
Abstract
Abstract
Background:
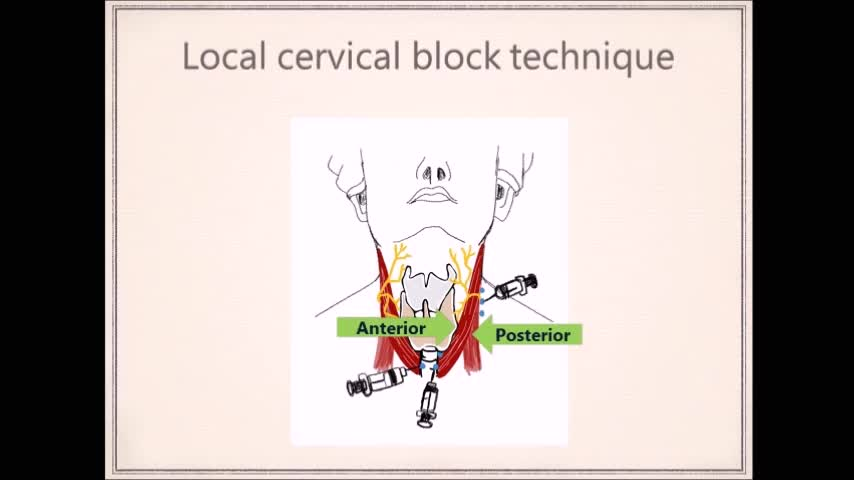
Renal hyperparathyroidism (rHPT) is an endocrine disease that is caused by the hyperfunctioning of the parathyroid glands. Medical treatment is the first option but can be ineffective in some cases. A total or subtotal parathyroidectomy is the standard treatment for patients who have not responded to medication. For example, hypercalcemia, parathyroid hormone (PTH) level >800 pg/mL, intractable bone pain, advanced osteopenia, calcinosis, calciphylaxis, or pruritus.1,2 A general anesthesia is a conventional option in total/subtotal parathyroidectomy, but end-stage renal disease patients may run a higher risk from anesthetic drugs. We have found that a local cervical block can reduce the possibility of cardiovascular or respiratory complications, which could occur with general anesthesia. The local cervical block is currently in use for open thyroidectomy and minimally invasive parathyroidectomy in parathyroid adenoma cases.3–6 The open total/subtotal parathyroidectomy may also be performed under a local cervical block anesthesia, with excellent curative rates.
Methods:
This video shows a detailed procedure of an open total parathyroidectomy with autotransplantation, using the local cervical block technique.
Results:
The diagnosis of rHPT is established by biochemical analysis. The indications that surgery is required are intractable bone pain, osteopenia, elevated PTH level = 1955 pg/mL (15–65), and elevated calcium level = 12.7 mg/dL (8.6–10.2). The patient is placed in the semi-Fowler position. A local cervical block anesthesia is performed by the surgeon, using 1% lidocaine hydrochloride 1% and epinephrine 1:100,000 injection. The Kocher incision is made, the subplatysmal flaps are elevated superiorly, and the median raphe is opened. The parathyroid glands are individually resected without recurrent laryngeal nerve injury and confirmed by frozen section. The intraoperative parathyroid hormone level 15 minutes after four glands were removed was 205 pg/mL (15–65). The operative time was 155 minutes with 10 mL blood loss. The length of hospital stay was 32 hours. The final pathology report showed all four parathyroid hyperplasias. Postoperative PTH level at day 30 was 42 pg/mL (15–65) and corrected calcium was 9.2 mg/dL (8.6–10.2). There were no intraoperative or any postoperative complications (hoarseness, hematoma, seroma, or infection) in this patient.
Conclusions:
A total/subtotal parathyroidectomy using the local cervical block technique is feasible and safe in this end-stage renal disease patient. In addition, we are able to assess the patients' voice intraoperatively. This procedure could be an alternative in parathyroidectomy candidates with less chance of anesthetic complications.
No competing financial interests exist.
Runtime of video: 6 mins 16 secs

Keywords
Get full access to this article
View all access options for this article.