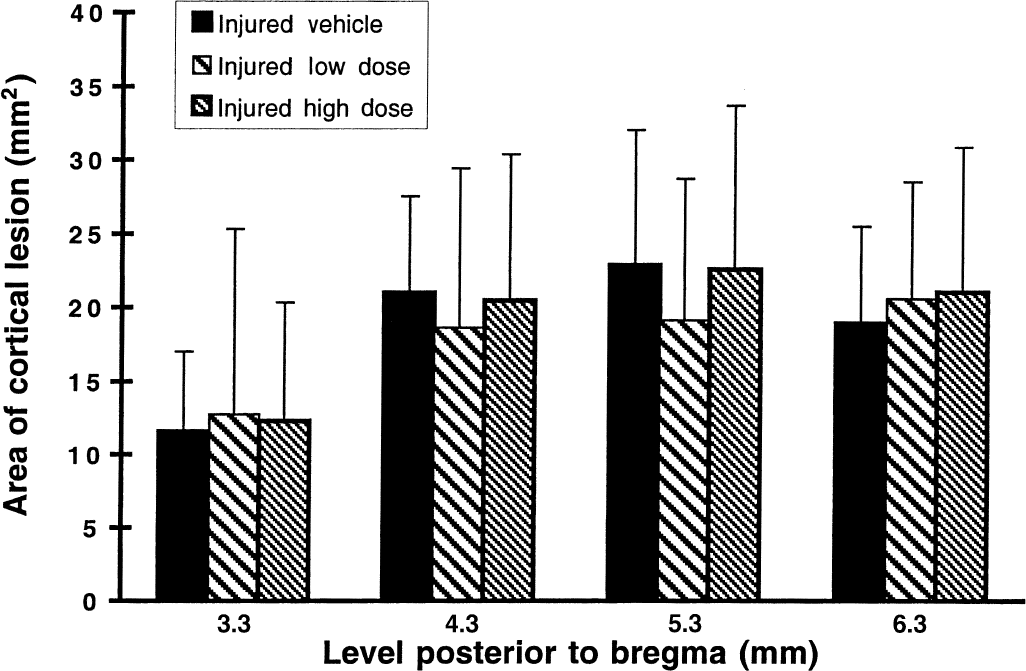
Cortical lesion area measured at 2 weeks postinjury in vehicle and low and high dose BMS-204352-treated animals. There were no significant differences observed among the three groups of injured animals at any of the four histologic levels analyzed. Bars represent mean for each group with standard deviation.
DISCUSSION
Acute, postinjury administration of the maxi-K channel opener BMS-204352 significantly attenuated regional cerebral edema formation at 48 hours and markedly improved neurologic motor function at 1 and 2 weeks after lateral FP brain injury in rats. No effects on posttraumatic cognitive dysfunction (at 42 hours) or cortical tissue loss (at 2 weeks) were observed. This is the first report regarding the ability of a maxi-K channel opener to improve neurobehavioral function and attenuate regional cerebral edema in an experimental model of head injury. The current results suggest that maxi-K channel openers, such as BMS-204352, may have a selective therapeutic benefit in the treatment of TBI.
In the current study, BMS-204352 at 0.1 mg/kg was shown to be effective in attenuating posttraumatic edema in the adjacent cortex, hippocampus, and thalamus of the ipsilateral hemisphere, whereas the lower dose was efficacious in reducing cerebral edema in the ipsilateral thalamus. These positive results regarding the attenuation of edema formation after TBI are similar to those reported previously with several of the noncompetitive NMDA glutamate receptor antagonists, such as MK801 (McIntosh et al., 1990; Shapira et al., 1990), kynurenate (Smith et al., 1993), and HU-211 (Shohami et al., 1993). Several other compounds that act on cation channels also have been successful in decreasing the formation of regional cerebral edema after experimental TBI, including the Ca2+ channel antagonist (S)-emopamil (Okiyama et al., 1992) and the use-dependent Na+ channel blockers, BW1003C87 (Okiyama et al., 1995) and Riluzole (Bareyre et al., 1997). The present beneficial effects of BMS-204352 on trauma-induced cerebral edema may be attributable to a reduction in membrane depolarization, EAA release, and intracellular calcium accumulation, all of which eventually can lead to an alteration in ion homeostasis with resulting cellular (cytotoxic) edema. The decrease in cerebral edema in the cortex and hippocampus of brain-injured animals treated with the high dose of BMS-204352 could be attributed to the large number of maxi-K channels in these brain regions (Knaus et al., 1996). The presence of these channels on the vasculature of smooth muscle cells also suggests the possibility that one component underlying this beneficial effect could be the compound acting on the cerebrovasculature (Gribkoff et al., 1997). The lack of a significant beneficial effect at the maximal site of injury in the ipsilateral cortex may be related to the fact that this site is associated with extensive hemorrhage and vasogenic edema (Soares et al., 1992), which may not be amenable to this type of pharmacotherapy.
Acute postinjury administration of 0.1 mg/kg BMS-204352 was also shown to improve neurologic motor function at 1 and 2 weeks after TBI. As with the effects on cerebral edema, the improvement in neuromotor function may also be a result of the ability of BMS-204352 to reduce EAA release and calcium accumulation. Other compounds that target these potentially deleterious posttraumatic cascades also have proven efficacious in attenuating motor function deficits after experimental TBI, including the NMDA antagonists kynurenate and indole-2-carboxylic acid (I2CA) (Smith et al., 1993) and MK-801 (Shapira et al., 1990; McIntosh et al., 1989a), (S)-emopamil (Okiyama et al., 1992), the free radical scavengers polyethylene glycol-conjugated superoxide dismutase (PEG-SOD) and lidocaine (Hamm et al., 1996), Riluzole (McIntosh et al., 1996; Wahl et al., 1997), the calpain inhibitor AK295 (Saatman et al., 1996), as well as the thyrotropin-releasing hormone analog, 2-ARA-53a (Faden et al., 1999). The reduction of cerebral edema at 48 hours also may have contributed functionally to the subsequent neuromotor recovery of the BMS-204352-treated, brain-injured animals at 1 and 2 weeks postinjury.
Although an attenuation of cell death has been previously observed after administration of BMS-204352 in a model of acute stroke (Starrett et al., 2000), a reduction in cortical tissue loss was not observed in the current study. The authors' evaluation of more chronic (2 weeks) histopathologic damage after an acute, single dose of the compound contrasts with the early (24 hours) neuroprotection observed in the ischemia model after BMS-204352 treatment at 2 hours postocclusion (Starrett et al., 2000). Perhaps evaluation of cellular damage at earlier time points may reveal similar benefits in the FP injury model. Considering the increasing cell and tissue loss that occurs after lateral FP brain injury (Smith et al., 1997; Bramlett et al., 1997b, c ; Pierce et al., 1998), multiple doses over the 2-week evaluation period may have greater therapeutic effects in the attenuation of this progressive cell and tissue loss.
Neither dose of BMS-204352 significantly influenced cognitive dysfunction in the acute (48 hours) postinjury period. Although a select number of compounds have proven beneficial in attenuating both cognitive and motor deficits (Okiyama et al., 1992; Smith et al., 1993; Gong et al., 1995; Saatman et al., 1996,1997; McIntosh et al., 1996; Faden et al., 1999), many other compounds have been shown to have a selective advantage in improving neurologic motor dysfunction without improving cognitive ability (Liu et al., 1994; Muir et al., 1995; Hamm et al., 1996; Cheney et al., 2000). It is possible that evaluation of memory function at a later time point after the injury may have revealed a positive effect of the drug, particularly because neuromotor improvement was not seen until 1 week postinjury. It is also plausible that the optimal dosages for improving motor and cognitive function are not identical.
In the current study, the authors demonstrated that a single bolus of BMS-204352 in the acute posttraumatic period could successfully reduce regional cerebral edema formation at 48 hours and improve neuromotor function at 1 and 2 weeks after lateral FP brain injury in the rat. These beneficial results, in a clinically relevant model of brain injury, are suggestive of the potential use of this maxi-K channel opener as a therapeutic agent for the treatment of TBI, and future studies should attempt to assess the therapeutic window for this compound. BMS-204352 currently is undergoing large-scale efficacy trials in patients with suspected acute cortical stroke and further evaluation in the treatment of TBI appears warranted.
Footnotes
Acknowledgments:
The authors thank Jeanne Marks for her assistance in the preparation of this manuscript and Hilaire J. Thompson for her help with data analysis.