
Abstract
Mental disorders often have their first onset during youth. For example, the recent New Zealand Mental Health Survey estimated a median age of onset of 13 years for anxiety disorders, 31 years for mood disorders and 18 years for substance use disorders [1]. Young people therefore need to have knowledge to take appropriate action, either for informal self-help or professional help-seeking. However, this is a stage of life at which appropriate knowledge and experience may be lacking.
There are limited data available on the mental health literacy of young people. An Australian regional survey of 12–25-year-olds found poor recognition of depression and psychosis in vignettes, with better identification by young adults than by adolescents [2]. Overall, some appropriate form of help for depression was endorsed by 53% of the sample, and for psychosis, by 63%. Approximately 40% of respondents endorsed medication as an appropriate treatment for either disorder.
Another survey covered high school students in years 8–10 from two parts of Australia [3]. That survey used vignettes of depression and conduct disorder. Depression was recognized in the vignette by around half the students, but conduct disorder was not seen in psychiatric terms. The most frequently endorsed professional helper was a school counsellor, but students preferred to speak to family and friends. Students had a positive attitude towards medication, with almost 60% endorsing antidepressants as likely to be helpful for depression. Other actions seen as helpful were talking to a friend, reading self-help books, avoiding drugs and alcohol and getting more exercise.
More recently, a survey of Sydney adolescents aged 15–17 years examined their ability to recognize depression using a range of vignettes: two meeting criteria for depression (one of which expressed suicidal ideation), one describing someone who presented with grief, one who had broken up with her boyfriend, and one who had drunk too much at a party [4]. Two-thirds of the sample identified depression in the vignette that included suicide ideation, whereas only one-third identified depression in the vignette without suicide ideation. Beliefs about interventions were not examined.
It is not only the mental health literacy of young people themselves that is important for guiding help-seeking, but also that of key supporters. For adolescents in particular, the knowledge of key supporters such as parents may play a critical role in guiding what actions they take for mental disorders. There are relevant surveys of mental health literacy of adults from a number of countries. In general, these show that adults often have beliefs about treatments that differ from those of professionals [5–12].
To fill the gap in information about young people's mental health literacy, we report here the first national survey of this age group, covering both adolescents and young adults, and a survey of their key group of supporters, that is, co-resident parents.
Method
Sample
A national computer-assisted telephone survey was carried out on young Australians aged 12–25 years by the survey company Social Research Centre. The sample was contacted by random-digit dialing covering the whole country from May to August 2006. Up to nine calls were made to establish contact. Interviewers ascertained whether there were residents in the household within the age range and, if there were multiple, selected one for interview using the nearest-birthday method. If the young person lived with a parent, then one parent was also invited to be interviewed using the nearest-birthday method. The response rate was 61.5%, defined as completed interviews (3746) out of sample members who could be contacted and were confirmed as in scope (6087). There were 835 male and 798 female subjects in the 12–17) age group, and 958 male and 1155 female subjects in the 18–25) age group. There were 2925 youth respondents with a parent in the household, of which 2005 completed interviews, giving a response rate of 68.5%.
Interview
The interview was based on a vignette of a young person with a mental disorder. On a random basis, respondents were read one of four vignettes: depression, depression with alcohol misuse, social phobia and psychosis (schizophrenia). Respondents were read a vignette of the same gender as their own. The male vignettes referred to ‘John’ and the female Jenny. The respondents aged 12–17 years were read a version of the vignette portraying a person aged 15 years, while those aged 18–25 years were read one portraying a person aged 21 years. The details of the vignettes were altered slightly to be age appropriate (e.g. reference to functioning at school vs in a course). If a parent was interviewed, they were read the same vignette as their child. Text of the vignettes is available elsewhere [13].
After being presented with the vignette, respondents were asked a series of questions to assess their recognition of the disorder in the vignette, what they would do to seek help if they had the problem, beliefs and intentions about first aid, beliefs about interventions, beliefs about prevention, stigmatizing attitudes and social distance, exposure to mental disorders, the Kessler 6-item (k6) symptom questionnaire [14], exposure to campaigns and media items about mental health, and sociodemographic characteristics. Parents were asked a subset of the same questions as their child, with changes in the wording to reflect the parent's perspective.
The current paper presents data on treatment beliefs, so these are described in detail here. Young people were asked: ‘There are a number of different people who could possibly help John/Jenny. I'm going to read out a list and I'd like you to tell me whether they would be helpful, harmful or neither to John/Jenny. Again, if you are unsure, that's fine, just let me know’. Then the following list was read out: a general practitioner (GP) or family doctor, a lecturer/teacher (the former used for 18–25-year-olds and the latter for 12–17-year-olds), a counsellor, a telephone counselling service such as Lifeline/ Kids Helpline (the service was varied by age group), a psychologist, a psychiatrist, a close family member, a close friend. Next the young person was asked: ‘Is it likely to be helpful, harmful or neither if John/Jenny tried to deal with his/her problems on his/her own?’ and ‘Do you think the following medicines are likely to be helpful, harmful or neither for John/Jenny? Again, if you are unsure, that's fine, just let me know’. The following were then read out: vitamins, St John's wort, antidepressants, tranquillizers, antipsychotics, sleeping pills. Finally, the young person was asked: ‘Do you think the following are likely to be helpful, harmful or neither for John/Jenny?’ and given the following list: becoming physically more active, getting relaxation training, practising meditation, having regular massages, getting acupuncture, getting up early each morning and getting out in the sunlight, receiving counselling, receiving cognitive behaviour therapy, looking up a website giving information about his/her problem, reading a self-help book on his/her problem, joining a support group of people with similar problems, going to a local mental health service, being admitted to the psychiatric ward of a hospital.
Parents were asked the same questions about treatment options as their child.
Statistical analysis
The data were analyzed using percent frequencies and 95% confidence intervals, with the sample divided by age group into adolescents (12–17 years and young adults 18–25 years). The analysis used sample weights that took account of number of in-scope persons in the household, age group, gender and geographic location. The analysis was performed using Intercooled Stata 9 (StataCorp LP, Texas, USA).
Results
The numbers assigned to each vignette were: depression, n = 929; depression with alcohol misuse, n = 944; social phobia, n = 905; and psychosis, n = 968. Table 1 shows the percentages of the groups giving ratings of ‘helpful’ for the various interventions, while Table 2 shows the percentages giving ‘harmful’ ratings. Interventions that had low frequencies of both ‘helpful’ and ‘harmful ratings’ (e.g. St John's wort) were those with frequent ‘neither’, ‘don't know’ or ‘depends’ responses.
Percent (and 95% CI) of youth and parents believing in the helpfulness of various interventions
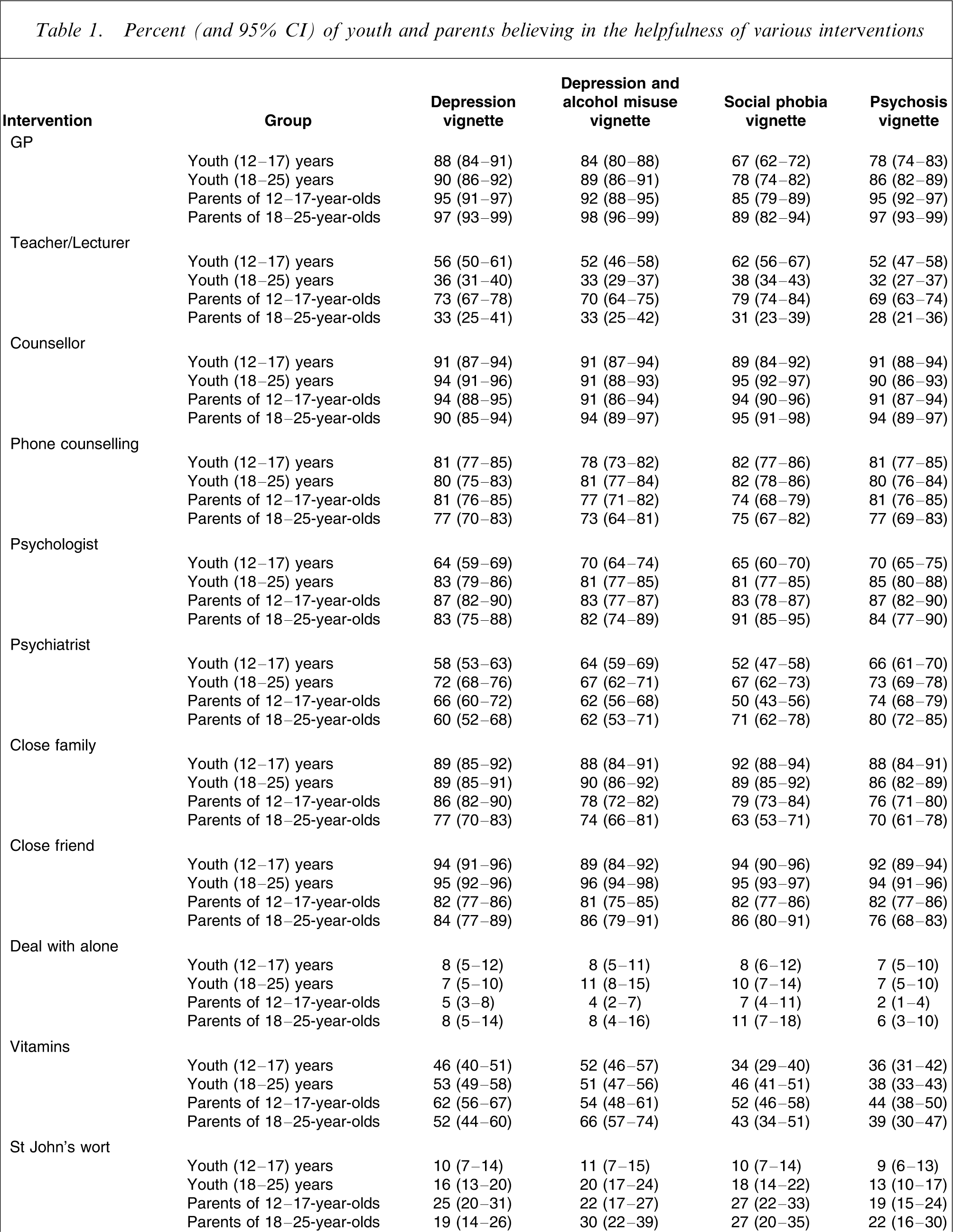
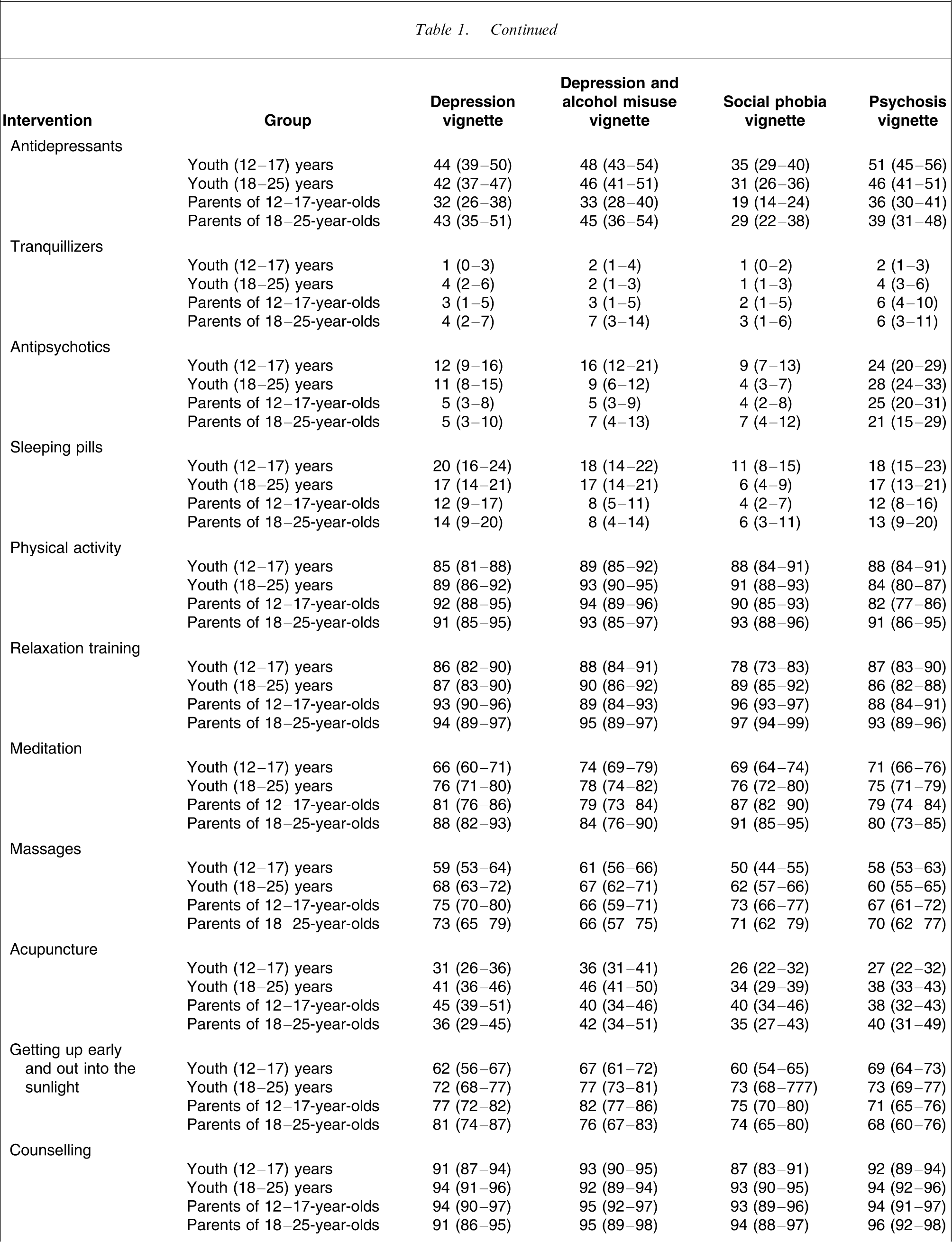
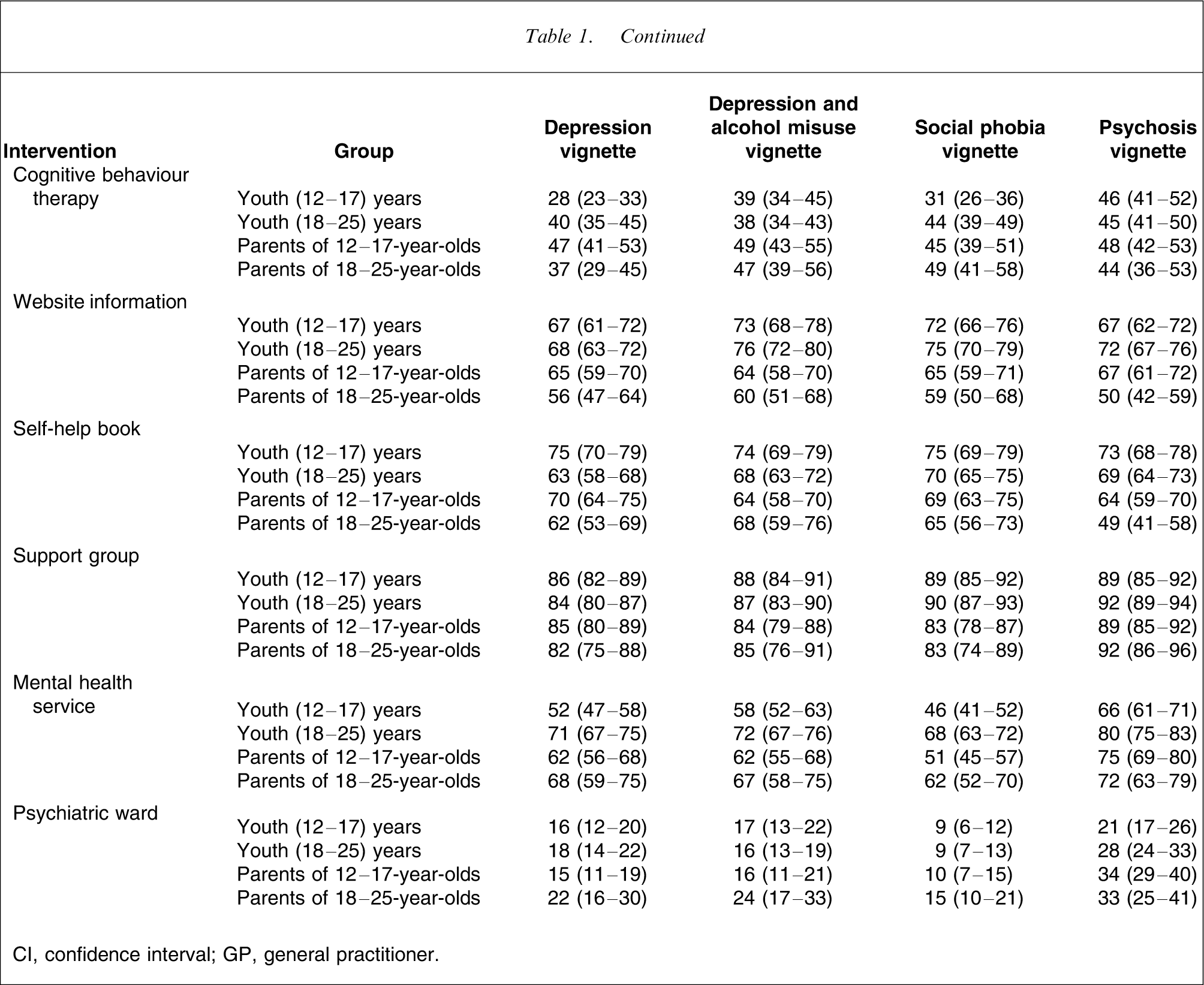
CI, confidence interval; GP, general practitioner.
Percent (and 95% CI) of youth and parents believing in the harmfulness of various interventions
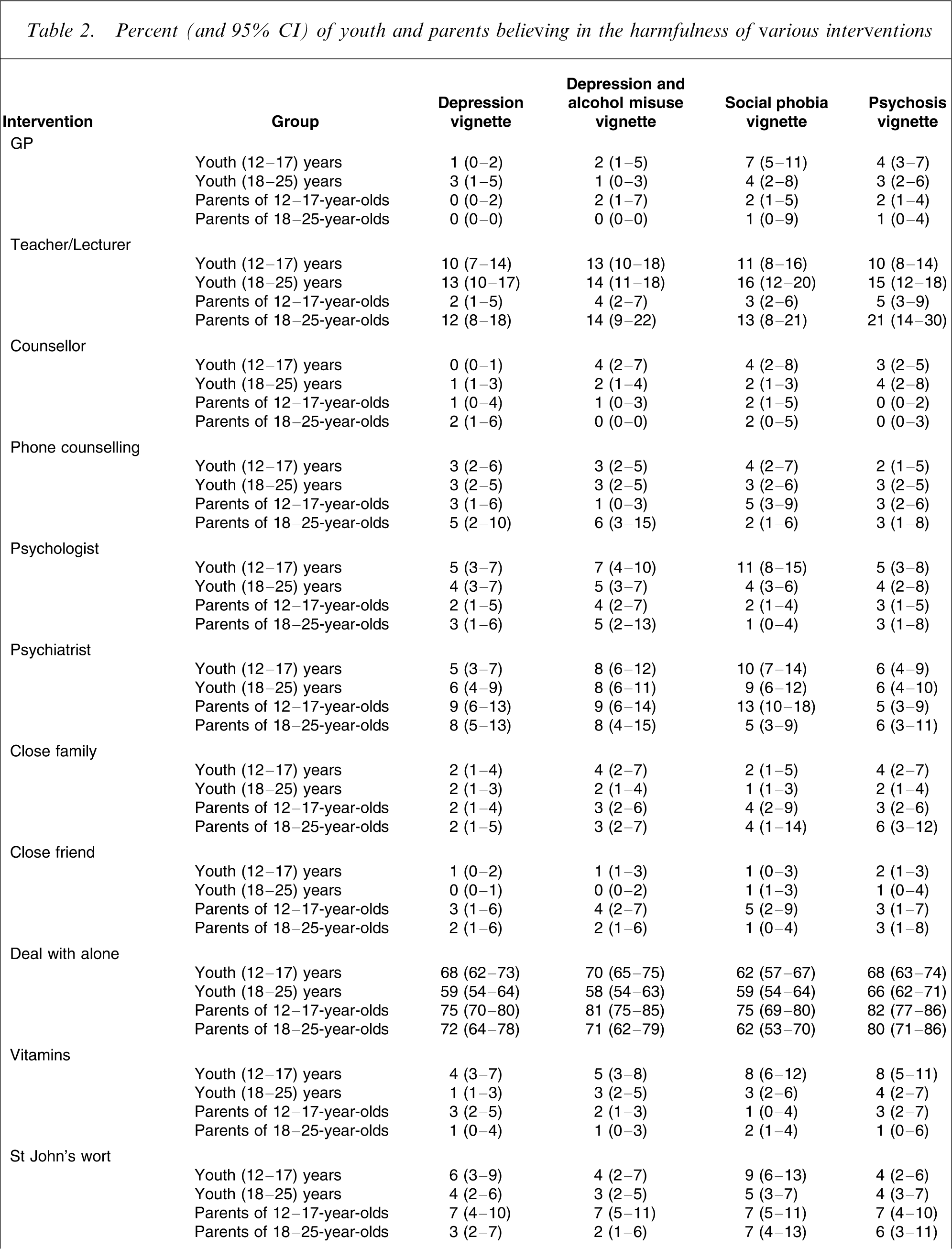
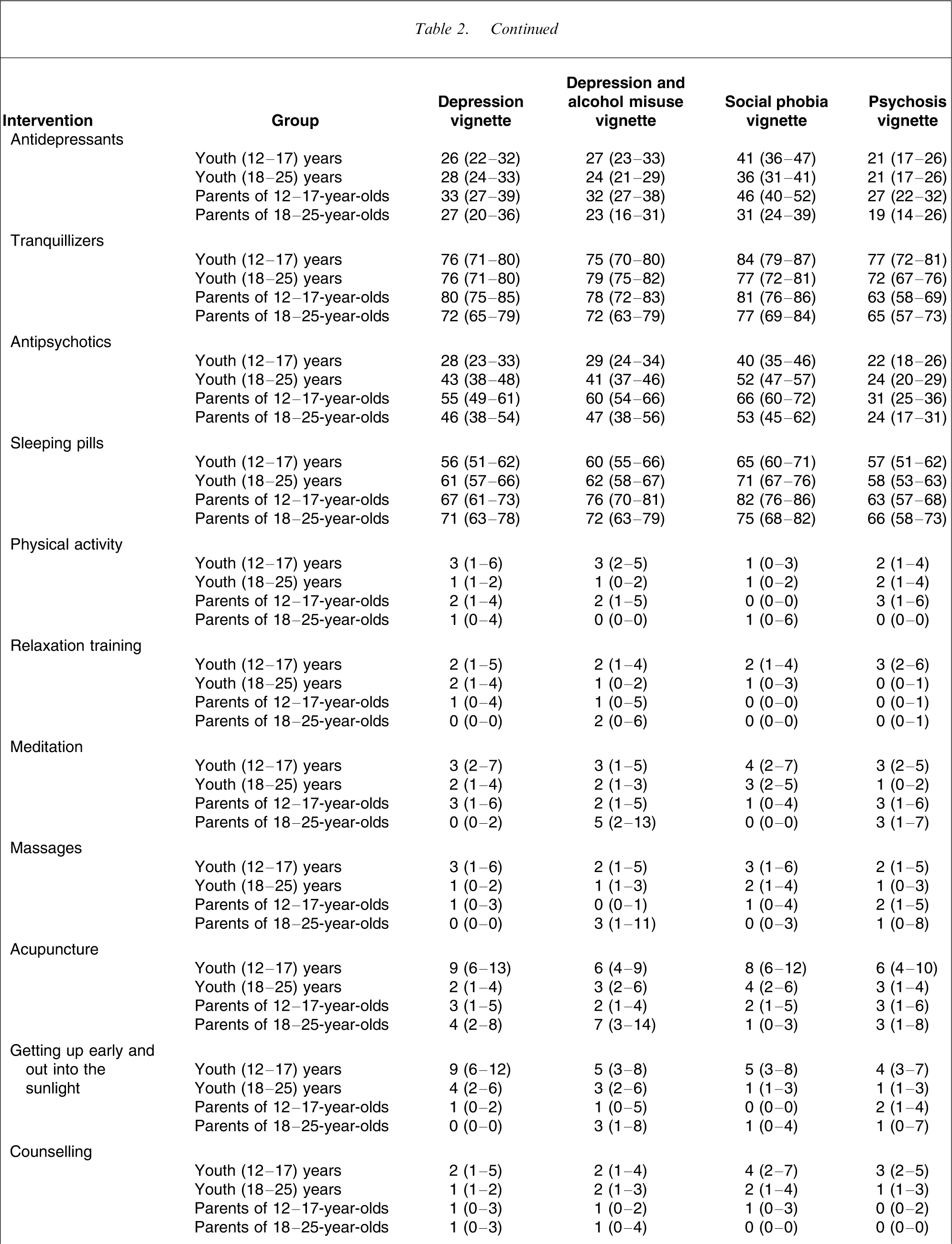
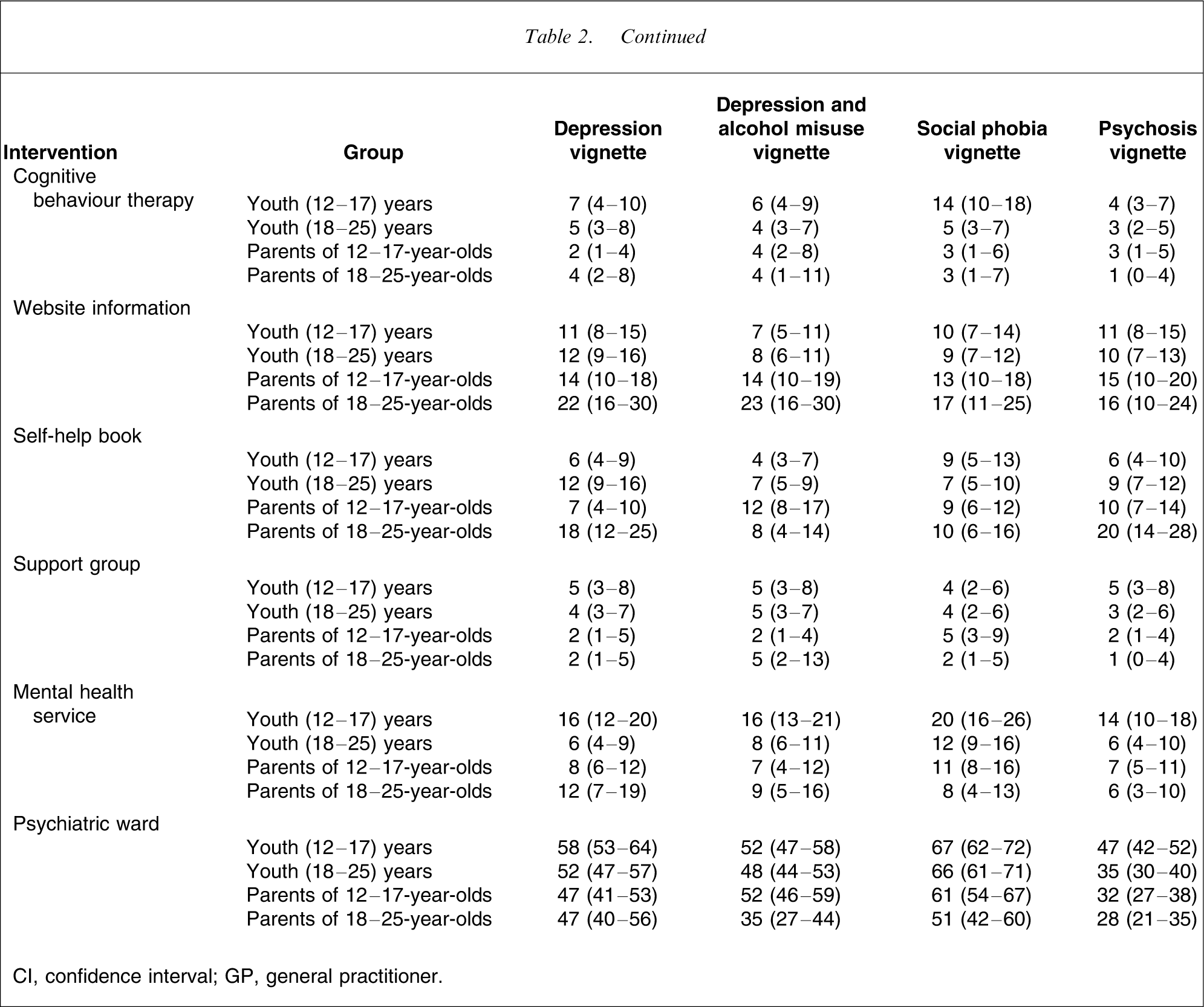
CI, confidence interval; GP, general practitioner.
Areas of agreement between youth and parents
There were substantial areas of agreement between youth and parents. Broadly speaking, the ratings of both groups were similar whatever vignette was presented. Large percentages of both groups agreed about the likely helpfulness of GPs, counsellors, phone counselling, family, friends, physical activity, counselling, and support groups. There was also agreement between youth and parents about the likely harmfulness of dealing with the problem alone, receiving psychotropic medication and being admitted to a psychiatric ward.
Differences between youth and parents
The differences between young people and their parents were less apparent than the similarities. Differences were small to medium in magnitude by Cohen's [15] effect size index h. Parents were more positive about GPs and about seeking help from teachers. Young people were more positive than their parents about help from close friends. One surprising finding was that young adults were more likely to rate close family as likely to be helpful than were their parents. Parents were more likely to see dealing with the problem alone as harmful.
For specialized interventions, parents were more positive than their adolescent children about psychologists, cognitive behaviour therapy and a mental health service. In contrast, compared to adolescents, parents were more negative about a range of psychiatric medications (antidepressants, antipsychotics and sleeping pills), but there was little difference between young adults and their parents in this regard. Parents were also more positive about St John's wort, but this appeared to reflect young people's lack of knowledge of this herbal remedy. Parents also tended to be more positive about a range of complementary treatments (relaxation, acupuncture, meditation and getting up early and into the sunlight).
A notable intervention for which young people were more positive than their parents was getting information from a website, which is consistent with the high internet use of young people. However, there was a similar trend for getting information from a self-help book, which is a more traditional source of information.
Differences between adolescents and young adults
The only major difference between adolescents and young adults was in the greater endorsement of help from a teacher versus a lecturer, which reflects more on the different roles of staff in secondary compared to tertiary education. However, even this was only a medium effect size by Cohen's definition [15]. Other differences between adolescents and young adults were mainly seen with specialized mental health interventions. The young adults were more positive about psychologists, psychiatrists, GPs, cognitive behaviour therapy, and a mental health service. However, they were also more positive about several more specialized complementary interventions: meditation, massages and acupuncture.
Intervention beliefs for specific disorders
Ratings of interventions were broadly similar across vignettes. However, there were some differences that were small to medium in magnitude. Respondents who read the social phobia vignette tended to be less positive about medical interventions such as GPs, psychiatric medications (including antidepressants) and a mental health service. In contrast, those who read the psychosis vignette tended to be more positive about antipsychotics, a mental health service and admission to hospital. Responses to depression were very similar whether or not there was comorbid alcohol misuse.
Discussion
There was broad agreement from young people and their parents about what interventions were likely to be helpful and these views applied across the range of disorders presented. These interventions could be described as general and informal sources of help, rather than as specialist mental health services. The most negative views were about psychiatric medications and admission to hospital, which is consistent with earlier Australian surveys of adults [12, 16] and with findings from other countries [5, 8].
When adolescents, young adults and parents were compared, the differences were less impressive than the similarities. In general we could say that the differences were greater between adolescents and their parents than between young adults and their parents. Parents were more positive about specialist mental health help and complementary treatments, but more negative about psychiatric medications. These differences may in part reflect less developed knowledge or attitudes about specialized mental health interventions and complementary treatments in the younger age group. One surprising finding was that young people (particularly young adults) were more likely to see close family as a source of help than were parents, suggesting that parents may be underestimating their own potential role.
As in previous surveys of adults, the similarities in beliefs across different mental disorders were more impressive than the differences. However, social phobia was seen as less warranting medical intervention, and psychosis more so. The addition of substance misuse to the depression vignette had little impact on ratings of interventions.
The major interest in these findings is where the views of young people and their parents conflict with recommended practice. Such conflicts may lead to delayed or inappropriate help-seeking, or may affect adherence to clinicians’ recommendations. Ideally, the public endorsement of recommended interventions should be close to 100%. The biggest gap is for psychiatric medications, where <50% rated recommended interventions as likely to be helpful. For schizophrenia, antipsychotics are recommended as a core component of clinical care for both adolescents and adults [17, 18]. However, for the psychosis vignette, only a minority of young people and parents rated antipsychotics as likely to be helpful. Approximately as many rated them as likely to be harmful. Fortunately, psychiatrists and mental health services were endorsed by large majorities as likely to be helpful, although this was not true of inpatient admission.
For depression and social phobia, antidepressant medication is also recommended as a core intervention, at least in adults [19, 20]. However, in adolescents they are not recommended for mild depression or as a first-line treatment for moderate–severe depression [21]. In the present survey antidepressants were the most favourably viewed psychiatric medication, but still less than half thought they would be helpful for depression and an even smaller proportion thought they would be helpful for social phobia. Interestingly, parents were less favourable towards antidepressants in adolescents than in young adults, which is consistent with clinical guidelines. In all groups surveyed, antidepressants were viewed less favourably than vitamins, which is a pharmacological therapy not supported by evidence.
Psychological therapies, such as cognitive behaviour therapy, are recommended for all the disorders covered in the survey [17–21]. Cognitive behaviour therapy was rated as likely to be helpful by less than half of adolescents, young adults and parents, and this held irrespective of the vignette presented. However, this low rating was largely because of ignorance of this treatment (which may be related to its limited availability). Unlike medication, respondents did not often see it as harmful. By contrast, the non-specific psychological intervention of counselling was overwhelmingly rated as likely to be helpful by all groups for all vignettes. Similarly, psychologists and psychiatrists, who would often administer psychological therapies, were rated less positively than counsellors.
Previous surveys of adults have shown relatively positive views of complementary and self-help therapies. In the present survey we asked about a range of interventions not covered in the earlier surveys. The complementary and self-help therapies included were those known to have some evidence for effectiveness in treating depression or anxiety disorders in adults [22, 23], although the amount of evidence on these therapies with adolescents is much poorer [24], making comparison with young people's preferences more difficult. Many of these therapies were frequently rated as likely to be helpful (physical activity, relaxation training, meditation, massages, morning light exposure, self-help books). St John's wort did not rate so highly, but this appeared to be largely due to ignorance of what it was rather than a concern about possible harms.
These findings have implications for areas on which campaigns to improve mental health literacy need to focus in the future. The first is in attitudes towards medication. Although there is evidence that attitudes of adults in Australia have become more favourable in recent years [16, 25], there is still a considerable gap with clinical practice guidelines. The second is with the preference for generic psychological interventions (counselling) compared to specific interventions known to be effective (e.g. cognitive behaviour therapy). A similar gap exists with the professions providing psychological therapies (psychologists and psychiatrists vs counsellors). There is evidence that knowledge and attitudes of young people and adults can be changed by community campaigns [26, 27] so these are feasible goals. Recent changes in funding provided under Australia's national health insurance scheme, Medicare, have made psychological services more readily available, but young people need to know about the availability and usefulness of these services.
Another possible approach to improving evidence-based care for young people would be to use terms to describe services that would make them more appealing to this age group and their parents. For example, services might be more acceptable if psychological therapies were labeled as ‘counselling’ and mental health professionals as ‘counsellors’. To some extent, this approach runs counter to the aim of improving mental health literacy and requires cautious exploration.
The present results highlight the need for further evidence on complementary and self-help interventions. We face a situation in which some therapies that have a strong evidence base are perceived less favourably than others that have weaker supporting evidence. As well as trying to improve the mental health literacy of the public about what is known to work, we need to do further evaluation of interventions that already have wide acceptance and use. Interestingly, a recent study found that people who had experienced depression also rate many of these types of interventions as having helped them [28].
Because of their more limited life experience, adolescents require assistance from others in their social network to seek appropriate professional help. In this regard, both family and close friends are viewed favourably as sources of help. However, parents tended to underrate their importance compared to their children. Parents need to be a target for first aid knowledge and skills to assist young people who develop mental disorders [13]. Although it is perhaps too much to expect young people to provide a high level of peer support, there is certainly room for some basic skills. For example, adolescents often do not respond to a friend in a way that could facilitate appropriate help, such as engaging a parent, teacher or school counsellor to help [29]. Even with a suicidal peer, many young people would not tell an adult [30].
The study has several limitations. The survey elicited responses in relation to hypothetical vignettes. Although the vignettes were matched in age group and gender to the young respondent, these responses may not correspond to beliefs or actions that would operate if the young person actually developed a mental disorder. Another limitation is that some of the interventions may have been unknown to the respondents, particularly the younger ones. Terms such as ‘psychiatrist’, ‘psychologist’ and ‘cognitive-behaviour therapy’ are not always understood, even by adults. Nevertheless, the survey does elicit responses to labels that might be used in a help-seeking situation. For example, if a young person has a negative reaction to being referred to a psychiatrist or being prescribed an antidepressant, this reaction is relevant whether or not the intervention is understood.
In conclusion, this is the first national survey of young people's treatment beliefs in any country. As in previous surveys of adults, it found some gaps between public perceptions and current clinical practice. These gaps can be the target of community mental health literacy campaigns and training of key supporters in first aid skills. However, consideration can also be given to describing some interventions using terminology that may make them more acceptable to young people. Furthermore, the evidence base needs to be extended to more fully evaluate those complementary and self-help interventions that are already widely accepted by young people.
Footnotes
Acknowledgements
Amy Morgan assisted with the organization of the survey. Claire Kelly, Robyn Langlands, Betty Kitchener and Len Kanowski had input into the survey content. Darren Pennay and Graham Challice from the Social Research Centre provided advice on survey methodology. Funding was provided by the National Health and Medical Research Council, the Colonial Foundation and beyondblue: the national depression initiative.