
Abstract
Mental health literacy is defined as ‘the knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ [1], p.182]. The mental health literacy of the Australian population has been found to be quite limited, with many members of the public being unable to correctly identify mental disorders and common treatments [1–4]. A 1997 study reported that 39% of Australian adults could accurately identify the symptoms of depression from a vignette. Correct identification of schizophrenia was lower at 27% [1].
Poor mental health literacy may impede early recognition of symptoms in the self and others [1]. This in turn may delay help seeking [4, 5]. Help-seeking behaviour may also be influenced by the lack of awareness of availability of mental health services, the types of professionals on hand for support and treatment options [1]. The ability of young people to articulate problems to health practitioners may also be hindered by a lack of knowledge about mental illness [5].
Gender is one factor that may influence mental health literacy. Gender differences in physical and mental health occur with respect to illness incidence, prognosis, morbidity and mortality [6-8]. Differences have also been found with respect to perceptions and awareness of illness. In general, women have more diffuse views of illness and tend to be more aware of symptoms than men. Men tend to be unaware of health problems and are more likely to delay seeking help [7, 9].
Gender differences in knowledge and attitudes towards mental illness have been documented in a small number of studies [4,10-12]. As demonstrated in a recent study with 202 young Australians (15-17 years), males demonstrated poorer mental health literacy than females with respect to depression [4]. Male secondary students in Hong Kong have been found to have more stereotyping, restrictive, cynical and stigmatizing attitudes towards mental illness whereas female students displayed more benevolence [12]. Gender differences in stigmatizing attitudes towards mental illness have also been reported elsewhere. A study of 5025 German adults examined the relationship between emotional reactions to mental illness (i.e. schizophrenia and major depression) and illness beliefs [11]. Females were more likely to react to a vignette depicting mental illness with pity and fear, and were less likely than males to respond with anger [11]. It is unclear whether these gender differences in emotional reactivity relate to differences between males and females with respect to illness knowledge and awareness. Research into whether there are gender differences in knowledge and beliefs about mental illness is sparse, particularly among young people. Thus, the purpose of the present paper is to examine gender differences in mental health literacy using data from a survey of young Australians aged between 12 and 25 years [13]. It was hypothesized that males and females would differ in their knowledge and beliefs about mental illness.
Method
Participants
A total of 1207 young Australians (539 males, 668 females) aged between 12 and 25 (M = 17.75, SD = 3.79) years were recruited from four regions in Victoria, Australia [13].
Sampling techniques
The sampling frame was derived from a CD-ROM containing white pages listings of private household telephone numbers in the four regions. Households were randomly selected, and the most recent birthday method used to select respondents from households with more than one eligible member. The sample was stratified by age group (12-14, 15-17 and 18-25 years) and region. Once eligibility of a household was ascertained (i.e. young people within the defined age range) verbal consent was obtained either from the young people (18 years and over) or their parent or guardian (12-17 years old).
Measure
Each young person completed a 17 minute telephone survey adapted from Jorm et al.'s [1] Mental Health Literacy Questionnaire. The questionnaire was slightly modified to ensure suitability for administration by telephone interview and to ensure the questions were age-appropriate. This revised tool was successfully piloted with 40 respondents.
Each respondent was randomly presented with one of four vignettes, differentiated on the basis of mental illness (depression vs psychosis) and gender of the character (John vs Mary) (see Table 1 for the description of the two vignettes). The symptoms described in the two vignettes met both ICD-10 [14] and DSM-IV [15] minimum diagnostic criteria for psychosis (schizophrenia) or depression [13].
After being read the vignette, respondents were then asked the two following open-ended questions ‘What, if anything, do you think is wrong with John/Mary?’ (problem recognition) and ‘How do you think John/Mary could best be helped?’ (best form of help). Coding of responses to the open-ended questions was based on a content analysis undertaken on the same questions in a previous study [1]. This procedure was adopted to facilitate comparisons across studies. Twenty-six categories were derived for the problem recognition question and 13 were generated for the best form of help question. Correct responses for the problem recognition question were either ‘depression’ or ‘schizophrenia’ or ‘psychosis’ for the respective vignettes. Further information about the coding of these variables is detailed elsewhere [13].
Respondents were also read a list of pharmacological and psychological treatments and were asked rate each treatment according to whether it would be ‘helpful’, ‘harmful’ or ‘make no difference’ to the character in the vignette (closed-ended questions). They were also asked to estimate the prevalence of mental illness in young people in Australia by selecting from one of five options including: (i) one in every 1000 people (not common at all); (ii) one in every 100 people (slightly common); (iii) one in every 10 people (moderately common); (iv) one in every four people (very common); and (v) not sure/do not know.
Procedure
Data were collected during March-July 2001 by a consulting group with experience in large health surveys using Computer-Assisted Telephone Interviewing (CATI). Further details of the methodology can be found in Wright et al.'s study [13].
Depression and psychosis vignettes used in the telephone interview
Data analysis
The chi-square test (χ2) was employed to compare gender differences in recognition of depression/psychosis. Analyses were also conducted to compare responses between two age groups 12-17 years and 18-25 years. Fisher's exact test was used as an alternative to chi-square when expected frequencies were less than 5. When appropriate, signif icant chi-square results were followed by examination of standardized residuals to determine which cells contributed to the significant finding [16]. Alpha (a) or type I error was set at the 0.05 level.
Results
Recognition of depression versus psychosis
Overall, female respondents were significantly more familiar with depression (60.7%, n = 199, N = 328) than they were with psychosis1 (27.9%, n = 95, N = 340), χ2(1) = 72.58, p < 0.001 (see Fig. 1). This finding was replicated in both the 12-17 years (χ2 (1) = 43.86, p < 0.001) and 18-25 years (χ2 (1) = 32.89, p < 0.001) age groups.
Gender differences in the recognition of (▪)depression and (□) psychosis as depicted in the vignette.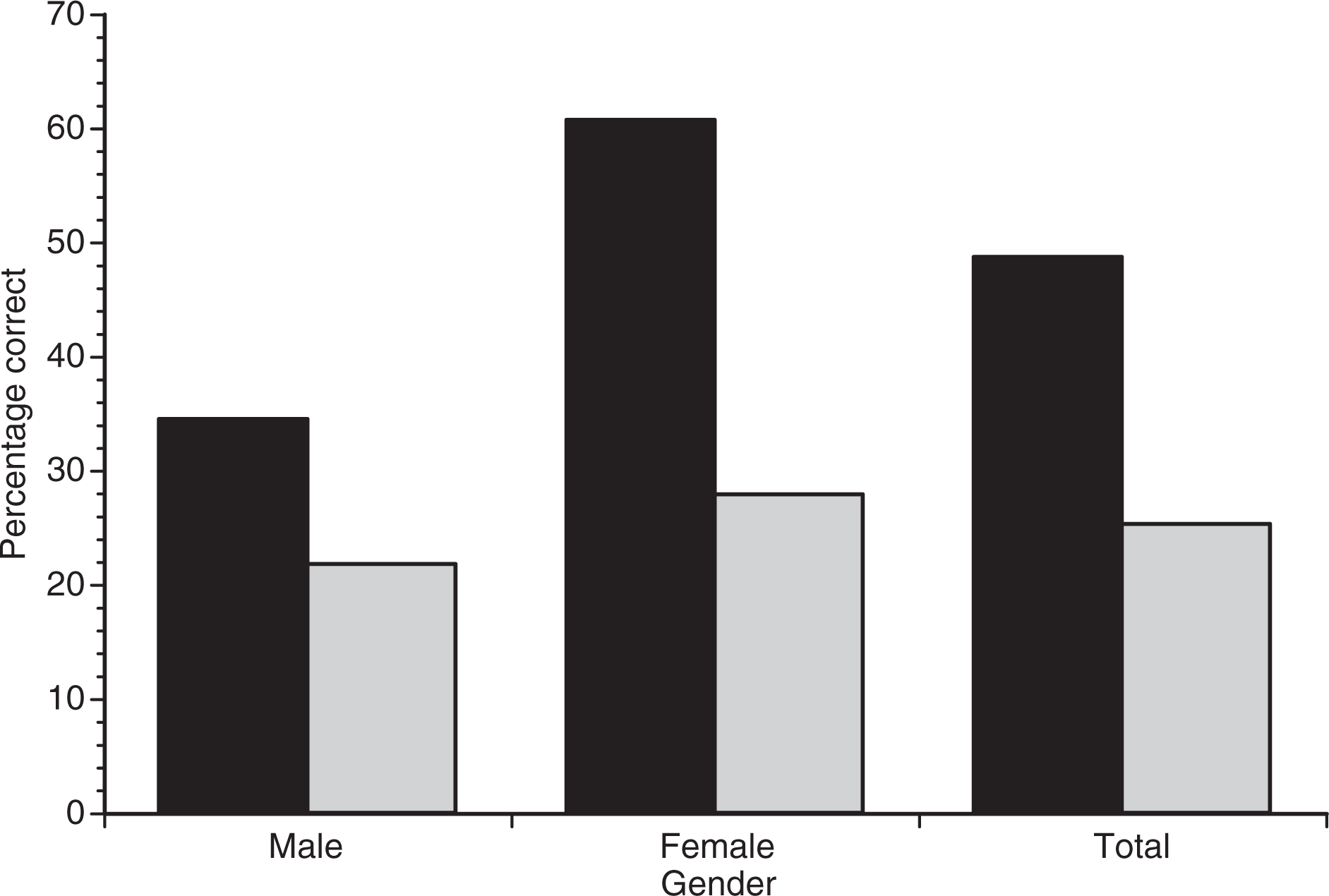
On the whole, males were significantly better at recognizing depression (34.5%, n = 96, N = 278) than they were with psychosis (21.8%, n = 57, N = 261), χ2(1) = 10.67, p = 0.001. Similarly, 18- to 25-year-old males were significantly more likely to correctly identify depression (43.8%, n = 60, N = 137) than psychosis (25.8%, n = 33, N = 128), χ2(1) = 9.43, p = 0.002. For the 12- to 17-year-old males, there was no difference in recognition of depression and psychosis (depression 25.5%, n = 36, N = 141; psychosis 18.0%, n = 24, N = 133), χ2(1) = 2.24, p = 0.13.
Gender differences in the interpretation of depression vignette
Female respondents were significantly more likely to correctly recognize depression than males χ2 (1)=41.15, p < 0.001, regardless of age.
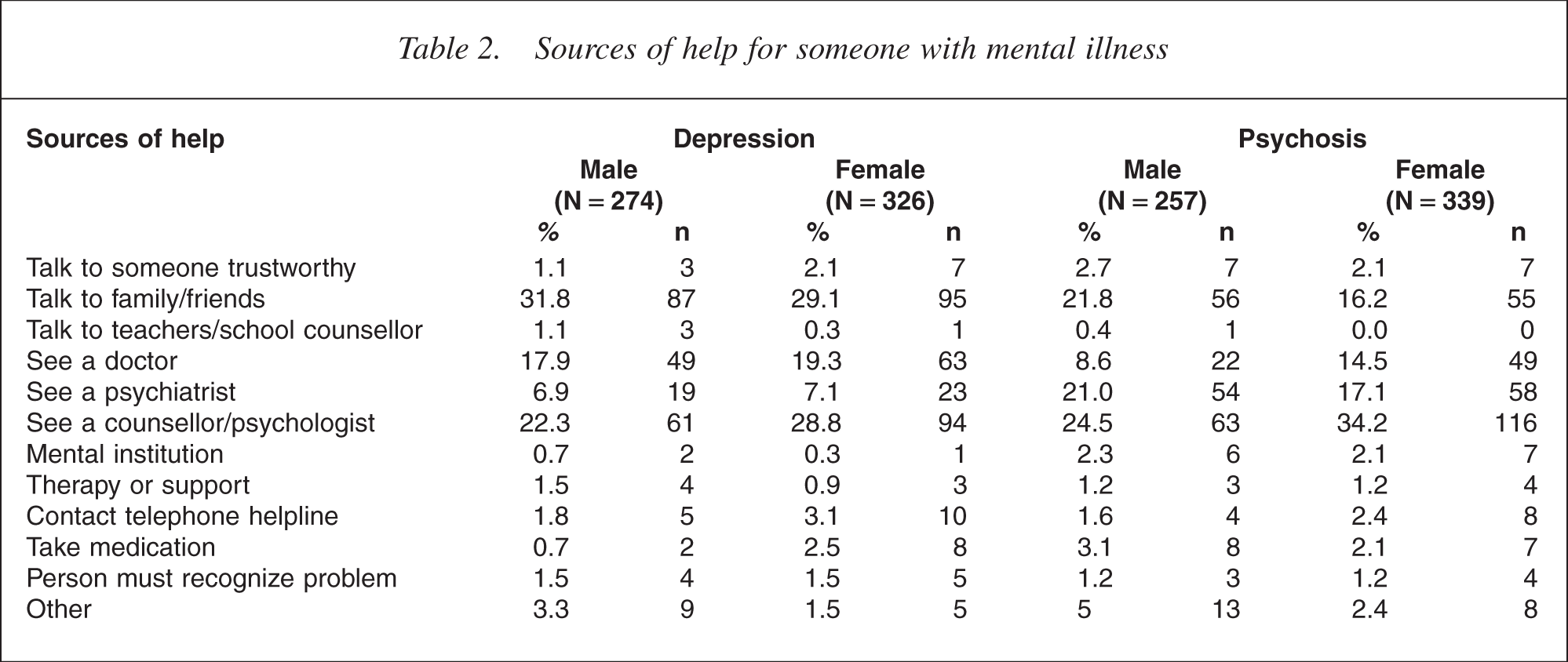
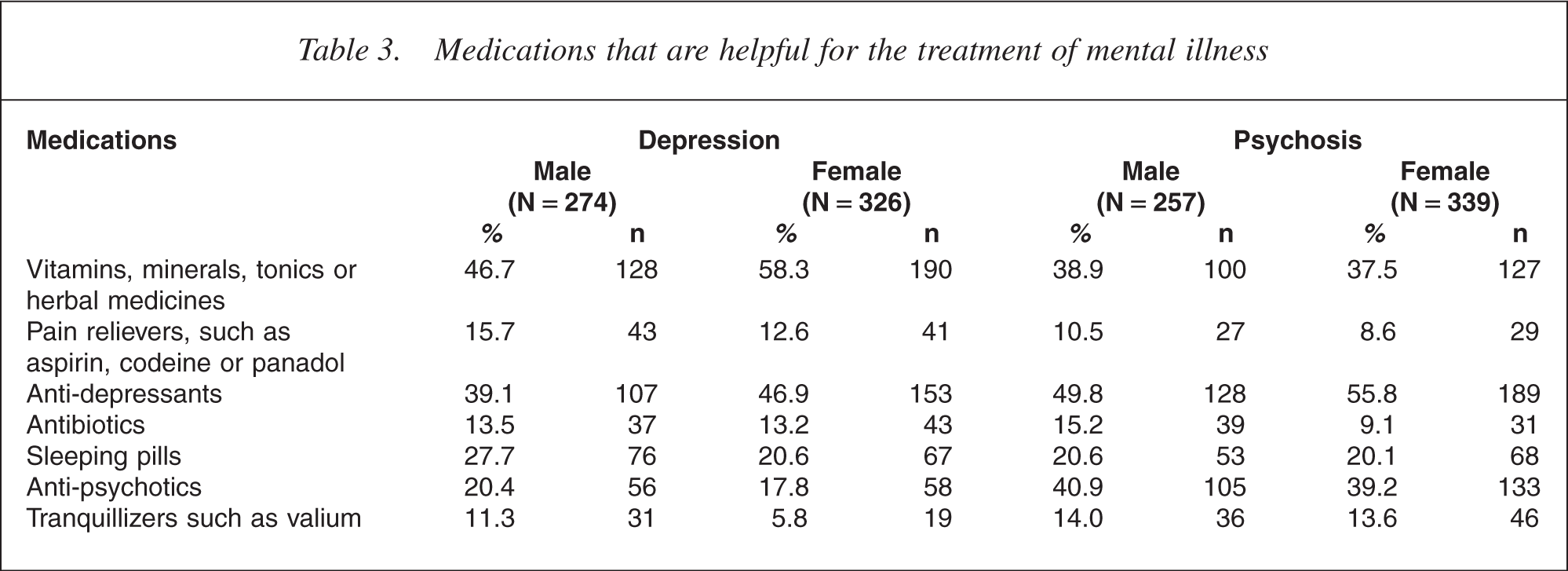
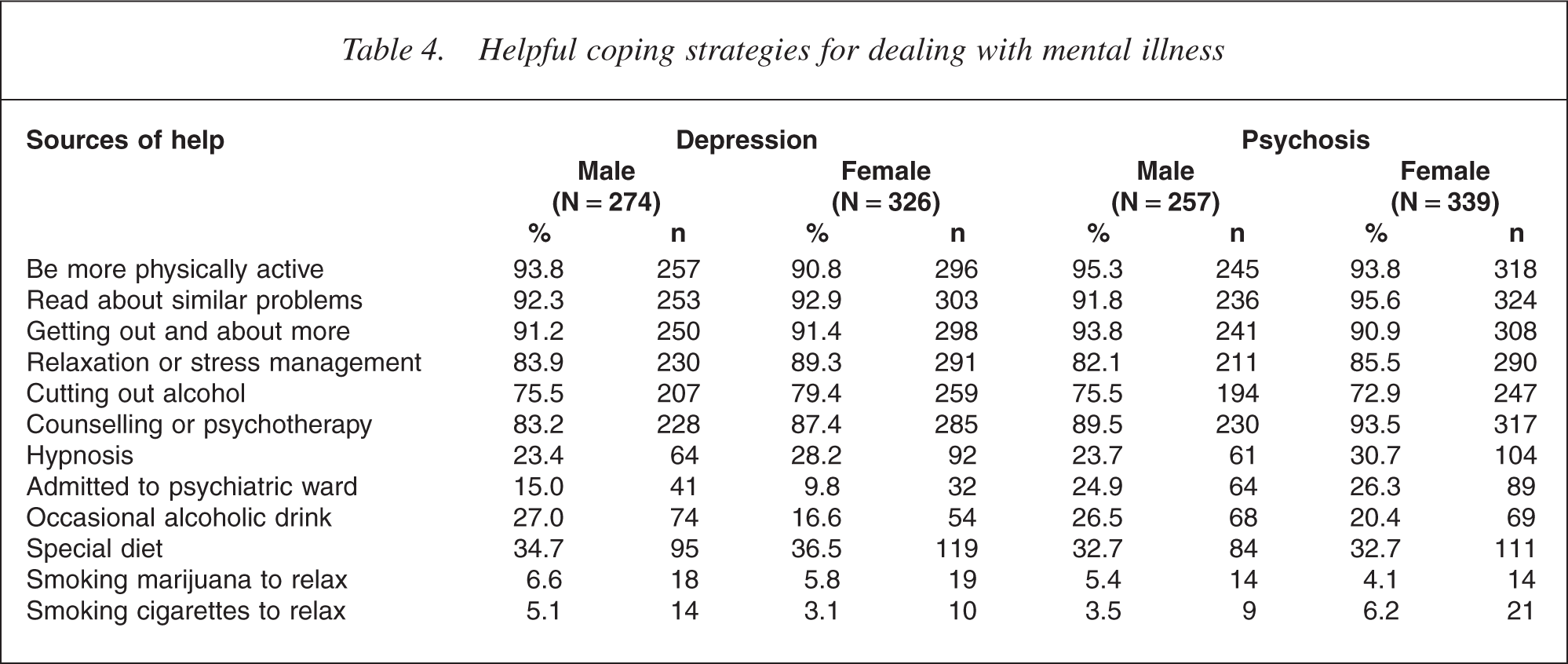
Males were significantly more likely than females to report that the vignette was characteristic of ‘mental illness’, χ2(1) = 5.83, p = 0.016, ‘bully, teasing or peer pressure’, χ2(1) = 8.36, p = 0.004 or the ‘consequence of family problems’, χ2(1) = 1.18, p = 0.041 (see Table 1). No significant differences were found between the genders with respect to views about the sources of help for the character in the vignette (see Table 2). Females, however, were significantly more likely to view vitamins, minerals or herbal remedies to be helpful for the treatment of depression, χ2(1) = 7.99, p = 0.005, whereas males were significantly more likely to favour sleeping pills, χ2 (1) = 4.23, p = 0.040, and tranquillizers χ2 (1) = 5.87, p = 0.015 for the treatment of depression (see Table 3). Interestingly, males were significantly more likely than females to perceive an occasional alcoholic drink as helpful for dealing with symptoms of depression χ2(1) = 9.67, p = 0.002 (see Table 4).
Sources of help for someone with mental illness
Medications that are helpful for the treatment of mental illness
Helpful coping strategies for dealing with mental illness
Gender differences in the interpretation of psychosis vignette
Overall, no significant gender differences were found for the correct identification of psychosis in the vignette, χ2 (1) = 2.91, p = 0.088, however, in the 18-25 years old group, females (19.9%, n = 68, N = 341) were significant more likely than males (12.5%, n = 33, N = 265) to correctly identify psychosis, χ2 (1) = 6.02, p = 0.014. This was difference was not observed for the 12- to 17-year-olds (males 8.8%, n = 24, N = 274; females 8.3%, n = 27, N = 327), χ2(1) = 0.05, p = 0.826.
Gender differences, however, were found with respect to sources of help for psychosis. Males were significantly less likely recommend a doctor, χ2(1) = 4.84, p = 0.028, or a psychologist/counsellor, χ2 (1) = 6.55, p = 0.010 for the treatment of the symptoms of psychosis (see Table 1). Additionally, males were significantly more likely to view antibiotics as helpful for the treatment of psychosis, than females, 2(1) = 5.13, p = 0.024.
The influence of gender of character in vignette
Gender of the character in the depression scenario had an impact on responses. The accuracy of recognition was significantly higher when the character in the scenario was male (53.3%, n = 163, N = 306) than female (44.0%, n = 132, N = 300), χ2(1) = 5.21, p = 0.022. Furthermore, when the character was female (i.e. Mary), males were significantly more likely than females to perceive the symptoms as due to ‘mental illness’ generally, Fisher's exact test, p = 0.015, or as the result of ‘bullying, teasing or peer pressure’ Fisher's exact test, p = 0.038.
Gender of the character in the psychosis scenario made no difference to accuracy of recognition, χ2(1) = 0.85, p = 0.358.
Estimating prevalence of mental illness
Female and male respondents were compared in terms of their estimates of the prevalence (in a 12 month period) of mental illness in young people (see Fig. 2). Initially, the variable was examined in terms of the proportion of respondents with the correct estimate (i.e. one in every four young people) versus incorrect estimate (i.e. all other responses). Only 23.9% (n = 129, N = 539) of males and 25.0% (n = 167, N = 668) of females correctly estimated the prevalence of mental illness in young people, with the difference between the genders being not significant. There was, however, a significant difference between the genders in responding across the five categories of the prevalence variable (see Fig. 2), χ2(4) = 15.36, p = 0.004. Closer examination of the standardized residuals indicated that males were more likely to report that one in every 100 people had a mental illness, z = 1.8, p = 0.004.
Gender differences in the estimation of the prevalence of mental illness in young people. (▪) Male, and (□) female.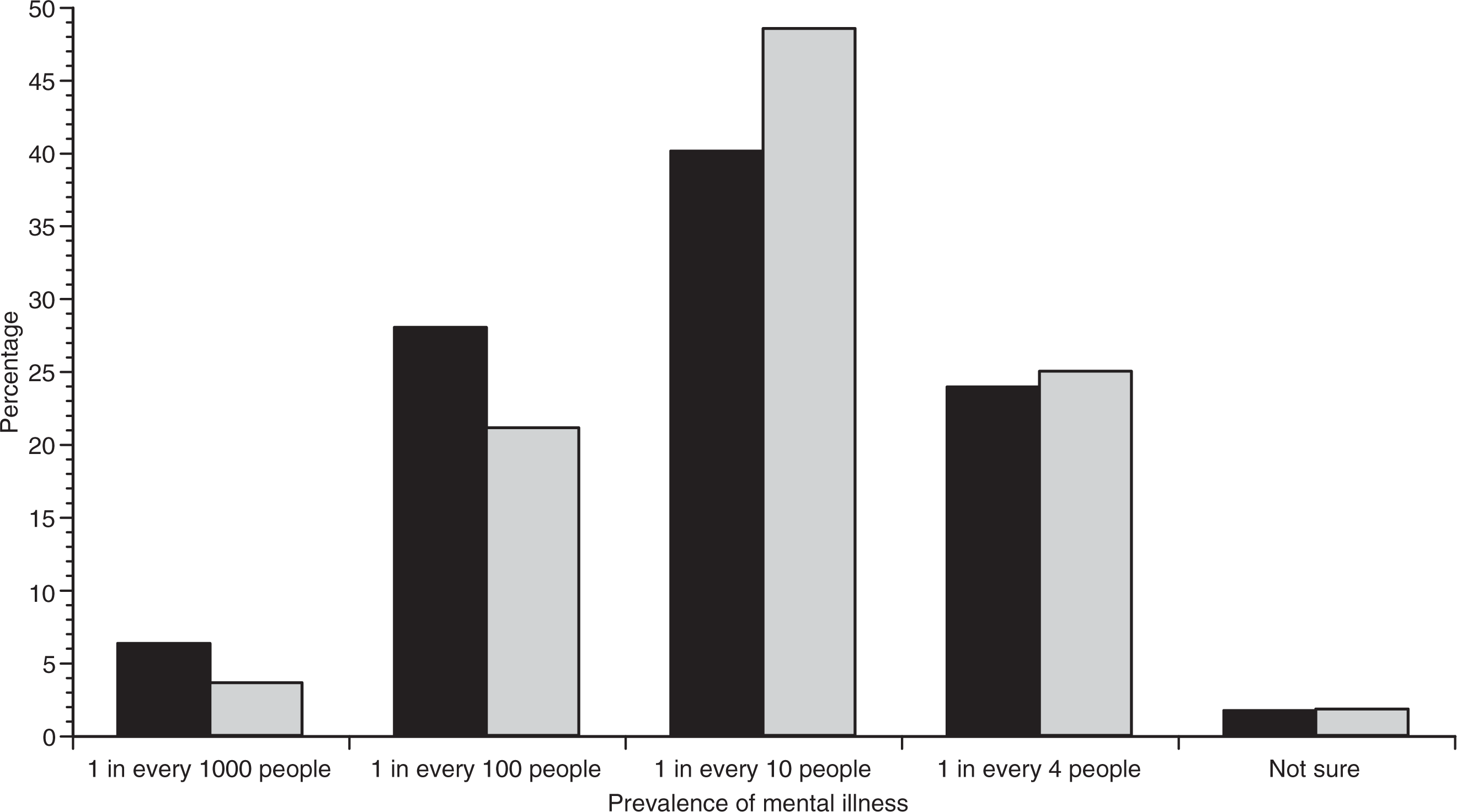
Discussion/conclusions
This study provides a synopsis of gender differences in the mental health literacy of young Australians aged between 12 and 25 years of age. This study is important because of the understanding it gives of the possible reasons for delayed help seeking in young males, therefore adding to the existing survey studies of mental health literacy [1, 3, 4, 10, 11, 13].
Overall, males were significantly less literate than females with respect to knowledge about the symptoms of depression, regardless of age. Males were also more likely to report that the prevalence of mental illness in young people was one in 100.
Although there were no significant differences between the genders with respect to correct interpretation of psychosis, further analysis revealed that the 18- to 25-year-old males demonstrated significantly less awareness of psychosis than females in this age group. This is a disconcerting finding given that, although psychotic disorders are relatively rare, the onset of the first episode psychosis peaks during late adolescence and young adulthood, particularly in males [17].
Both genders, however, had low levels of literacy regarding psychosis, with the correct recognition of this illness for the total sample being only 25.3%. This percentage is comparable to the recognition of schizophrenia in Jorm et al.'s 1997 study [1] where only 27% of 2031 18- to 74-year-olds were able to use the correct terminology to define this illness from a vignette. In follow-up study, conducted in 2006, correct recognition of schizophrenia in the Australian population was reported to be 42.5%, indicating that mental health literacy is improving [3].
Males differed from females in how they identified the symptoms of depression. Males were more likely to use general terms such as ‘mental illness’ or to ascribe the symptoms to external causes such as peer pressure or family problems. One interpretation of this finding is that males are more likely to externalize than internalize mental health problems, particularly depression [18, 19]. Additionally, they were more likely to favour medications such as sleeping pills and tranquillizers, and occasional alcohol use, as potential methods for dealing with such problems. This might explain why depression in males is often masked by problems such as substance use and abuse [20, 21].
Another possible reason for the discrepancy is that males are less likely to have a ‘male’ stereotype for depression due to the lower prevalence of depression within this gender [19, 22]. Conversely, the stereotypes of ‘normal’ women tend to more closely estimate those of ‘mentally ill’ women than do analogous male stereotypes [22].
For the psychosis vignette, males were less likely to recommend the services of doctors or psychologists. These findings support the view that males are generally less likely to value health professional assistance [6, 9, 12, 23]. A surprising finding was that males were more likely to view antibiotics as helpful for the treatment of psychosis, a finding that is difficult to explain except as being reflective of lack of knowledge or awareness.
Gender differences in mental health literacy were also examined by manipulating the gender of the character in vignette. Both male and female respondents were more likely to recognize the symptoms of depression when the character in the vignette was John rather than Mary. No such differences were reported for the psychosis vignette. The trend for depression may be the result of the symptoms presented being more likely to be considered abnormal for males than females. It may be the case that the symptoms are considered stereotypic of a female's menstrual cycle and associated moods or female ‘hysteria’ rather than being abnormal per se [22].
Gender differences in response to the character in the depression vignette diverge from previous findings of Jorm and colleagues [1, 24] who reported that gender in the vignette had little impact on measures of mental health literacy. However, these studies focused on adult populations rather than young people.
The current study has highlighted the poor understanding of mental health problems such as depression and psychosis in males between the ages of 12 and 25 years. Males in the 18-25 years age group demonstrated particularly poor understanding of psychosis which is worrying given that they are at most a risk of developing psychotic illness. The lack of awareness of psychosis in this age range for both males and females is also salient but not dissimilar to previous studies of mental health literacy in the Australian adult population [1]. Further research is needed to ascertain why such gender differences in knowledge and perception about mental illness exist. Consideration needs to be given to whether different types of information and educational strategies would more effectively target the mental health literacy of males and females. Additionally, further research to elucidate the extent to which poor mental health literacy in males may influence and delay their help-seeking behaviour is indicated.
Footnotes
1For the psychosis vignette, none of the respondents used the term ‘psychosis’. A correct response, however, was identified if the young people used the term ‘schizophrenia’.