
Abstract
Introduction:
Wandering spleen (WS) rarely occurs in clinical practice, with an incidence of 0.2% and a predominance in children <10 years old and in young girls. 1,2 When suspensory ligaments typically securing the spleen in the left upper quadrant (LUQ) are absent or display abnormal laxity, the spleen translocates within the abdominal cavity, and the attached splenic pedicle is predisposed to torsion. 1 To treat WS, splenopexy should be performed to save immunologic functioning when feasible. Safe and effective minimally invasive procedures for splenopexy have been reported and include mesh attachment to the abdominal wall (most common), creation of a retroperitoneal pouch, direct suturing to the abdominal wall/diaphragm, omental wrapping, and creation of a peritoneal flap. 2
Case Presentation:
A 12-year-old girl was referred to surgery clinic after presenting to her pediatrician with a suprapubic mass. Ultrasonography was performed and demonstrated the spleen in the midline lower pelvis with the tip abutting the dome of the bladder. There was also no spleen identified in the LUQ, consistent with a WS.
Materials and Methods:
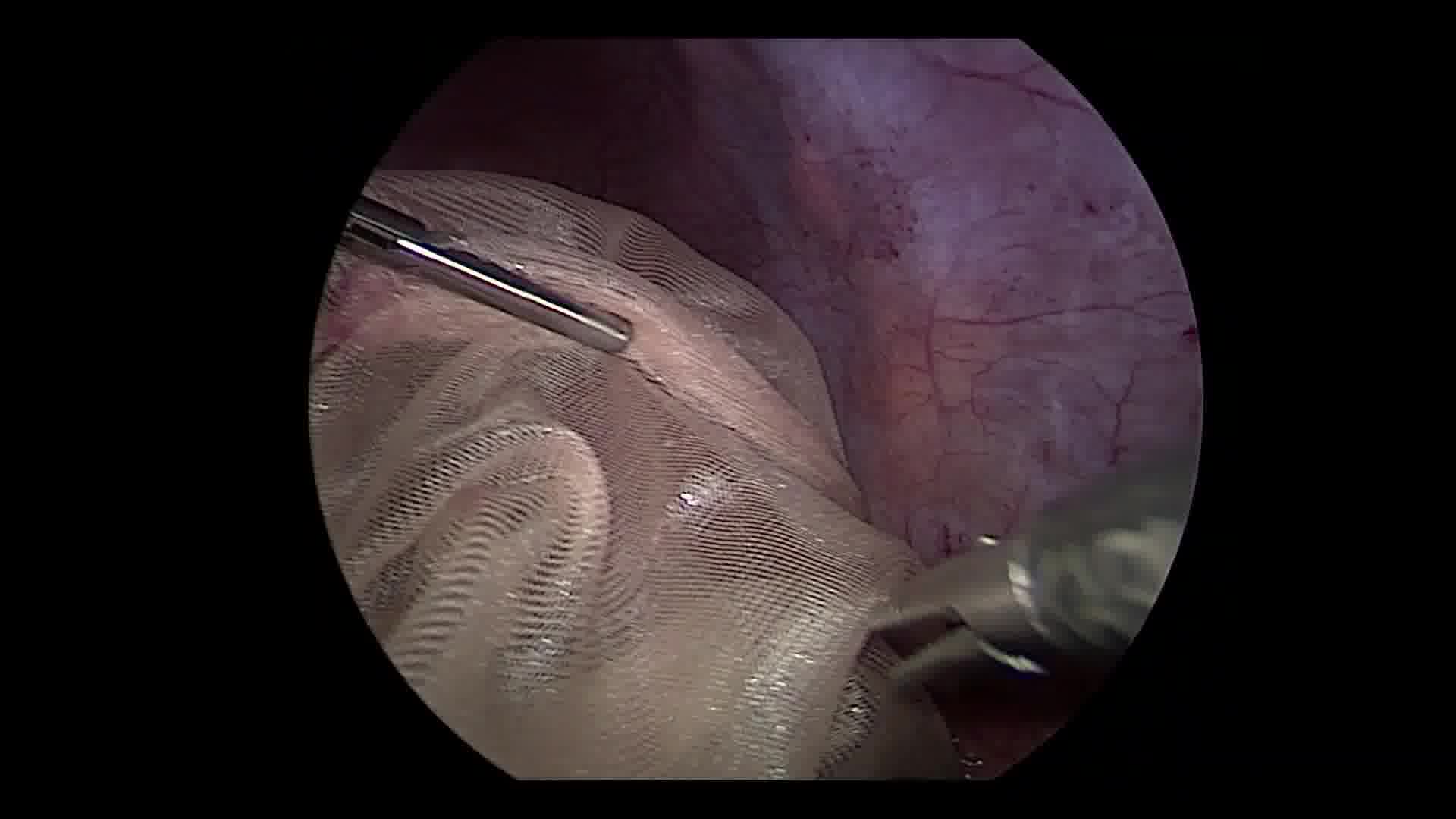
General anesthesia was administered, and the patient was positioned supine. After pneumoperitoneum was established with carbon dioxide insufflation, four laparoscopic ports were placed: a 10 mm infraumbilical trocar, two 5 mm trocars in the right upper quadrant, and one 5 mm trocar in the right lower quadrant. The abdomen was observed. The spleen was located in the pelvis, and the LUQ was void of a spleen, but all other anatomy was normal. There were no attachments to the spleen except for the vascular pedicle, which was not torsed; however, it was redundant with vessel engorgement, suggesting chronic obstruction. A slit was cut into a piece of Vicryl mesh, which was introduced into the peritoneal cavity, wrapped around the spleen, and clipped to itself to create a bag. The bag was moved into the LUQ, ensuring that the splenic pedicle did not torse. The Vicryl mesh was secured to the anterior abdominal wall using absorbable tacks. An omental overlay was then created and also tacked to the abdominal wall as a second layer.
Results:
Total operative time was 146 minutes. There were no intraoperative complications, conversion to an open procedure, and minimal blood loss. The patient's postoperative course was uncomplicated, and she was discharged home on postoperative day 1. At clinic follow-up 1 month later, she continued to recover appropriately, and the spleen remained in the LUQ, confirmed by palpation under the ribs with deep inspiration. She was advised to avoid excessive exertion for three additional weeks to allow for adequate scar tissue formation around the mesh-covered spleen, with surgical follow-up as needed.
Conclusions:
Laparoscopic splenopexy with mesh fixation to the LUQ abdominal wall is safe and feasible in a pediatric patient. However, one pitfall we encountered was the unsuccessful attempt to use a premade Vicryl bag to wrap the spleen. Instead, a slit was cut halfway into a sheet of Vicryl mesh and used to adequately wrap and secure the spleen.
Patient Consent Statement:
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure. Patient anonymity has been preserved, and personal information has been protected.
All authors have no disclosures to report. There are no competing financial interests that exist. All authors have no conflicts of interest to declare. The authors have no commercial associations or sources of support that might pose a conflict of interest. No conflicts of interest or obligations resulted from this study.
Funding:
No funding was received for this article.
Runtime of video:
5 mins 41 secs
Presented at the International Pediatric Endosurgery Groups 31st Annual Congress for Endosurgery in Children, June 1–3, 2022, Miami, FL.


Get full access to this article
View all access options for this article.