
Abstract
Wandering spleen is a condition that describes the movement of the spleen to an ectopic location inside the abdomen/pelvis as a result of weakened peritoneal ligaments. Wandering spleens are rare, with a less than 0.2% incidence being reported. Diagnosing a wandering spleen can be challenging because of the wide range of findings and the oftentimes vagueness of the patient’s symptoms. The most common ectopic location of the spleen is the left mid-abdomen. The most frequent treatment for wandering spleen includes splenopexy or splenectomy, depending on the complications associated with the condition.
A wandering spleen is an abnormal condition recognized by an increased mobility of the spleen. The ability of the spleen to reposition inside the abdomen is due to the absence, underdevelopment, or laxity of the suspensory ligaments required to fixate it to its normal position in the left upper quadrant. 1 The occurrence of a wandering spleen is rare, and its incidence has been reported to be less than 0.2%. 2 Nearly one-third of all cases of wandering spleen occur in young girls older than 1 year. In adults, women of childbearing age are more frequently affected as a result of acquired laxity of the splenic ligaments. 3
The vague symptoms associated with a wandering spleen often create a diagnostic challenge. In most cases, acute abdominal pain is the first presentation. Most often, laboratory tests do not reveal any definitive findings. Medical imaging modalities such as sonography and computed tomography (CT) are excellent techniques for imaging the spleen, but if the spleen returns to its normal position before a scan can be completed, the results will fail to diagnose the condition. 4 The treatment for a wandering spleen is splenopexy or splenectomy depending on the severity of the case and the viability of the organ. 5
Case Report
A 20-year-old woman presented to the emergency room with acute abdominal pain for the preceding 6 to 12 hours. The patient reported her other symptoms as chills, diaphoresis, shortness of breath, nausea, vomiting, back pain, and abdominal pain. During the physical examination, the nurse charted that the patient had tenderness in the right upper quadrant, epigastric pain, and a positive Murphy’s sign.
Abdominal sonography was performed to assess the right upper quadrant pain. The examination revealed an absence of the spleen in the left hypochondriac region of the abdomen. Upon further investigation by the sonographer, the spleen was identified in the right iliac region without any color Doppler filling (Figure 1). The sonographic images also identified air in the spleen (Figure 2) and liver (Figure 3), which affected the portal vein and splenic vein, respectively. Air in the biliary tree was suspected during sonography as well. The radiologist concluded that the images revealed a wandering spleen with a splenic infarct. A CT scan with contrast of the abdomen and pelvis was ordered to further evaluate the multiple abnormalities present. This protocol includes both oral contrast and intravenous contrast.
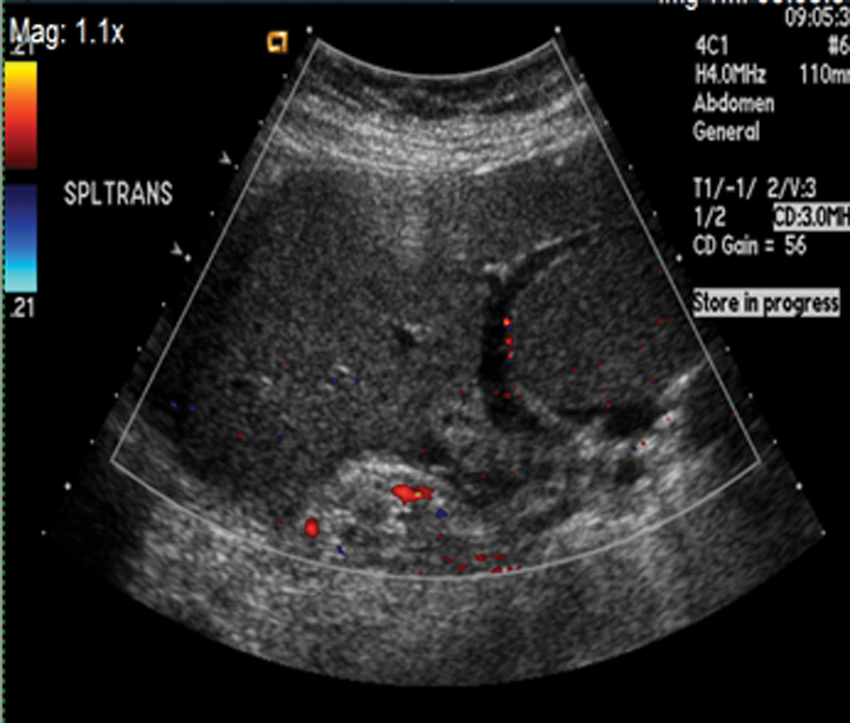
Image in the right lower quadrant showing the spleen in a transverse view, with no color Doppler filling noted.
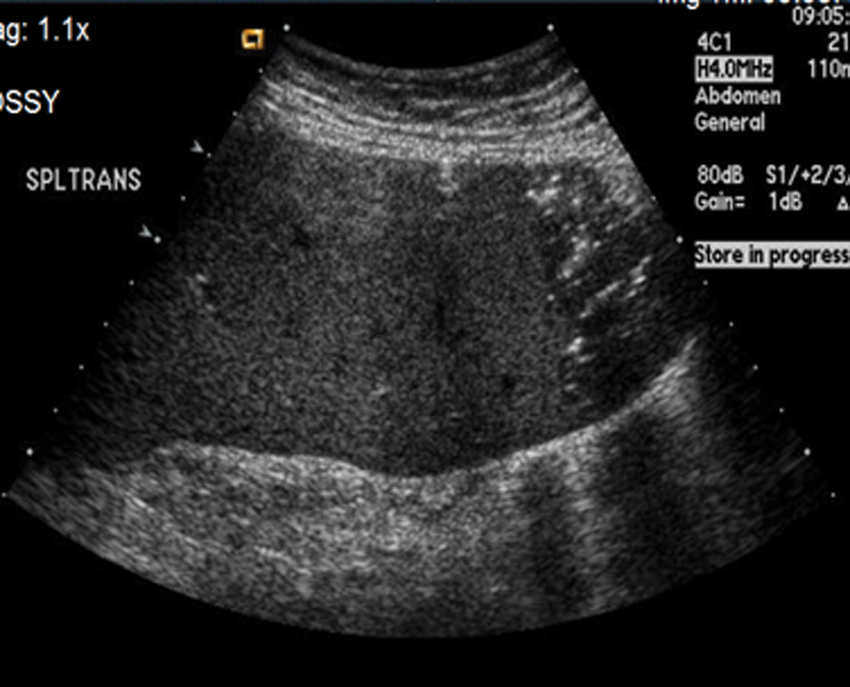
Transverse image in the right lower quadrant with characteristics of air in the spleen.
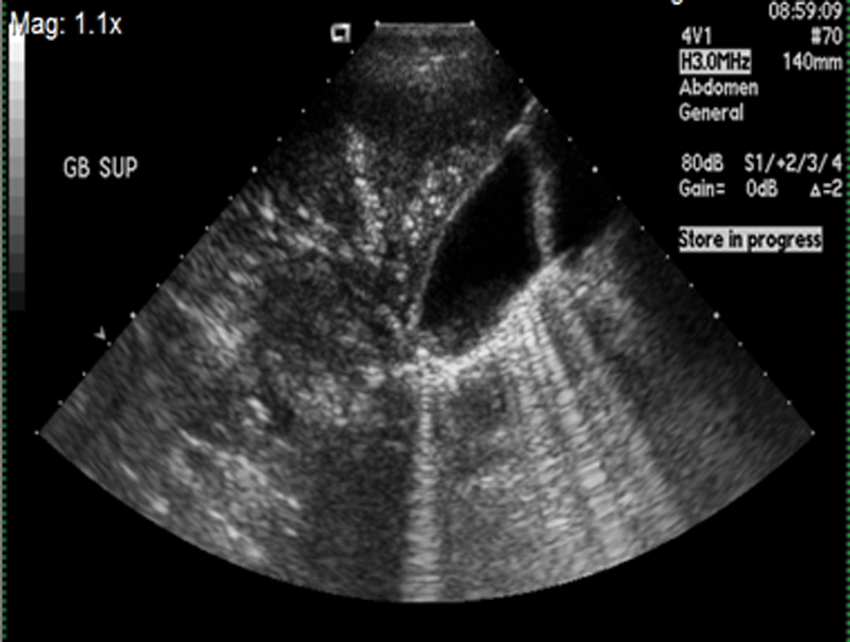
Longitudinal image in the right upper quadrant with characteristic signs of air in the liver and gallbladder wall.
A CT scan of the abdomen and pelvis using only intravenous contrast was performed since the patient could not tolerate oral contrast. The CT images revealed a dilated stomach with air and fluid present, pneumatosis of the gastric wall, and pneumoperitoneum (Figure 4). The images also confirmed the sonographic findings of air in the portal venous system throughout the liver and air in the spleen. Air in the peripheral branches of the superior mesenteric vein, inferior mesenteric vein, and systemic veins in the pelvis was also confirmed. The CT showed no evidence of air in the biliary tree. The CT scan also demonstrated a gastric volvulus, gastric outlet obstruction, and a compromised vascular pedicle of the stomach. The discovery of pneumatosis of the gastric wall and venous air raised suspicion for gastric ischemia resulting from the ectopic location of the spleen.
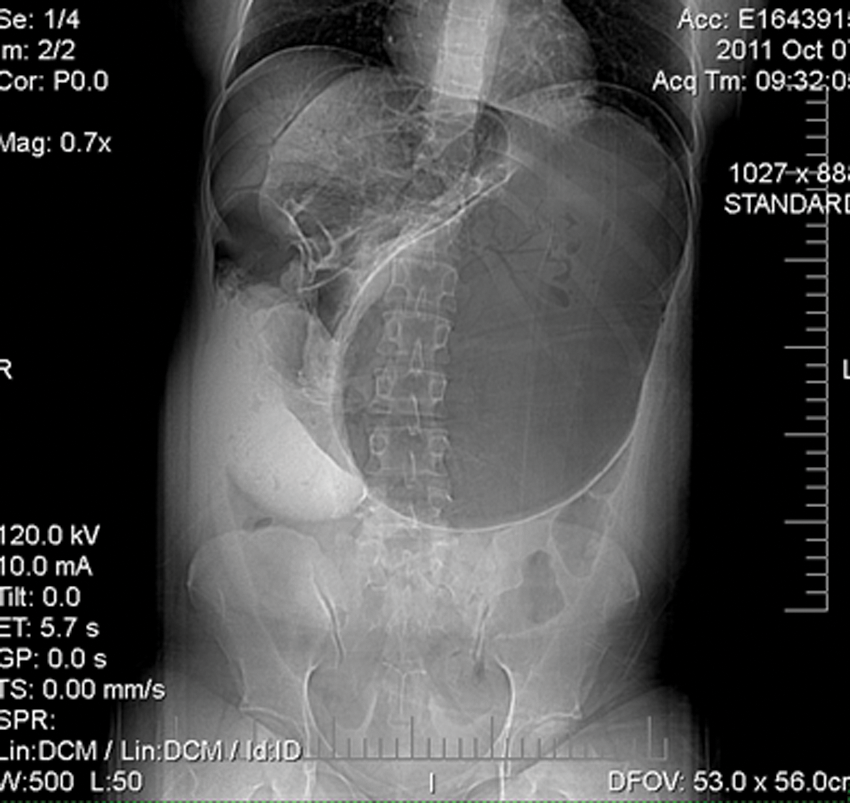
Computed tomography (CT) anterior-posterior scout image of the abdomen and pelvis showing the anatomic location of the liver, enlarged stomach, and wandering spleen.
The woman was admitted to the hospital and monitored overnight. Her symptoms worsened the first evening, and she was taken to the operating room the next morning. The surgeon performed an exploratory laparotomy, which once again confirmed the wandering spleen and gastric volvulus. He also discovered a gastric perforation, peritonitis, and evidence of sepsis as a result of the migration and complications related to the ectopic spleen. The surgeon then performed a subtotal gastrectomy with esophagogastrostomy and a splenectomy. The patient’s postoperative course was uneventful, and she was discharged from the hospital 10 days later.
The patient was referred for a follow-up CT scan of the abdomen and pelvis six months after her surgery. The examination documented normal postoperative changes and findings consistent with the patient’s history of pyelonephritis; no other abnormalities were seen.
Discussion
Wandering spleen is a condition that describes the mobility of the spleen with an ectopic location anywhere in the abdomen. 6 According to Sharath et al, 7 the left mid-abdomen is the most common location for an ectopic spleen. The challenge of diagnosing a wandering spleen is related to the clinical symptoms. Some patients may be asymptomatic, and a wandering spleen is detected accidently on a physical examination or accidently when imaging for another ailment. Some patients have mild intermittent abdominal pain. This would be due to splenic congestion with intermittent torsion and spontaneous detorsion. Patients may present with acute abdominal pain as a result of torsion of the splenic pedicle with subsequent infarction. Some patients may present with nausea, vomiting, fever, leukocytosis, and a palpable mass in the abdomen or pelvis.
Splenopexy is preferred in cases of wandering spleen with no torsion; however, splenectomy is the general treatment procedure in the presence of torsion, thrombosis of splenic vessels, secondarily developed hypersplenism, or infarction. 8 In our case study, a splenectomy was performed as a result of the severity of the complications from the wandering spleen.
Wandering spleen can be a difficult diagnosis, and the appropriate imaging study for diagnosis is debatable. Conventional radiography is of limited use. It may demonstrate bowel obstruction or soft tissue mass displacing bowel loops in the mid-abdomen. A CT scan can be a beneficial study revealing the wandering spleen, other abdominal organs, the peritoneal cavity, and with, use of contrast agents, splenic infarction. Computed tomography, however, is expensive compared with sonography, exposes the patient to ionizing radiation, and may subject the patient to allergic reactions from the contrast agent. Gray-scale sonography and power Doppler sonography are valuable in the diagnosis of wandering spleen and the torsion and infarction associated with this condition. Not only will it demonstrate the absence of the spleen in the left hypochondric region, but it will identify a homogeneous mass in the abdomen or pelvis consistent with that of the spleen. Use of power Doppler, color Doppler, and duplex sonography allows evaluation of blood flow in the splenic parenchyma and in the major splenic vessels. Sonography is performed quickly; is noninvasive, inexpensive, and nonionizing; and does not require any contrast agents. 9
Conclusion
A case of a wandering spleen is presented for which there is correlative imaging by CT and sonography. A search of the literature found no other reported cases of wandering spleen demonstrating gastric volvulus, gastric outlet obstruction, compromised vascular pedicle of the stomach, and pneumatosis of the gastric wall. These complications were attributed to the wandering spleen. Once the spleen was removed and repair made to the stomach and esophagus, the patient made a full recovery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.