
Abstract
Introduction:
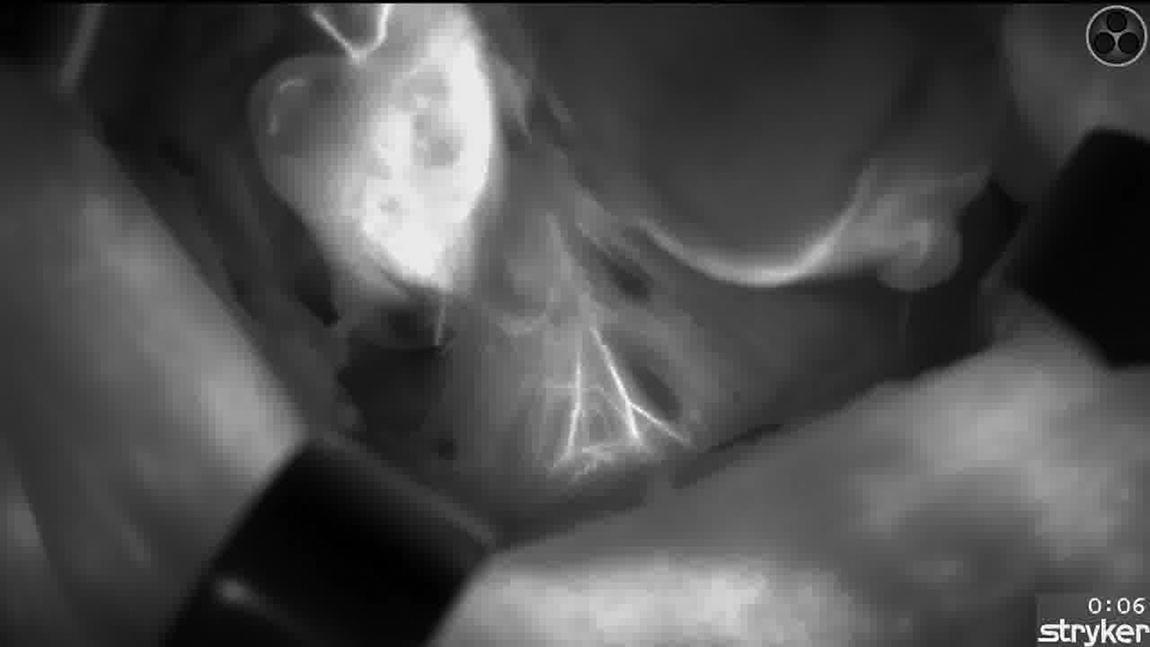
ICG angiography allows for visualization of the parathyroid gland’s feeding vessels by enhancing their vascular map, as well as to evaluate their viability. Parathyroid gland vessel identification and its preservation using ICG angiography-guided thyroidectomy have proven to aid in maintaining parathyroid function and reducing transitory and permanent hypocalcaemia. 1 Preservation of inferior parathyroid glands’ vascularization during thyroidectomy is difficult due to their position, as they often have long pedicles, and especially for the right inferior parathyroid gland, as its feeding vessel can be intertwined with the recurrent laryngeal nerve. Furthermore, it may become especially challenging when their vessels are subcapsular.
Materials and Methods:
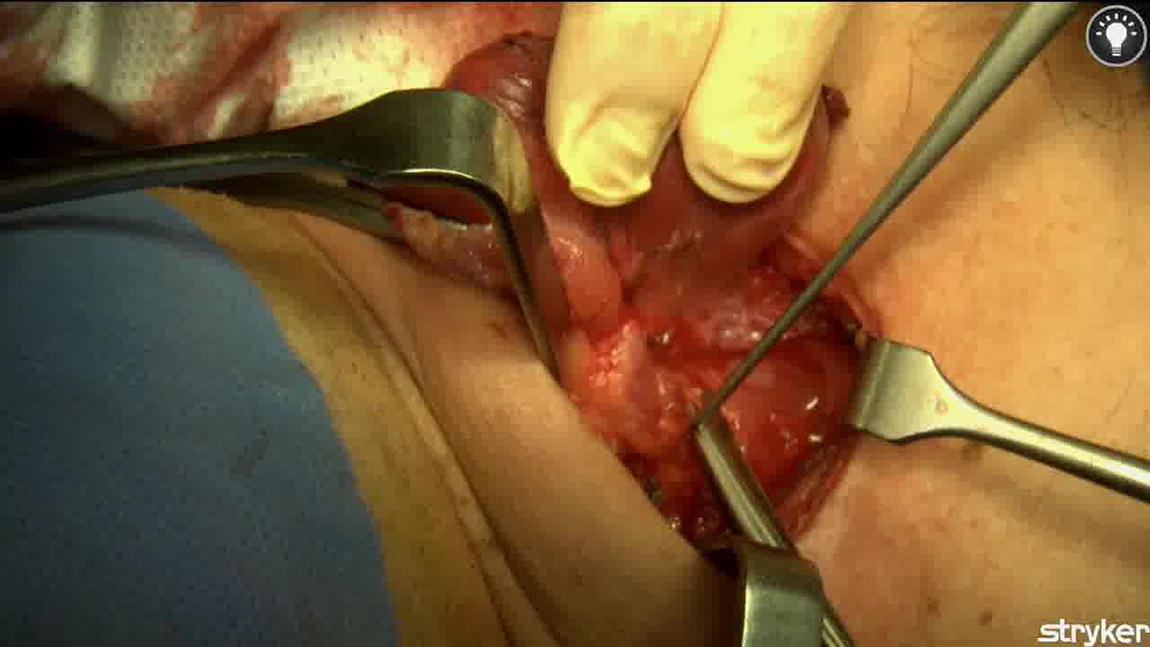
We present the video of a right lobectomy, focusing on the angiography-guided dissection of the inferior parathyroid gland with its vascularization in a subcapsular position. We use our described technique of ICG angiography guided thyroidectomy 2 in order to identify vascularization of the parathyroid glands before starting dissection of the right lobe. We administer 1 mL of a diluted solution of 25 mg of ICG and 10 mL of bidistilled water intravenously. After 10–30 seconds, we are able to identify a well-perfused right inferior parathyroid gland and a main identifiable feeding vessel with a defined pattern of vascularization. In this case, the right superior gland shows no perfusion with ICG angiography, and, therefore, we are not able to identify the gland’s feeding vessel before starting dissection. Visualization of the vessels with ICG also permits the use of high-energy devices with safety, as we are able to maintain the distance of thermal injury. Identification of the recurrent laryngeal nerve is an important step in preserving the inferior parathyroid gland’s vascularization. 2 Cranial dissection of the nerve until its intersection with the branches of the inferior thyroid artery allows for their better dissection and preservation on the right side. Visualization of the vessels with ICG also permits the use of high-energy devices with safety, as we are able to maintain the distance of thermal injury. Repeated doses of ICG may help in the dissection of the gland’s feeding vessel as it is often intertwined with the laryngeal nerve. Preserving the inferior parathyroid gland is especially challenging due to its long pedicle and its close relation with the laryngeal nerve and the branches of the inferior thyroid artery. We perform a careful dissection of the previously identified feeding vessel caudally from the exact point where the branch originates from the inferior thyroid artery, following its path to the inferior gland.
Results:
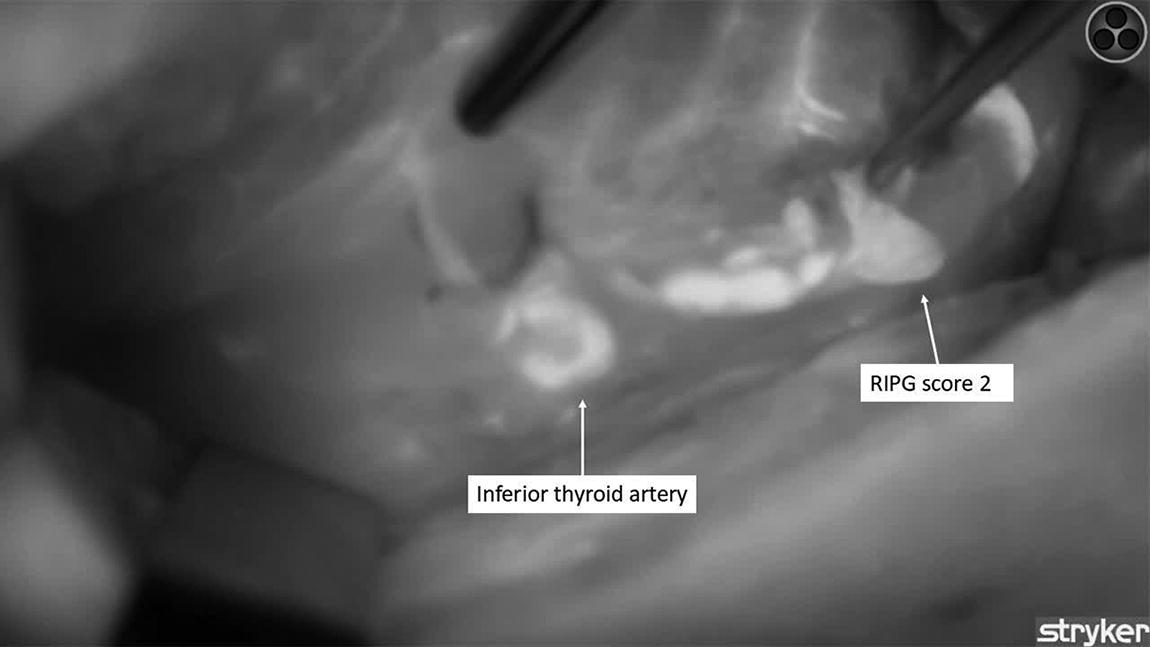
After lobectomy is completed, we perform ICG angiography showing no ICG uptake in the superior gland, while the inferior gland shows an intact vascularization and degree of perfusion than before starting dissection, maintaining a score of 2. As stated in our previously published articles, one well-perfused parathyroid gland is enough to predict normal function and therefore normal blood calcium levels. 3
Conclusions:
With this technique, we propose a paradigm shift in thyroidectomy by beginning with the identification of the parathyroid glands and their vascular map using ICG before lobectomy.
Disclosure Statement:
No competing financial interests exist for none of the authors of this abstract. Representation of any instrumentation does not indicate an endorsement of the product and/or company by the publisher, the American Thyroid Association, or the authors.
Author Disclosure Statement:
P Moreno Llorente is a KOL for J&J. NO disclosures.
Authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
Runtime of video: 4:11 mins
Get full access to this article
View all access options for this article.