
Abstract
Background:
Inguinal hernia is a common surgical disease and is defined as “giant” when descending below the midpoint of the inner thigh of a patient in upright position. These types of hernia are extremely rare and may still be encountered especially after years of self-neglect. 1,2 With the evolution of technology, minimally invasive surgery is the choice in a large number of interventions. The robotic approach has recently been increasingly used for hernia repair, mostly with the transabdominal preperitoneal hernia repair (TAPP). 3,4
Materials and Methods:
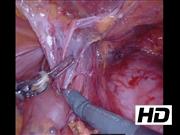
In our hospital between October 2019 and October 2020, three cases of giant inguinal hernia were performed. All of these are men, with a mean age of 69 years. The young patient had no comorbidities, the two elderly had hypertension and one also had cardiomyopathy associated with pacemakers implant and coronary stents, recurrent urinary infections, diabetes mellitus, and chronic renal failure. One patient had a body mass index > 30 kg/m2. Two of those had an ASA (American Society of Anesthesiologists) classification = 2, one patient had an ASA score of 3. Preoperative CT showed bladder and perivisceral fat content in all patients. The postoperative course was regular. All patients received antibiotics for the first 72 hours and were fully mobilized by postoperative day 1. Dysuria was reported in two patients experiencing inguinal “discomfort” and scrotal hematoma with drainage removed in the clinic after dimission. No late recurrences were diagnosed or any long-term complication observed. There was an improvement in the post-operative quality of life (QoL). In particular, the patient with recurrent urinary infections resolved this pathological condition. Another one with stranguria regained normal urinary function. Finally, in all three cases the pain in the inguinal region is resolved. This video describes the challenging reparation of a right giant inguinal–scrotal hernia containing bowel loops and urinary bladder in an 80 year-old man. The patient had longer than 10 years history of this hernia of ∼20 cm in size, causing pain, pollakiuria, voiding dysfunction, thickened scrotal skin, and influencing the QoL. The CT scan shows the bladder in the hernial sac. The forward traction of the bladder caused a compression on the distal ureteral tracts, showing a fair dilation of the right ureter and a hydroureteronephrosis on the left ureter. A left inguinal hernia is also present.
Results:
Hernias repairs are approached by TAPP with Stoppa's technique. In particular, the video shows the use of a polypropylene 22 × 18 cm mesh fixed by a few loose sutures and fibrin glue covering both hernia ports. In any hernia but especially in large hernias, we believe that the preperitoneal atraumatic dissection of peritoneal flap is very important. 5,6
Conclusion:
Giant inguinal hernia is a rare variant of inguinal hernia. Its clinical and instrumental classification is important and patient comorbidities must be taken into account. Appropriate patients selection is important in limiting complications and satisfactory prognosis. 1,2,7 The robotic TAPP is a technique that seems a safe, feasible, and reproducible approach. 3
Authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
No competing financial interests exist.
Runtime of video: 6 mins 51 secs


Get full access to this article
View all access options for this article.