
Abstract
In the 2005 Budget, the Australian government announced significant reform of the social security or welfare system, placing greater obligations on a range of payment recipients (lone parents, disability pensioners) to look for and engage in work as a requirement for payment. Increasing the rate of workforce participation rates is argued to be necessary given the projected ageing Australian population and declining proportion of the working age population in employment [1]. Government ministers have also suggested that the proposed changes are intended to improve the wellbeing of individuals and families reliant on welfare [2–6].
The US academic Lawrence Mead has been influential in Australia and internationally in the conceptualization of welfare dependency and promotion of work-first policy responses [7,8]. Mead argues that long-term reliance on welfare payments creates a culture of dependency, leading to a lack of personal competency and personal efficacy, and heightened feelings of hopelessness and despair. In response, he advocates ‘paternalistic’ policies that are directive, involve close supervision and impose behavioural requirements and obligations so as to increase self-reliance (see Pearson for similar discussion of indigenous welfare dependency) [9,10]. Thus, psychiatric and psychological research and practice is highly relevant to, but little considered in the current social policy debate.
In previous research, we demonstrated the greater prevalence of common mental disorders (anxiety, depression and substance use) and disability because of poor mental health among welfare recipients compared with non-recipients [11–13]. Analysis of the Australian National Survey of Mental Health and Wellbeing (NSMHWB), for example, found that 45% of lone mothers receiving income support experienced a diagnosable mental disorder in the previous 12 months, as did 34% of unemployed welfare recipients. Rates among nonrecipients were around 19%. These findings are not unexpected given the well-established relationship between mental health and socioeconomic and demographic factors such as unemployment, poverty, lone parent status and social exclusion [14–16]. Recent analysis of data from the NSMHWB at both individual and aggregate levels has also demonstrated the relationship between psychiatric disorders, suicidal behaviour and measures of socioeconomic circumstances [17–19].
A critical question is whether the adverse psychological characteristics of welfare recipients are a consequence of welfare dependence. Alternatively, the sense of hopelessness and poorer psychological wellbeing of welfare recipients may reflect other contemporaneous circumstances (financial hardship, relationship breakdown) or long-term disadvantage (socioeconomic status, poor human capital and work skills, adverse early experiences). In research with lone mothers in the US, Petterson and Friel [20] found that elevated rates of depression and hopelessness among welfare recipients were a reflection of material deprivation. Rates were similar for those on welfare and in low-pay jobs, but much lower for those in higher paying jobs.
The aim of this paper is to extend our analyses of the NSMHWB and examine the concepts related to the personal despair and hopelessness hypothesized to be a consequence of welfare dependency. We consider suicidal ideation (having thoughts of killing oneself), suicide attempts and measures of psychological wellbeing (reported feelings of hopelessness, worthlessness and dissatisfaction with life). These measures explore in psychiatric terms the concepts discussed in the social policy literature. In considering mediating or confounding factors, we do not focus solely on immediate circumstances, but also consider measures of long-term social disadvantage and personal characteristics. Finally, this research also has a broader objective of demonstrating the role of psychiatric epidemiology and other mental health disciplines in informing the development of social policy and interventions, and monitoring and evaluating the outcomes of welfare reform.
Method
Sample
The analysis used the confidentialized unit record file of the NSMHWB. The survey was conducted by the Australian Bureau of Statistics (ABS) in 1997. The NSMHWB used a representative sample of people living in private dwellings from all States and Territories. It remains the only data providing comprehensive national information on the prevalence of major mental disorders, the associated levels of disability and health service usage in Australia. About 13 600 households were approached, with one person aged 18 or over from each house selected for interview. Overall, 10 641 individuals completed the survey (a 78% response rate). The sample was weighted based on State, part-of-State, age, gender and probability of selection to match the overall Australian population.
Measures
The study considered items representing suicide ideation and attempts, and reported hopelessness, worthlessness and dissatisfaction with life. These items were examined separately and also combined into a composite score. The survey used a modified version of the Composite International Diagnostic Interview (CIDI). Survey participants who responded positively to screening questions for the depression module (periods of being sad, empty or depressed in the last 12 months; or lost interest in work, hobbies and other things usually enjoyed in the last 12 months) were asked about suicidal ideation in the previous 12 months (‘Did you feel so low you thought a lot about committing suicide?’). Those who reported suicidal thoughts were asked whether they had attempted suicide. All survey respondents were asked about lifetime suicidal ideation and, subsequently, suicide attempts. Two items from the K10 scale of psychological distress [21] assessing feelings of hopelessness and worthlessness in the past 4 weeks were examined. For these measures, respondents who reported such feelings ‘some’, ‘most’ or ‘all of the time’ were categorized as experiencing each psychological symptom. The survey included the life satisfaction scale of Andrews and Withey [22] which asked ‘How do you feel about your life as a whole, taking into account what has happened in the last year and what you expect to happen in the future?’ Respondents were classified as dissatisfied if they responded ‘mostly dissatisfied’, ‘unhappy’, or ‘terrible’.
The NSMHWB assessed a range of sociodemographic variables including age, gender, marital status (collapsed into partnered and not partnered), labour force status, occupation, main source of income, number of children in household and educational attainment. The NSMHWB dataset included the ABS-derived Index of Relative Social Disadvantage, which reflects the socioeconomic circumstances of geographical areas. Individuals were categorized as living in a low socioeconomic area if their place of residence was in the lowest two quintiles. Respondents were classified with a physical condition if they reported experiencing any of a list of 12 common chronic conditions and were classified with a physical disability (mild, moderate, severe) if they obtained scores of less than 50, less than 40 and less than 30, respectively, on the Physical Component Summary Scale from the SF12 [23,24]. Four questions from the posttraumatic stress disorder module of the CIDI were used to assess lifetime experience of physical and sexual violence (rape, sexual molestation, serious physical attack, threatened with a weapon or tortured) which is utilized not just as a measure of trauma but also as a surrogate indicator of adverse life circumstances [25,26]. An item from the Eysenck Personality Questionnaire [27] assessed whether respondents ‘often feel lonely’ and those who responded ‘yes’ were classified as lonely, used as a proxy for perceived social support. Finally, analyses also controlled for the presence of any anxiety disorder, any depressive disorder, and harmful alcohol or drug use or dependence in the previous 12 months assessed using the CIDI according to the ICD-10 classification.
Analysis
The analysis focused on survey respondents of workforce age, that is, men aged under 65 years and women aged under 60 years. Reliance on income support was defined as reporting government pensions or payments as main source of income. The sample was divided into six groups, with non-recipients the reference category for all analyses. Five different groups of income support recipients were derived from sociodemographic characteristics to correspond to the main types of payments: unemployed; students; partnered women with children; unpartnered women with children; and not in the labour force (NILF, which previous research has demonstrated primarily represents recipients of Disability Support Pension and other payments available to mature-aged people [11]). Further information on the formation and validation of the individual client segments is available in previous publications [11,13].
The association between sociodemographic characteristics and income support status was examined using chi-squared tests. A series of logistic regression models were used to examine the association between income support status and each of the psychological and suicidal behaviour outcomes. Given the similar pattern of results evident for the outcome measures examined, the three psychological and two suicidal behaviour measures (12-month attempts and ideation) were combined to create a demoralization scale, which was analysed in several different ways. Sequential logistic regression models examined whether measures of socioeconomic status (educational attainment and occupation) and, subsequently, psychiatric disorders and other sociodemographic and personal characteristics (partnered status, physical health, presence of children, loneliness, adverse life experiences) explained the relationship between income support status and each of the outcome measures. To further control for socioeconomic differences between recipient and non-recipient groups, the analyses were replicated on the subset of respondents residing in areas of greatest socioeconomic disadvantage.
Statistical analyses were conducted using STATA (Stata Corporation, Release 8.0). Data were weighted to reflect population parameters and robust (Huber/White) estimates of variance were used.
Results
There were significant differences among the non-recipient and welfare recipient groups on all characteristics shown in Table 1 (all chisquared tests of association significant at p < 0.001). Some differences are a consequence of the way in which groups were defined (i.e. lone and partnered mothers are women). Nonetheless, many categories of welfare recipients reported poorer physical health, lower levels of educational attainment, were more likely to have experienced physical and sexual violence, reported higher rates of loneliness, and elevated prevalence of common mental disorders (anxiety, affective and substance-use disorders).
Sociodemographic characteristics of the income support and non-recipient client groups
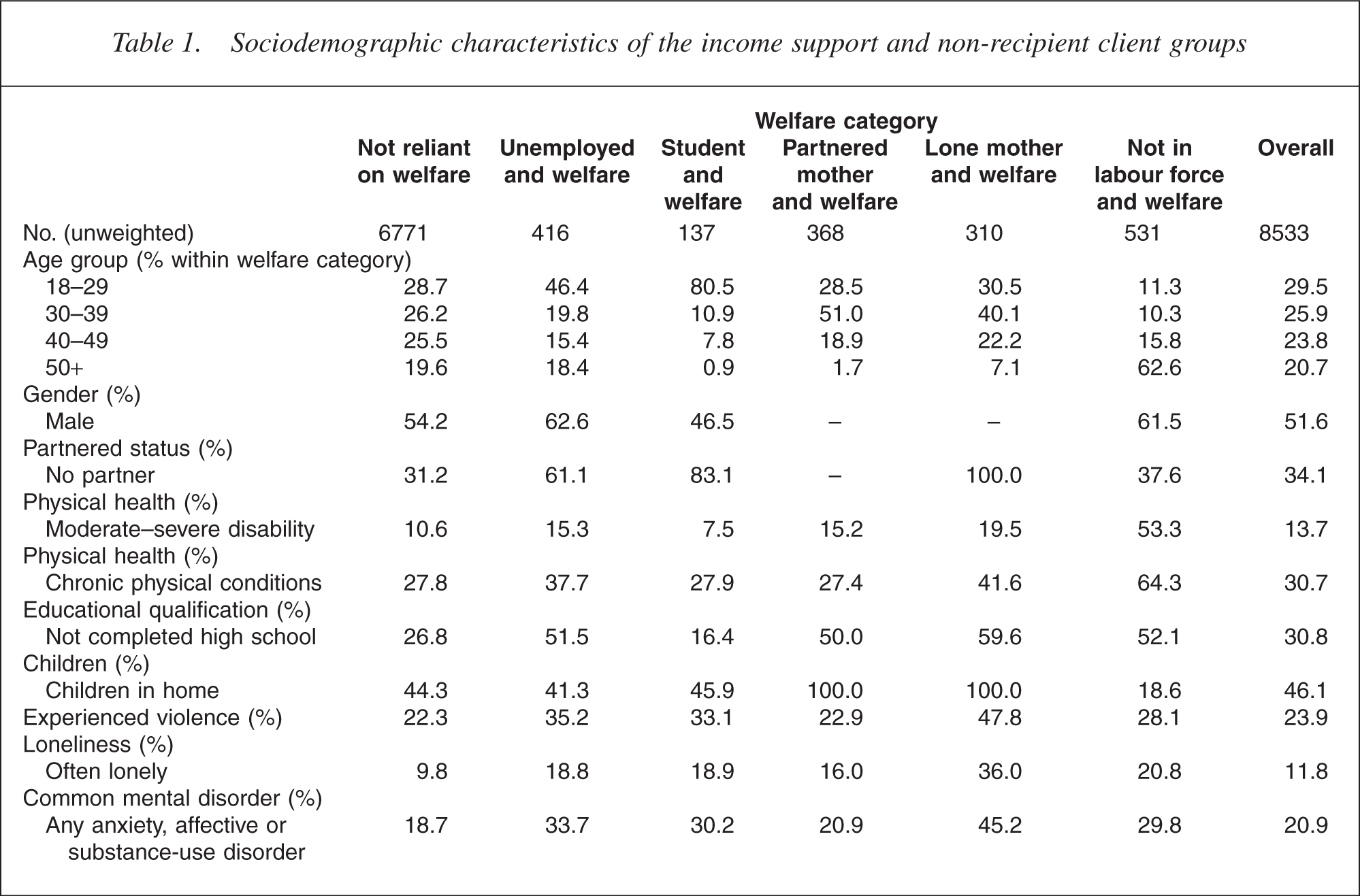
Table 2 shows prevalence rates for each of the psychological symptoms and suicide measures (Table 3, model 1 presents odds ratios and 95% confidence interval from simple logistic regression models for many of these comparisons). Non-recipients are the reference category for each analysis. Welfare recipients in the unemployed, lone mother and the NILF (primarily recipients of disability payments) groups reported significantly higher levels of hopelessness, worthlessness and dissatisfaction with life compared with non-recipients. In contrast, full-time students receiving income support did not report elevated rates on any of these psychological outcomes. Partnered mother recipients demonstrated higher rates than non-recipients on the hopelessness and worthlessness items, although rates were much lower than for the previously mentioned three groups. Post-hoc analyses confirmed that partnered mother recipients were significantly less likely to report these psychological symptoms than lone mother and NILF recipients.
Prevalence of adverse psychological wellbeing, suicidal behaviour and demoralization for the income support and non-recipient client groups
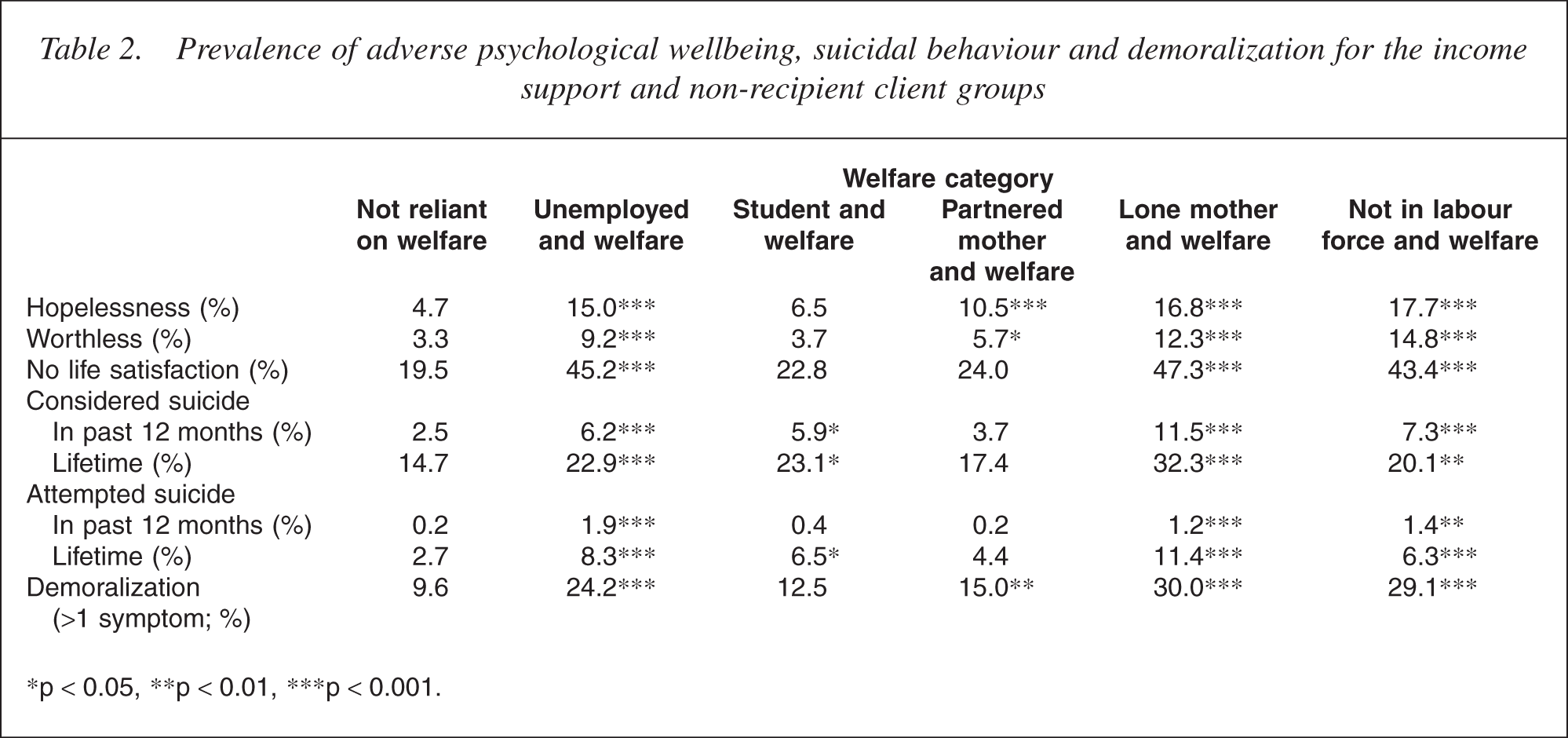
∗p <0.05, ∗∗p <0.01, ∗∗∗p <0.001.
Odds ratios (and 95% CI) from sequential logistic regression models showing association between the income support and non-recipient client groups and psychological and suicide measures and demoralization
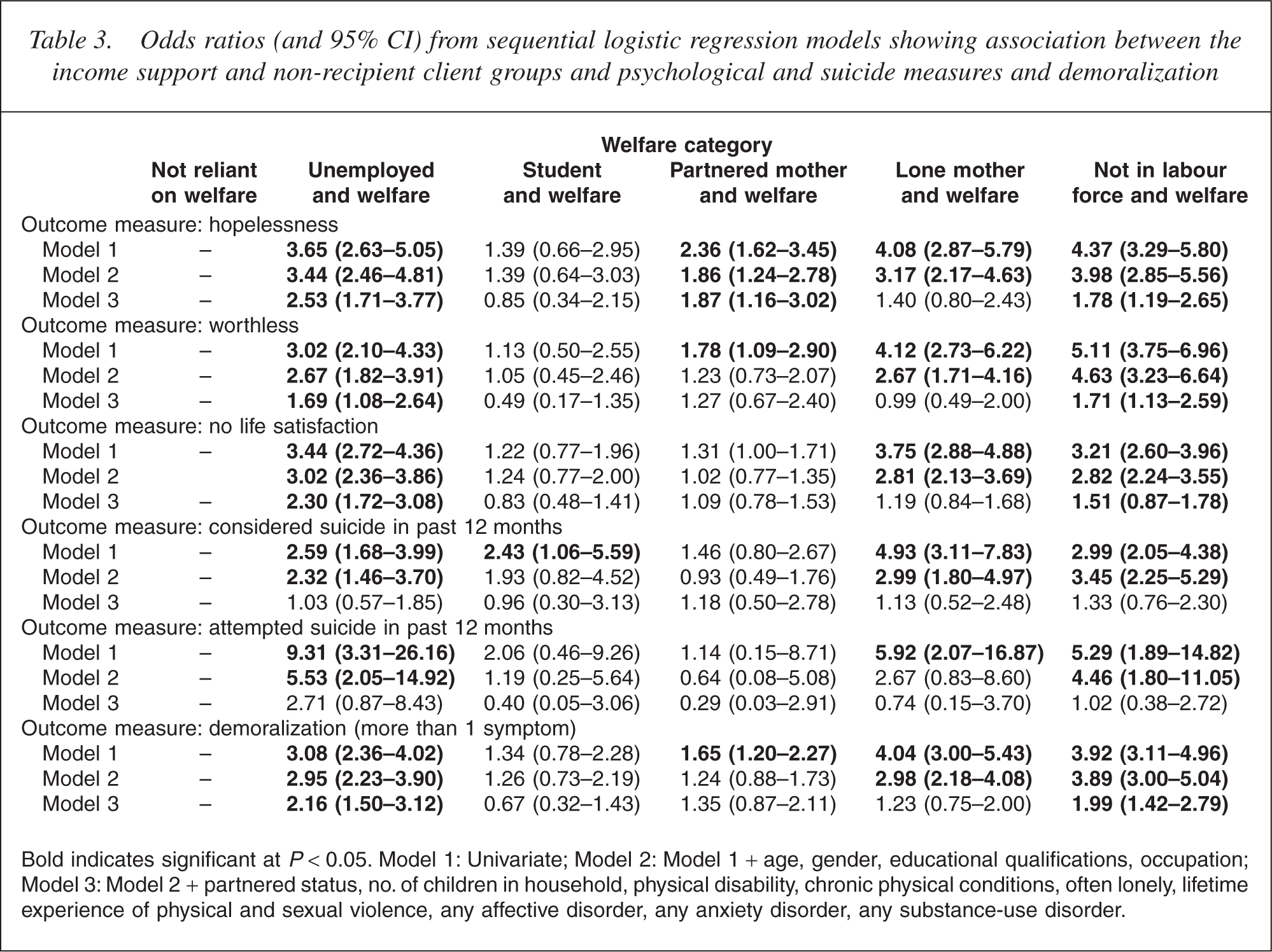
Bold indicates significant at P < 0.05. Model 1: Univariate; Model 2: Model 1 + age, gender, educational qualifications, occupation; Model 3: Model 2 + partnered status, no. of children in household, physical disability, chronic physical conditions, often lonely, lifetime experience of physical and sexual violence, any affective disorder, any anxiety disorder, any substance-use disorder.
Whereas 2.5% of those not reliant on welfare payments reported suicidal ideation in the past 12 months, the rate among lone mothers receiving welfare was 11.5% (increased odds of over 5). Rates were also significantly elevated among the other welfare groups with the exception of partnered mother recipients. Similarly, rates of lifetime suicidal ideation were higher for these four groups of welfare recipients (unemployed, lone mothers, NILF and students) compared with nonrecipients, although the strength of the effect was less than for the 12month prevalence measures (odds ratios ranged from 1.5 for the NILF group to 2.8 for the lone mother group). Considering suicide attempts in the past 12 months, 0.2% of non-recipients reported recent suicide attempts whereas the rates among the lone mother, NILF and unemployed groups were 1.2, 1.4 and 1.9 (increased odds of 6–9). Reported lifetime attempts were also elevated in these three groups, with the highest rate among lone mother recipients (11.4%). Rates of suicide attempts were not elevated among partnered mother recipients relative to non-recipients, while student recipients only demonstrated significantly higher rates of lifetime attempts.
The broad similarity in the pattern of results across the individual outcome measures supports the decision to combine the items (including the 12-month prevalence suicidal behaviour measures) into a single scale that assesses demoralization. Exploratory factor analysis of the five items, recognizing the measures as categorical variables, identified one dominant factor with an eigenvalue greater than 1 and reasonably similar factor loadings for each variable (range 0.65 to 0.93). We also obtained similar results from analyses that combined these items in different ways, including analysis of factor scores (using linear regression), a count of symptoms (using negative binomial regression), or logistic regression results based on various cut-points (0 vs 1 or more symptoms; 0 or 1 vs 2 or more symptoms). The results presented in Table 2 report the percentage of respondents in each income support category reporting 2 or more of the symptoms. Three groups of welfare recipients (unemployed, lone mothers and NILF) reported much higher rates than non-recipients and, according to post-hoc testing, greater than the rates among partnered mother and student recipients. Nonetheless, partnered mother and student recipients reported somewhat higher rates than non-recipients (partnered mothers significantly greater).
Table 3 presents the results of a series of sequential logistic regression models which examined the extent to which the relationship between income support receipt and each of the psychological symptoms and 12-month suicidal behaviours was explained by other covariates. Significant odds ratios are in bold. Model 2 includes measures of socioeconomic status (also controlling for age and gender). Apart from the hopelessness measure, the inclusion of socioeconomic measures explained the elevated rates of the partnered mother and student recipient groups on the psychological and suicidal behaviour measures. In contrast, even after controlling for these socioeconomic covariates, the unemployed, lone mother and NILF groups remained more likely to report all symptoms and suicidal behaviours than non-recipients. The pattern of results is replicated in analysis of the composite demoralization score where, after controlling for age, gender and socioeconomic status, rates of demoralization remained significantly elevated among welfare recipients in the unemployed, lone mother and NILF groups relative to non-recipients.
In the third model, a range of personal characteristics were included (partnered status, number of children, physical health/disability, loneliness, experience of violence, psychiatric disorders). The results across the outcome measures are somewhat inconsistent, though for all measures the inclusion of these covariates accounted for the elevated rates of demoralization, hopelessness and suicidal behaviour within the lone mother recipient group. On measures of suicidal behaviour (12-month ideation and attempts), consideration of the risk factors explained elevated rates in the NILF and unemployed groups. Note, however, that the odds ratio associated with suicide attempts within the unemployed group remains large (2.71), but is non-significant because of the wide confidence intervals. Unlike the suicide measures, the inclusion of individual risk factors did not explain the elevated rates of the unemployed and NILF groups on the three psychological measures (hopelessness, worthlessness and life satisfaction). Effects were reduced but remained significantly higher than non-recipients. Analysis of the composite demoralization score showed a similar pattern, with the unemployed and NILF group showing reduced but still significantly elevated levels of demoralization compared with non-recipients. The covariates which were consistently significant in the full models were age, physical conditions/disability, low educational attainment, loneliness, and experience of anxiety and affective disorders.
Finally, replication of the results of Petterson and Friel would require data on respondent's financial circumstances in addition to information on main source of income. Information on income is not available in the NSMHWB dataset. As a proxy, the analyses were repeated for the subpopulation residing in areas of greatest relative socioeconomic disadvantage. The objective was to reduce heterogeneity and maximize comparability between welfare recipients and nonrecipients on other potentially important characteristics. The effective sample size was considerably smaller resulting in wider confidence intervals, but the analysis produced similar results to those obtained with the full dataset. The main difference was that the rates of demoralization among lone mother recipients was greater and remained significant in analysis of the suicidal ideation, life satisfaction and overall demoralization measures after controlling for socioeconomic and other risk factors.
Discussion
This study examined the relationship between welfare dependence (considering five different categories of income support recipients) and hopelessness, worthlessness, dissatisfaction with life, suicidal ideation and reported suicide attempts. In general, income support recipients were more likely to report these adverse psychological outcomes and suicidal behaviours than nonrecipients, although there were important differences between groups of welfare recipients. Compared with non-recipients, rates on all of the psychological measures were higher among those in the unemployed, lone mother and NILF/disability payment groups. Partnered mother recipients also reported higher rates of these adverse psychological outcomes, although prevalence rates were much lower than in the three previously mentioned groups. Except for the measure of hopelessness, socioeconomic status explained the elevated psychological outcomes reported by partnered mother recipients, while the inclusion of a range of personal risk factors and mental disorders explained the elevated rates of lone mothers. Results were similar for suicide ideation and attempts, although partnered mothers demonstrated no greater prevalence of suicidal behaviour than nonrecipients. The elevated rates of suicide ideation and attempts reported by income support recipients in the unemployed and NILF groups were explained by personal risk factors and mental disorders (particularly poorer physical health, loneliness, affective and anxiety disorders), although the odds ratio representing recent attempted suicide among unemployed recipients was high but non-significant because of large confidence intervals. The results on the composite demoralization scale were consistent with those of the individual psychological measures.
The results show that welfare recipients often feel hopeless, worthless and dissatisfied with life. The demonstration of elevated rates of suicidal ideation and suicide attempts adds to the literature about the personal adversity associated with welfare dependence. While mental disorders are a strong risk factor for suicide, a recent review [28] emphasized factors such as hopelessness (entrenched negative expectations about the future), social isolation and sense of ineffectiveness (learned helplessness, shame and guilt about being an ineffective agent of change in one's own life, and sense of being a burden). Taylor and colleagues showed the important influence of material life circumstances, including receipt of government payments, on suicidal behaviour [17]. Thus, factors such as unemployment, occupational level, low socioeconomic status, incomesupport receipt, poor physical health, poor social support, residing in a rural area and relationship problems are risk factors for suicidal behaviour [17–19,29–33]. Previous research has shown that the categories of welfare recipients that report the greatest level of material and social disadvantage are lone parents, the unemployed and disability pension recipients [11,34]. These are also the groups most affected by the announced reforms. The current results show that these three groups also report significantly elevated rates of suicidal behaviour.
The psychological and suicidal behaviour measures were combined into a composite scale labelled demoralization. Three findings supported this decision: the broad consistency evident across each of the individual outcome measures; the statistical evidence supporting these as measures of the same underlying construct; and the fact that this scale was differentiated from affective disorders (48% of those classified as demoralized did not meet criteria for affective disorder). Thus, in one respect the use of the demoralization measure represents an attempt to parsimoniously analyse the multiple outcome variables. However, the concept of demoralization is also relevant to current welfare reform planning in Australia. Clarke and Kissane discuss demoralization in the context of palliative care/end-of-life decisions and define it as feelings of meaninglessness and pointlessness in life, a lack of personal utility to resolve these feelings, suicidal thoughts, hopelessness and helplessness, a lack of coping mechanisms, feeling trapped within circumstances and being desperate for relief [35,36]. Other literature, often in the context of medical illness, considers demoralization as an inability to meet own or others' expectations and an inability to cope or resolve difficulties [37,38]. de Figueiredo [39,40] outlines two key components of demoralization: general psychological distress and feelings of subjective incompetence.
The concept of demoralization captures the concepts discussed by Mead and Pearson in psychiatric terms, including sense of hopelessness and ineffectiveness. While the goal of welfare reform is to increase participation, welfare recipients who are demoralized may not behave in ways consistent with these policy objectives. Feelings of demoralization may reduce the capacity of individuals to engage in society. For example, Williams
[41] argues that the long-term consequences of feelings of entrapment are reduced and abnormally low aspirations. This may be misinterpreted as a lack of motivation and result in further stigmatization [35,41] and, in the welfare context, increase the risk of administrative sanction or penalty. The links between feelings of incompetence and behaviour require careful consideration in the social policy environment. The role of paternalistic policies (which do not emphasize choice and control on the part of the individual) may counterintuitively reinforce the sense of helplessness identified in this analysis.
The current results show that welfare recipients are among the most psychological vulnerable people and this needs to be considered when evaluating current welfare and social policy. Certainly, social policy reform offers opportunities to change many of the social factors associated with mental illness and suicidal behaviour that cannot be addressed through a focus on the individual [17,19,42], and the psychological benefits of work are well-established [43]. However, the implications at the individual level of elevated levels of demoralization [35,44] and poor mental health need to be considered when implementing a work-first approach. It is imperative that the administrative requirements placed on individuals are sensitive to, and do not exacerbate their current circumstances. We question whether, in general, social policy analysts and employment providers have the knowledge and experience to adequately identify and assist welfare recipients in such circumstances. Customer service staff in welfare offices (Centrelink) and employment service organizations (Job Network) must have appropriate skills and experience to identify and assist income support recipients with these needs. The current research therefore illustrates the importance of involving mental health professionals in welfare and social policy. Kessler [45] argues that psychiatric epidemiology has a key role informing social policy and welfare interventions. It is also important to develop links and partnerships between welfare/employment services and (mental) health professionals.
One unusual finding was the consistently elevated levels of hopelessness reported by partnered mother recipients, even after controlling for socioeconomic status, personal risk factors and psychiatric illness. Women in this category are eligible for payment because of low family income or partner's receipt of income support payments and the results may reflect broader family circumstances. Similarly, the elevated levels of suicidal ideation reported by student recipients, while explained by socioeconomic characteristics, may provide cues for appropriate targeting of intervention strategies.
The argument that welfare reliance causes a loss of mastery, depression and hopelessness [7–9] has been used to support policy responses which emphasize work and mutual obligations among welfare recipients. The current research, however, found that there were significant differences between groups of welfare recipients suggesting that the poor mental health, suicidal behaviour and demoralization were not necessarily a consequence of welfare receipt per se. That is, the partnered mothers and student recipients had different reasons for receiving welfare and different background characteristics and neither group showed elevated rates on any outcome after controlling for socioeconomic status. Further, differences between welfare recipients and non-recipi-ents were largely explained by other characteristics (mental and physical health, partnered status, etc.) rather than simply reflecting welfare receipt (although differences on the psychological measures remained significant for the unemployed and NILF groups). This provides some indication of the need to look more generally at life circumstances that are associated with welfare dependence. For example, Field [46] argues that economic restructuring and the loss of unskilled jobs are the underlying cause of both unemployment and subsequent feelings of hopelessness.
It is important to recognize the limitations of the current research. The stronger effects demonstrated for the 12-month compared with lifetime suicide measures show the relevance of more contemporaneous characteristics such as financial hardship, current housing arrangements or location. Petterson and Friel [20] found that current income rather than background characteristics mediated the relationship between welfare receipt and hopelessness and depressive symptoms. The NSMHWB lacks detailed information on such measures. Therefore, we plan to examine these types of research questions using other datasets. The NSMHWB data are also crosssectional, limiting our ability to expand on the nature of the relationship between the variables examined. While future research can be improved through the use of prospective data collection, a key to improving the policy relevance of research is to focus on modifiable risk factors and assess characteristics relevant for intervention design. Further, we advocate the involvement of psychiatric epidemiologists in the design and evaluation of the ‘natural experiments’ provided by welfare reform. As Kessler argues in the US context, there is a need for the empirical and conceptual input of psychiatric epidemiology in welfare and social policy.
Footnotes
Acknowledgements
Peter Butterworth was supported by NHMRC Public Health (Australia) Fellowship No. 316970. Kaarin Anstey was supported by NHMRC Career Development Award No. 179839. Funding was also provided by NHMRC Program Grant No. 179805.