
Abstract
Objective:
Differences between adolescent self-reported and parent-reported emotional and behavioural difficulties may influence psychiatric epidemiological research. This study examined concordance between adolescents and their parents about mental health symptoms using the Strengths and Difficulties Questionnaire.
Methods:
The study comprised a randomly selected, nationally representative sample of adolescents aged 11–17 years who participated in the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing (N = 2967). Matched adolescent and parent responses across the five Strengths and Difficulties Questionnaire subscales (emotional problems, hyperactivity, peer problems, conduct problems and prosocial behaviour), as well as total difficulties and total impact scores were examined to estimate concordance. Concordance patterns were analysed by sex, after stratifying the sample by age group (younger adolescents: 11–14 years; older adolescents: 15–17 years).
Results:
Concordance was 86.7% for total difficulties, 77.5% for total impact and ranged from 82.4% to 94.3% across the five Strengths and Difficulties Questionnaire subscales. There were no differences in concordance between sexes on the total difficulties score. Older females were more likely to disagree with their parents about emotional problems compared to males of the same age. Younger males were more likely to disagree with their parents compared to same-aged females about peer problems, hyperactivity, conduct problems and prosocial skills, as well as the impact of their problems. Older males were more likely to disagree with their parents about their prosocial skills compared to older females.
Conclusion:
Overall, concordance between adolescents and parents on the Strengths and Difficulties Questionnaire was largely driven by the high proportion of respondents who reported having no problems. Discordance on a subscale increased as the prevalence of problems in a sex and age demographic subgroup increased. These findings highlight the need for a multi-informant approach to detect emotional and behavioural difficulties in adolescents, particularly when assessing the impact of symptoms, as this subscale had the lowest concordance.
Mental disorders are the leading cause of disability in young people (Gore et al., 2011), and elicit significant distress within the family, problematic peer relationships and functional impairment at school (Lawrence et al., 2015; Van Der Meer et al., 2008). Early detection and treatment can minimise disruption to psychosocial development (Martin et al., 2004; Van Der Meer et al., 2008) and prevent persistent mental illness in adulthood (Costello, 2016; Vaz et al., 2016). Psychometric scales are routinely used in epidemiological surveys, schools and primary care settings to assess adolescent mental health problems (World Health Organisation, 2003). A multi-informant approach, usually entailing assessments from parents or caregivers (hereafter referred to as ‘parent/s’) is considered best practice for the detection of emotional and behavioural difficulties in adolescents.
Multi-informant assessment is used to examine the consistency with which young people display difficulties (De Los Reyes et al., 2015; Gaete et al., 2018). However, there is a consistent observation that there is low to moderate concordance between parent and child/adolescent reports (Achenbach et al., 1987; De Los Reyes et al., 2015). Informant discrepancies may indicate reporting bias, measurement error or differences in symptomatology across contexts (De Los Reyes et al., 2009; Vaz et al., 2016). The contemporary view is that each informant provides a valuable perspective by offering unique and meaningful information (De Los Reyes et al., 2015; Van Roy et al., 2010). This is important because it can have implications for clinical decision making and service planning (Becker et al., 2004; Martin et al., 2004; Van Der Meer et al., 2008). In clinical settings where referrals require triage, individuals may need to meet a symptom threshold to be accepted into a tertiary treatment service with limited places. This creates a second challenge as to how to reconcile discrepant assessment information in clinical decision making. As models of care for adolescent mental health continue to evolve, the function of the clinical assessment using standardised tools remains salient in evaluating the mix of services required to appropriately service the mental health needs of adolescent populations.
A detailed understanding of the concordance of reporting mental health problems using screening instruments between adolescent–parent dyads is important for two reasons. First, screening tools are widely used in epidemiological surveys to inform estimates of the prevalence of various mental health conditions (Thombs et al., 2018). Prevalence estimates from epidemiological studies are also used in the subsequent allocation of resources for adolescent mental health care and the associated mix of services (Kessler, 2000). Estimates of concordance inform survey methods and specifically, can help determine if the use of one informant is acceptable or whether both parent and adolescent responses are justified. Second, parents are often the enablers of access to mental health care for young people (Bajeux et al., 2018; Lawrence et al., 2015; Schnyder et al., 2020). An understanding of the discordance between parents and their adolescents in reporting mental health problems informs the needs for programs that improve mental health literacy to support access to appropriate care.
The Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997) screens for common emotional and behavioural problems in children and adolescents. It has robust psychometrics and short administration time (Aebi et al., 2017; Essau et al., 2012; Liu et al., 2013; Warnick et al., 2008). The SDQ consists of 25 items across five subscales: emotional problems, conduct problems, hyperactivity/attention problems, peer problems and prosocial behaviour (Goodman, 1997, 2001). It has three versions to be completed by parents/caregivers, teachers and the young person themselves if aged 11–17 years (Goodman, 2001). In a community sample of adolescents, cross-informant concordance on the SDQ indicated adolescent–parent correlations to be 0.48 for total difficulties and 0.30 for total impact (Goodman, 2001). In the Australian context, there was a moderate to high level of agreement between SDQ generated psychiatric diagnoses and clinical team diagnoses in children aged 4–15 years referred to a community child and adolescent mental health clinic (Kendall’s tau-b = 0.39 for emotional problems, 0.44 for hyperactive problems, 0.56 for conduct problems) (Mathai et al., 2004).
A number of previous studies have examined parent–adolescent concordance regarding adolescent emotional and behavioural problems, many of which use the SDQ. Overall, the level of concordance is similar for internalising subscales (emotional and peer problems, Pearson’s r = 0.25) and the externalising subscales (hyperactivity and conduct problems, Pearson’s r = 0.30) (De Los Reyes et al., 2015). This relatively low positive correlation is thought to reflect the difficulties in parents assessing the internal emotional states of their adolescents for internalising disorders and a lack of awareness of problems for many adolescents with externalising problems (De Los Reyes et al., 2015; Van Der Meer et al., 2008).
There is variation in the concordance between parents and their male and female adolescents. A cross-sectional study of Dutch children aged 11–19 years using the Child Behaviour Checklist (CBCL) and Youth Self-Report (YSR) found lower concordance among females for internalising problems compared to males, though adolescents overall endorsed more internalising problems than their parents. The same study found no difference between sexes for externalising problems (Verhulst and Van Der Ende, 1992). An Australian study of a clinical sample that used the SDQ found that compared to males, female adolescents were more likely to agree with their parents about not experiencing emotional and behavioural problems, though they were also more likely to be the only informant endorsing problems. In contrast, males were more likely to agree with their parents about having problems or have parents only endorse problems (Van Der Meer et al., 2008).
Studies that have examined the effect of age on adolescent–parent concordance on mental health symptom measures have produced somewhat inconsistent findings. The general trend has been a reduction in concordance as adolescents age (Achenbach et al., 1987; Verhulst and Van Der Ende, 1992). This is consistent with the adolescent developmental period of individuation whereby young people become increasingly autonomous from their parents and there is an appropriate reduction in parental knowledge of their adolescent’s emotions and behaviours (Blos, 1979). A large meta-analysis found no significant effect of age on levels of concordance between children (<11 years) and adolescents aged 11 years and older (De Los Reyes et al., 2015). However, this study incorporated a number of different measures including but not limited to the SDQ across a wide range of ages. The study also included comparisons of pairs of parents, teachers, and/or older children and adolescents. Both of these factors may have potentially masked an age effect. The lack of association between age and concordance was explained as a likely result of the increased take-up of including self-report assessments by both older children and adolescents in more recent years (De Los Reyes et al., 2015).
In the Australian context, there are limited data on parent–child concordance on the SDQ, restricted to small studies of clinical samples (ages 11–18 years, n = 379 [Van Der Meer et al., 2008]; ages 14–18 years, n = 119 [Wahlin and Deane, 2012]). In addressing this gap, the objective of the current study was to examine adolescent–parent concordance on the SDQ using data from a nationally representative community sample of Australian adolescents. This study aimed to investigate the effects of sex and age on concordance, as well as the nature of the discordant groups (problems endorsed by parent or adolescent only). It was hypothesised that there would be lower levels of concordance among male adolescents regarding externalising problems, owing to parents reporting more problems than adolescent males. Another hypothesis was that there would be lower levels of concordance among female adolescents regarding internalising problems, owing to more adolescent females reporting more problems than their parents. Given the individuation that occurs during adolescent development, we hypothesised that concordance would be inversely associated with adolescent age, such that concordance will be lower among older compared to younger adolescents.
Method
Participants and procedure
The sample was drawn from parents and adolescents who participated in the Second Australian Child and Adolescent Survey of Mental Health and Wellbeing, known as the Young Minds Matter Survey (Hafekost et al., 2016; Lawrence et al., 2015). The survey was conducted between June 2013 and April 2014. Area-based sampling was used to randomly select households that accommodated at least one young person aged 4–17 years. Trained interviewers conducted face-to-face interviews with a parent or carer. In households where the young person was aged 11–17 years, the young person was invited to complete a questionnaire on a tablet computer. A single participant was randomly selected if there was more than one eligible participant residing in the household.
In total, 6310 parents (55%) from eligible households agreed to provide information about the randomly selected child. Of the 3334 adolescents aged 11–17 years whose parents or carers were interviewed, 2967 (89%; mean age = 14.6; 51.6% male) also agreed to complete the adolescent questionnaire. A detailed research methodology has been published (Hafekost et al., 2016). Further analyses indicated that the sample was representative of the Australian population aged 4–17 years based on sex, age, family type, household income, socio-economic index and parental employment.
Ethical approval for the original Young Minds Matters Survey research protocol was provided by the Australian Government Department of Health Human Research Ethics Committee (HREC) and The University of Western Australia HREC. An exemption for the use of the de-identified data for further research was provided by The University of Queensland HREC. All participants in the survey provided informed written consent.
Availability of data and materials
The authors applied for access to the Confidentialised Unit Record File (CURF) to obtain the relevant data files from the Australian Data Archives, who oversee the access, use and publication of data generated by the Young Minds Matter Survey.
Measures
Self-reported and parent-reported emotional and behavioural difficulties
The SDQ is a well-validated screening instrument that assesses emotional and behavioural difficulties in young people (Goodman, 1997). Adolescent participants completed the self-reported version and a parent completed the parent-reported version of the instrument. The SDQ uses a 3-point response scale (0 = not true; 1 = somewhat true; 2 = certainly true) to measure both positive and negative traits across five subscales: emotional problems, conduct problems, peer problems, hyperactivity and prosocial behaviour. Five items across the negative trait scales are reverse scored. Four of the subscales (excluding prosocial behaviour) are summed to form a total difficulties score ranging from 0 to 40. There are a further five items used to assess the overall level of distress and impairment caused by emotional or behavioural difficulties, summed to make a total impact score ranging from 0 to 10. Summed scores for all subscales were classified using the three-band categorisation of ‘normal’, ‘borderline’ and ‘abnormal’. Cut-off scores for these bands were defined by a population-based UK survey so that approximately 80% of adolescents score ‘normal’, 10% ‘borderline’ and 10% ‘abnormal’ (Goodman, 1997; Goodman et al., 1998).
Adolescent–parent concordance on SDQ
Various coding schemes were considered in determining concordance using the ‘normal’, ‘borderline’ or ‘abnormal’ groupings. Combining ‘normal’ with ‘borderline’ scores is consistent with previous methodologies used to examine concordance between adolescents and parents on the SDQ (Martin et al., 2004; Van Der Meer et al., 2008). A four-category coding system was established as it was thought to have the highest clinical relevance. Adolescent–parent dyads were categorised as ‘
Statistical analysis
Analyses were performed using IBM SPSS Statistics, Version 25. Data were weighted to represent the Australian population of adolescents aged 11–17 years, accounting for sex, age, family size and household income (Hafekost et al., 2016). In the first set of analyses, proportion of agreement was used to estimate the concordance between adolescent and parent scores across the five subscales and two summary scales of the SDQ. Traditionally, studies have employed Cohen’s Kappa to measure overall concordance; however, this measure is dependent on prevalence, even when sensitivity and specificity remain constant (Kessler et al., 2004). Cohen’s Kappa statistic may be low even when there appears to be high agreement among low prevalence measures (Feinstein and Cicchetti, 1990). Similarly, there may be a high proportion of concordance between informants, even if there is no relationship between the two measures. An alternative and preferred measure of overall classification accuracy is the area under the receiver operator characteristic curve (AUC). In the case of a dichotomous predictor and dichotomous outcome, AUC = (Sensitivity + Specificity) / 2, which can be interpreted as the probability that a randomly selected clinical case will score in the ‘Abnormal’ range on an SDQ subscale, than a randomly selected non-case (Kessler et al., 2004). In addition to estimating the proportion of concordant adolescent–parent dyads, we also examined the prevalence of abnormal scores on SDQ subscales (adolescent-reported and parent-reported), as well as AUC.
Participants were then grouped into ‘younger adolescents’ (aged 11–14 years) and ‘older adolescents’ (15–17 years). Binomial logistic regression analyses were used to examine the association between concordance and sex, stratifying by age group. In the second set of analyses, adolescent–parent dyads were further disaggregated into four categories to examine concordance/discordance based on the presence/absence of problems on each subscale: ‘
Results
Internal consistency of subscales and overall concordance based on two-way grouping
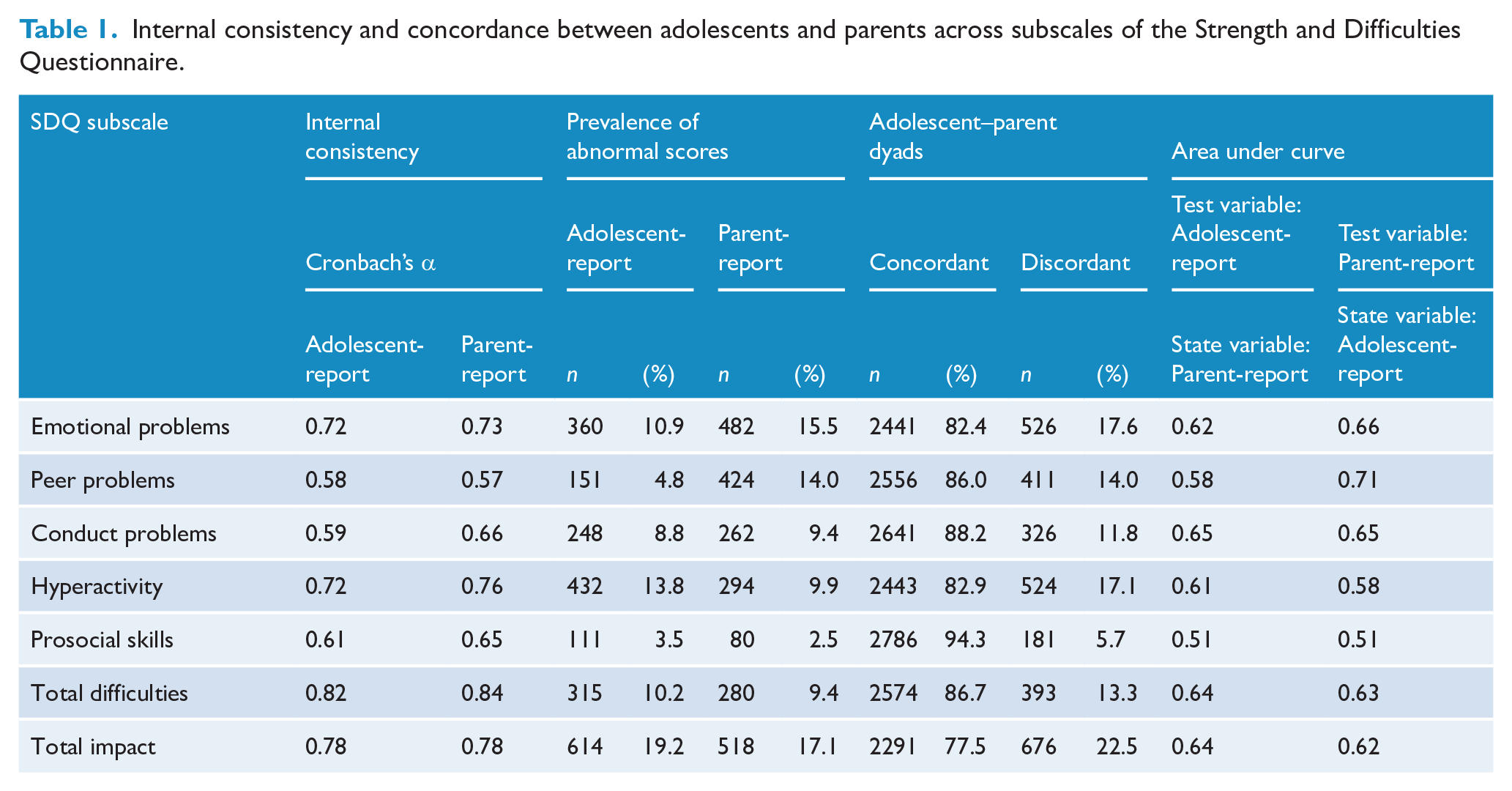
The internal consistency of each of the SDQ subscales for both adolescent-report and parent-report versions are presented in Table 1. Overall, Cronbach’s alpha statistics indicated that the five items on each of the emotional problems, hyperactivity, total difficulties and total impact scales had good reliability (α ⩾ 0.7). The internal consistency of the five items on the peer problems, conduct problems and prosocial skills subscales had weaker reliability indices (α = 0.58–0.66). The prevalence of abnormal scores on the SDQ subscales as reported by adolescents and parents are also presented in Table 1. The overall level of concordance between adolescents and their parents on the SDQ was > 82% on all subscales except for the total impact score (77.2%) (Table 1). Adolescent–parent dyads had the highest level of concordance on the prosocial skills subscale (93.9%).
Internal consistency and concordance between adolescents and parents across subscales of the Strength and Difficulties Questionnaire.
Demographic characteristics of the reporting parent and family context
Most commonly, the reporting parent was female (82.8%) and the adolescent was their biological offspring (95.8%). Female parents reported on a similar proportion of female and male adolescents (40.7% and 42.2%, respectively), and male parents reported on a similar proportion of female and male adolescents (8.1% and 9.1%, respectively) in the sample. The majority of adolescent–parent dyads comprised an intact family (64.1% – two biological parents reside), 22.8% were a single parent family, 12.1% were a step or blended family, and 1% had other family living arrangements.
Effect of age and sex on overall concordance
Older female adolescents were more likely than older male adolescents to disagree with their parent on their emotional problems (Table 2). Male adolescents irrespective of age were more likely than female adolescents to disagree with their parents about their prosocial skills. Younger male adolescents were more likely than younger female adolescents to disagree with their parents about their peer problems, hyperactivity, conduct problems and the total impact of problems. For both age groups, there were no significant differences between sexes on the total difficulties scores, based on the overall two-way grouping.
Concordance between adolescents and parents across the Strength and Difficulties Questionnaire subscales stratified by age and sex.
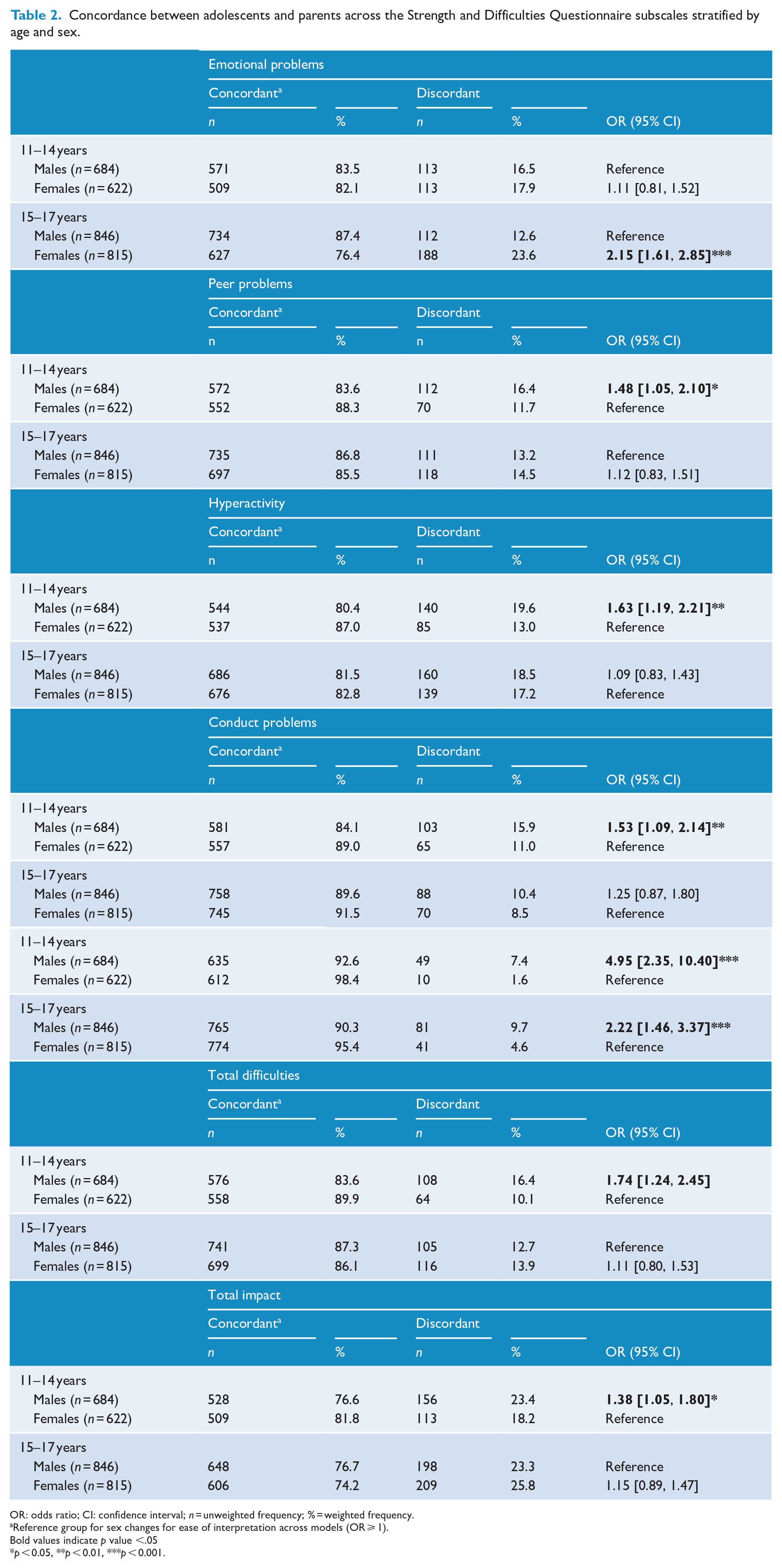
OR: odds ratio; CI: confidence interval; n = unweighted frequency; % = weighted frequency.
Reference group for sex changes for ease of interpretation across models (OR ⩾ 1).
Bold values indicate p value <.05
p < 0.05, **p < 0.01, ***p < 0.001.
There was a significant association between parent sex and concordance for conduct problems, such that female parents had higher odds of being in the discordant dyad group (odds ratio [OR] 1.66, 95% confidence interval [CI] [1.16, 2.37]). There was no association between parent sex and concordance on all other subscales. There was a significant pattern of association between family type and discordance on all SDQ subscales, except prosocial problems. On five out of six subscales (all except prosocial behaviour), those residing in non-intact families had significantly higher odds of being in the discordant dyad group. In a series of follow-up analyses, family type, age group and sex were entered into a multivariate model predicting overall concordance/discordance. Family type remained a significant predictor on all SDQ subscales, except hyperactivity and prosocial behaviour. Sex remained a significant predictor on all subscales, except emotional problems. Age group remained significantly associated with concordance/discordance for conduct problems and prosocial behaviour, and there was no longer an association with age group on the other SDQ subscales, after controlling for sex and family type.
Nature of concordance/discordance based on four-way grouping
The concordant group was further categorised into ‘
Concordance between adolescents and their parents across the Strength and Difficulties Questionnaire subscales utilising four categories of concordance.
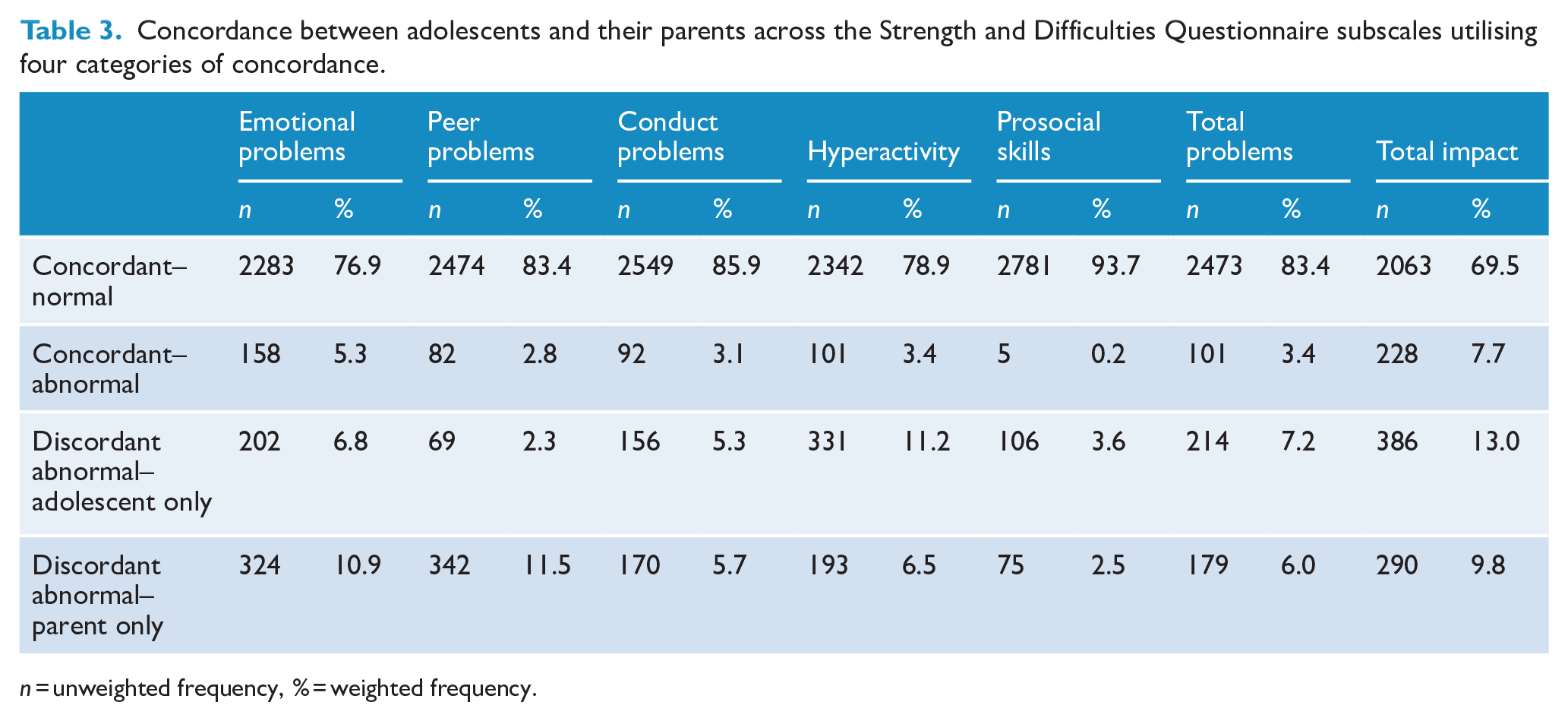
n = unweighted frequency, % = weighted frequency.
Effect of age and sex on the nature of the concordant/discordant groups
The four concordant/discordant groups were stratified by age group in order to examine the association with sex for each of the SDQ subscales (Table 4). When comparing the two concordant groups, females in both age groups were more likely than males to have emotional problems within the abnormal range. Older females were more likely to fall within the abnormal group for both total difficulties and total impact, compared to older males. There was a relatively similar pattern of results found when the discordant groups were examined. Older females were more likely than older males to be the only respondent to have scores in the abnormal range on the emotional problems and peer problems scales. Irrespective of age, females overall were also more likely than males to report abnormal total difficulties and total impact scores than their parents.
Concordance between adolescents and their parents across the Strength and Difficulties Questionnaire subscales utilising four categories of concordance and stratified by age and sex.
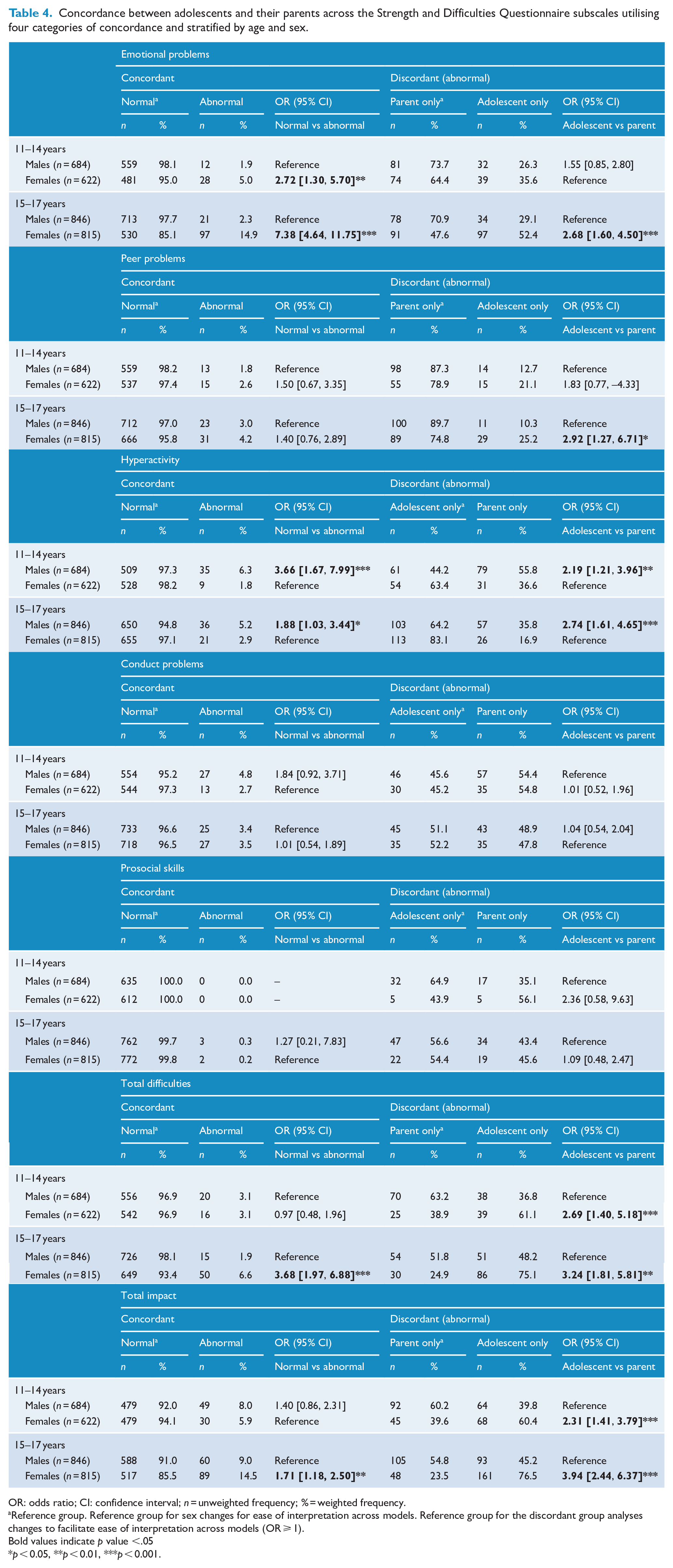
OR: odds ratio; CI: confidence interval; n = unweighted frequency; % = weighted frequency.
Reference group. Reference group for sex changes for ease of interpretation across models. Reference group for the discordant group analyses changes to facilitate ease of interpretation across models (OR ⩾ 1).
Bold values indicate p value <.05
p < 0.05, **p < 0.01, ***p < 0.001.
When comparing the two concordant groups, males in both age groups were more likely than females to have hyperactivity problems within the abnormal range. When the two discordant groups were further examined, males of both ages were more likely than females to have parents who reported abnormal hyperactivity problems. All of the other sub-group analyses showed non-significant results. In the concordant group analyses, there was no association between sex and peer problems, conduct problems, and prosocial problems, stratifying by age group. Among the discordant group analyses, there was no association between sex and conduct problems, hyperactivity, or prosocial skills, stratifying by age group.
Discussion
To the best of our knowledge, this study is the first to report the level of concordance between adolescent–parent dyads on the SDQ using an Australian nationally representative sample. Overall concordance was greater than 82% across the five core subscales. Concordance on the prosocial skills subscale was 93.9%, due to the large numbers of dyads who agreed that there were no problems present in this area. This overall level of concordance supports the use of the SDQ as a screening instrument for emotional and behavioural problems in adolescents, but it also highlights that there is some discordance when using the SDQ as an assessment tool which rises as the prevalence of problems in a sex and age demographic increases.
Researchers have commonly attributed discordance to a variety of factors including differences in developing cognitive abilities with age, and social desirability concerns on the part of the adolescent. This is due to a relative under-reporting via self-reports compared with adult reports on some subscales (De Los Reyes et al., 2015). However, studies have also found support for the internal validity of self-reports (Becker et al., 2004). Consequently, a previously proposed recommendation was that mental health professionals independently evaluate whether cognitive abilities or social desirability are impacting discordance between informants (De Los Reyes et al., 2015). While these factors can often be considered in clinical practice, they are challenging to assess in epidemiological studies. Building on previous studies, the current study highlights the importance of gathering self-report data, for the reason that there is a cohort of adolescents who endorse clinically significant problems that their parents do not recognise. While this has impacts in clinical settings, this challenge also has flow-on effects for estimating the prevalence of problems in epidemiological studies.
The current study found concordance was lower for total impact (77.2%) than for total difficulties (86.6%), which is consistent with another large community study of children aged 10–13 years (Van Roy et al., 2010). In particular, the current study found that older females were more likely to endorse abnormal total impact scores when their parents did not, and older males were more likely
Two of the findings from the current study suggest that there are likely lower levels of concordance among clinical populations compared to the general community. First, the concordance for total difficulties was higher than that reported previously in an Australian clinical sample (86.6% in current study vs 68.6% in Van Der Meer et al., 2008). Second, in the current study, for all subscales where there was a score in the ‘
There were a number of significant sex and age differences observed in this study. When comparing sexes of the same age group, older female adolescents (15–17 years) were more likely than same aged males to experience emotional problems regardless of who endorsed those problems. Older females were also more likely to report emotional problems and peer problems, when their parents did not. Females in both age groups were more likely than males to be the only one in the dyad endorsing abnormal total difficulties and total impact. Overall, younger male adolescents (11–14 years) were more likely to disagree with their parents about peer problems, hyperactivity, conduct problems, prosocial skills and their total impact, compared to younger females. Males of both age groups were more likely to report abnormal hyperactivity than females, and their parents were more likely to endorse hyperactivity problems when the adolescent did not. It is possible that this difference reflects a decreased self-awareness of emotional and behavioural symptoms in adolescent males, particularly for externalising problems or differences in social desirability concerns. While previous studies have reported mixed findings regarding sex and age differences (De Los Reyes et al., 2015; Van Der Meer et al., 2008), the current study examined these hypotheses in a nationally representative sample, and these results are specific to the SDQ and with adolescents aged 11–17 years.
The additional multivariate analysis revealed an association between non-intact family type and discordance on most of the SDQ subscales even when controlled for age group and sex. Perhaps this is a consequence of the reporting parent having less than full-time contact with the adolescent. This result is consistent with findings that recognise the higher prevalence of mental disorders in young people from step, blended or one-parent families (Lawrence et al., 2015).
Implications
The current study has demonstrated the level of agreement between adolescent–parent dyads across the subscales of the SDQ and provided detailed analyses of dyads who reported discrepant information. The first important consideration is that epidemiological surveys which rely on a sole informant will likely underestimate the prevalence of mental health problems in a population. This risks leading to an under-allocation of resources necessary to service the needs of a population. The second is that parents are usually responsible for initiating access to mental health services, so it is important to recognise that discordant adolescents who endorse problems are at greater risk of being overlooked and underserved (Martin et al., 2004). There may be valid reasons why parents and adolescents diverge in their ratings on the SDQ. Not all adolescents may be comfortable discussing concerns about emotional and/or behavioural difficulties with their parents. Beyond sex and age differences, it is plausible that in situations where family functioning is poor or where relationship difficulties between an adolescent and parent is a major contributor to the young person’s emotional or behavioural problems, it would be reasonable to expect disagreement. In Australia, the national youth mental health care service model ‘Headspace’ was established to allow for young people to seek help independently of their parents if necessary (Rickwood et al., 2019). Taken together, the current findings highlight the need for continued efforts to increase help-seeking among adolescents and provide support for mental health literacy programs which aim to teach young people and their parents how to identify mental health problems and empower them to seek help for themselves or their friends.
The general pattern of findings of the current study seemed to support the notion that females were more likely to report problems when their parent did not, whereas the parents of males were more likely to report problems than the male adolescents themselves. These results are broadly consistent with the findings of previous studies (Van Der Meer et al., 2008; Verhulst and Van Der Ende, 1992). It is possible that this sex difference may also contribute to the sex differences in help-seeking behaviour for mental health problems, in general. Some evidence suggests, however, that sex plays a significant, but not exclusive role in the inclination to seek professional help for mental health problems among youth (Haavik et al., 2019). These authors found that compared to males, females were better at identifying certain psychological problems and had greater awareness of mental health services, though they perceived more barriers to seeking help. This previous study also acknowledged that parents play a role in accessing mental health support for their adolescent. Specifically, these researchers found that lower parent education is associated with less help-seeking for mental health problems on behalf of their children (Haavik et al., 2019). In addition, from a socio-cultural perspective, it is possible that the sex difference in adolescent–parent discordance on the SDQ also relates to the way that parents recognise mental health problems in their adolescents. For both male and female adolescents clinically, it may be helpful to further examine how parents are provided information to recognise mental health problems, support their adolescents, and encourage help-seeking and timely access to appropriate treatment. In summary, the sex difference found in the current study regarding patterns of discordance between adolescent–parent dyads, likely has a range of influencing factors and explanations.
Limitations and future directions
Although this study is valuable due to its large, nationally representative community sample and provision of clinically relevant information about the level and direction of concordance, there are some limitations. The Young Minds Matter survey had a modest household participation rate (55%) which is similar to other Australian epidemiological studies (Slade et al., 2009). Statistical analysis of demographics suggested the sample was nonetheless representative of Australian 11- to 17-year-olds (89% of eligible adolescents participated) (Hafekost et al., 2016). The results of the current study would not be generalisable to younger age groups where patterns of concordance may be different given that self-report is not typically used. While the AUC approach has strengths over the Kappa statistic, a limitation of this method of calculating classification accuracy is that it places equal weight on sensitivity and specificity. Screening instruments such as the SDQ may be used for different purposes and in different contexts, and the implications of misclassification will be context dependent. Finally, there is no clinical validation of the individual SDQ results in the current study. Therefore, identifying informant discordance does not indicate which informant has greatest validity. It is suggested that a more valuable approach may be to consider an adolescent to be at risk of having a problem if either the parent or adolescent report falls within the clinical range, and that either situation could give rise to service use. Further studies into additional factors that may predict discrepancies would also assist in identifying adolescents most at risk of underreported problems. We also suggest that a clinical calibration study of the SDQ and the Diagnostic and Statistical Manual of Mental Disorders, Fifth edition (DSM-V) diagnoses would help to tease apart random measurement error from systemic error (e.g. informant bias).
Conclusion
The current study reported a high level of adolescent–parent concordance on the SDQ in an Australian nationally representative sample of 11- to 17-year-olds. However, there was discordance in about one in seven adolescent–parent dyads. Age and sex differences were observed, with the largest discordance occurring in relation to emotional issues in older females and hyperactivity in adolescent males of all ages. Generally, discordance was greatest when problems were present. This finding supports the need for a multi-informant approach to assess the population prevalence of emotional and behavioural problems in adolescents in epidemiological studies. Information from both the adolescent and their parent will more accurately inform the appropriate allocation of resources for adolescent mental health services.
Footnotes
Acknowledgements
The authors wish to thank Roy Morgan Research and the interview team for their work on the YMM survey, as well as the families who participated.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: James Scott is supported by a National Health and Medical Research Council Practitioner Fellowship (Grant 1105807). Hannah Thomas is supported by the Queensland Centre for Mental Health Research, which receives funding from the Queensland Department of Health.