
Abstract
This is the second of two papers that bring anthropological perspectives to focus on the meaning of community, as it is understood within mental health. Both papers are based on an ethnographic analysis of an emergency community mental health service that we have called the Crisis and Assessment Service (CAS). The first paper drew on two areas of anthropological theory concerned with summarizing symbols and boundary work. We adopted the convention of italicizing the term community when we were referring to it as a summarizing symbol, and continue the convention here. By examining a boundary identified by CAS workers themselves, the boundary between hospital and community, the first paper demonstrated that community stood for a cluster of social values that included autonomy, responsibility, integration and progress.
The analysis is extended here by drawing additionally on social network theory, an anthropological approach to the study of human groupings. This theory directs attention to another boundary, the boundary between community mental health professionals and the community in which they work. At this boundary community accrues additional values pertaining to professional conduct, con- fidentiality and privacy.
In the first paper we showed how the symbolism of community and its values applied equally to the community mental health service and the community it served, and united these two in opposition to institutional ways of thinking. In this paper we will show how the values associated with community served to separate members of a community mental health service from the community.
The boundary between professional and community
As we have shown in our companion paper, the organizational question of how the community related to the hospital was a major focus of the CAS service. It exerted an influence at all levels: service development, the deployment of staff, and the day-to-day clinical routine. It also surfaced in the many informal discussions between CAS workers that punctuated this routine. Equally important was the question regarding CAS workers' professional relationship with their clients and other community members. It surfaced in clinical meetings and, again, in the informal talk we observed among CAS workers. The question was brought into sharpest focus by what were termed ‘boundary violations’, transgressions of the professional–client relationship in which community mental health workers became personally involved with their clients.
It is of note that no fiagrant boundary violations came to light during the period of this study. We were struck therefore by the volume of ethnographic data we gathered in the form of stories of sexual boundary violations that were told and retold. These were semiapocryphal in nature, vague in detail and implicitly didactic in intent (‘Do not do this!’). They always pertained to the behaviour of other unnamed staff from other unnamed regions.
More commonly, the issue of the professional–client boundary arose during clinical meetings. In this context, it was not a matter of fiagrant breeches of professional conduct, but the very earliest suggestion that a worker may be a little ‘over involved’. Very often it fell to Geoff Freeman, the Team Leader, to gently rein in the CAS worker, and thereby underscore the boundary. During one meeting, a CAS worker set out his management plan, which included visiting the client the following Thursday. Geoff's response was: ‘You don't need to see her. Ring her instead and see how she's going.’ These brief exchanges were pre-emptive in nature and, like the apocryphal stories, didactic in intent.
During the period of our ethnographic study, a member of CAS conducted a questionnaire-based research project into mental health workers' attitudes to ‘ethical boundaries’ [1]. This body of work was a rich source of ethnographic data for us for several reasons. The research was formulated by a member of CAS. The way it was conceptualized reflected CAS thinking and practice. The responses to the questionnaire came from community mental health workers, CAS workers among them. Finally, it stimulated debate among these same CAS workers about ethical boundaries, and this constituted further observational data for us. In the discussion that follows therefore we examine this research from an anthropological perspective.
The questionnaire comprised a number of scenarios involving individual-to-individual professional–client interactions. Each had an ethical dimension. They ranged from what the author regarded as a fiagrant boundary violation (sexual activity), to situations that were posed as ethically ambiguous. An example of the latter was:
You visit a newly referred client at his home to assess him for his suitability for case management. Upon greeting you he extends his hand to shake your hand in the standard manner. Do you avoid shaking his hand whilst introducing yourself?
Two hundred and thirty-two health professionals employed at the Royal Prince Andrew Hospital (RPA) Community Mental Health Services and corresponding regional services in the state were asked to describe what they would do in these situations. As anticipated, all workers agreed: sexual activity with a client was forbidden. However, responses to other scenarios, such as the acceptance of gifts, were diverse, with interesting variations, for instance, by gender (women having a more liberal attitude to sending Christmas cards).
Exclusion from the client in the community
From an anthropological perspective, the questionnaire illustrates the extent to which the researcher and fellow CAS workers implicitly conceived of interpersonal relationships in terms of exchange. In fact all scenarios depicted forms of exchange between a mental health professional and a client. Some took the form of economic exchange, in degrees of increasing monetary value (from accepting payment for ‘homemade strawberry jam;’ lending one's own money to help with an overdue electricity bill, to accepting expensive gifts such as a digital camera). Others concerned exchanges that signify relationships of personal affinity, these in degrees of increasing intimacy (from shaking hands, sending a greeting card; lunch at your favourite cafe, giving out your home telephone number, going to a movie, to bodily–cum–emotional interactions such as hugging a grieving client as a gesture of condolence or having sex with them). Structuring the questions, the responses and the research findings was the idea that at a certain point along a scale of increasing monetary exchange one could cross the boundary from a professional to a personal relationship with one's client. Similarly along a scale of increasing intimacy there was a point at which the boundary was crossed. Precisely where the boundaries were located on these two scales varied from one context to another, one client to another and one mental health professional to another. But beyond them lay exchanges of a monetary and intimate nature that form the substrate of a human community. Excluded from these relationships by rules of professional conduct, mental health professionals are thereby excluded from basic forms of exchange that form the community they serve.
Another way of viewing this is to array the scenarios in the questionnaire on a scale based on the length of time that elapses till the exchange is complete. At one end of this scale are the formalities of interaction ritual [2] such as the handshake, completed in an instant, where there is little enduring obligation after two hands part. They fall into a category of what Mauss [3] has called balanced reciprocity. Of themselves, they anticipate no enduring relationship. Other transactions herald the development of a longer-term relationship through the social obligations of delayed reciprocity. They establish a perpetual state of imbalance (at any point in time, one or the other party is obliged to return the favour). These are the currency of everyday life; they consolidate what we recognize as an ongoing relationship. Examples include a loan that explicitly entails repayment, a gift that implicitly anticipates a response in kind, a sexual tryst that serves as an invitation to romance, or a romantic frisson that serves as an invitation to sex. All form the transactional cement of enduring social bonds.
Transactions of balanced reciprocity that effect immediate closure tended to be regarded by the respondents to the questionnaire as acceptable. Forbidden were the transactions of delayed reciprocity; those that invited an enduring exchange, be they economic transactions (lending money which anticipates repayment) or activities that signified interpersonal affinity (going to a movie, which might anticipate further socializing down the track). In short, personal involvement of mental health professionals with their community clients tended to be more acceptable if time-limited.
That is to say, CAS workers and their rules of professional conduct excluded themselves from forms of exchange that establish enduring personal bonds. Yet it is these continuing bonds that sustain a community over time. Crisis and Assessment Service workers thereby excluded themselves from the community they serve.
In our companion paper, we showed how, at a broader organizational level, community functioned as a summarizing symbol, and we showed that it stood for a cluster of values that the community service shared with members of the community, in opposition to the hospital. In this paper, by focusing down to the interpersonal level of professional–client relationships, we show that community incorporates additional values of continuity, reciprocity and intimacy, values which separate the community service from its community.
It is important to note that mental health professionals are involved in reciprocal exchange with their clients. However, these exchanges fall within the remit of clinical protocols and professional standards, no different to those that apply within a hospital setting. They are not the exchanges we have outlined above. Second, it must be emphasized that the notion of a community as comprising enduring reciprocal interpersonal bonds is an idealization (for example it does not address conflict). This is why we identify it as community, a summarizing symbol.
Exclusion from community as a network
With its focus on the individual professional interacting with the individual client, the questionnaire research did not take into account the client's primary network, an attribute of community that has been extensively researched by anthropologists under the rubric of ‘social network’ studies [4, 5]. At the core of the social network lies the primary network, a small cluster of people surrounding an individual, who interact primarily with the individual. These clusters, in turn, are loosely related to each other to form an extended social network. Within this genre of anthropological theory, the notion of loosely interconnecting clusters of people is paradigmatic of a community.
Studies of ordinary primary networks indicate that it is the secondary interactions between the people around the individual that provide for the stability and endurance of the primary network, and provide a solid structure of emotional support for that individual. This is represented schematically in Fig. 1a. If an individual, I, has primary social relationships with W, X, Y and Z, then it is the cross-cutting relationships between W, X, Y and Z that render I's network stable. The critical characteristic here is density, defined as ‘the extent to which the individuals connected to a focal individual are also connected to each other’ [6]. The denser these second-order interconnections, the more robust and long-lasting the network. Support in these interconnecting networks is typically bidirectional.
(a) ‘Normal’ primary network; (b) client's primary network; and (c) the relationship of the community mental health professional to the client's network.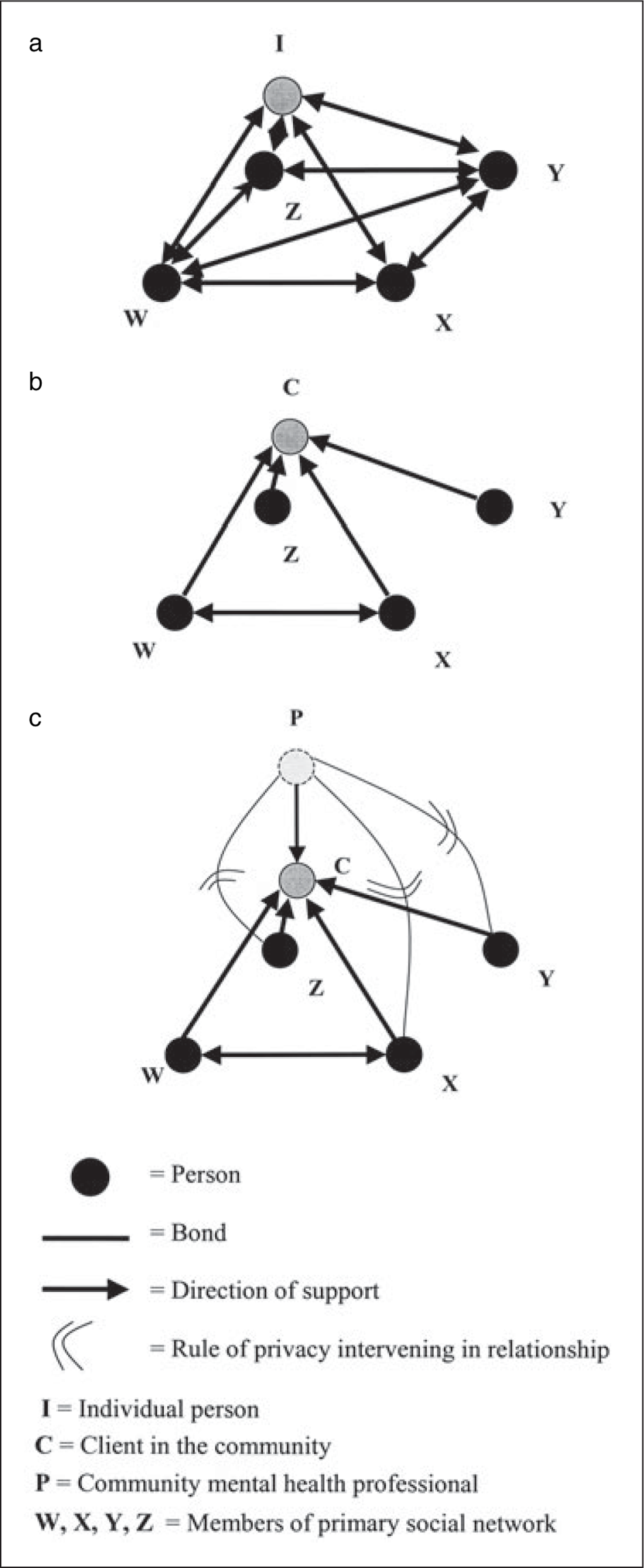
There is a considerable body of research into the social networks of people with schizophrenia [7, 8]. Hammer's review of this work suggests that their networks are characterized by ‘virtually no clustering and mainly a scattering of individuals’ [6, 9]. In Fig. 1b, the person with schizophrenia is represented as a client, C. Most members of C's network do not know each other. Support largely flows from network members to C.
This literature provides additional insights into the boundary between mental health professionals and the primary network members that surround their clients. When a community mental health professional, represented in Fig. 1c as P, forms a relationship with a client, C, then P is prevented by rules of confidentiality from revealing details of C's illness to W, X, Y and Z (say, the client's sister, drug supplier, next-door neighbour, local milk-bar owner). This prevents P from becoming part of C's primary network. Moreover, it largely precludes the possibility of enhancing those second-order interconnections that are lacking, and thereby knitting together and reinforcing the structure of the network.
Crisis and Assessment Service workers would at times interact with select members of the primary network. They would engage, for instance, with a client's mother or house-mate. They would also routinely involve other people who were part of the client's immediate professional network (the general practitioner, a housing authority officer, the social worker representing the Public Trustee). However, all forms of involvement, be they with lay or professional people, focused exclusively on the first-order relationship between the client and that person, never dealing with second-order relationships between network members. It would be unethical to suggest to a next-door neighbour that he ‘touch base’ with the client's mother to help her keep an eye on things. From time to time, the involvement of CAS workers began to focus too much on members of a client's network. When this became apparent during case discussions at clinical meetings, Geoff Freeman would typically redirect them by asking: ‘Who is our client here?’
We observed that when CAS workers did engage with primary network members, it was usually with family or friends who lived in the same house as the client, especially if they were present during clinical encounters there. Even so, CAS workers were careful to ensure that there was opportunity for confidential communication with the client, ‘one-on-one’, without the presence of others. The principle of shared domicile, as limited as it was, thus took precedence over the principle of relatedness. Those who did not reside with the client were less commonly involved, even if they had strong family ties or were close friends.
In cutting themselves off by rules of confidentiality and privacy from engaging with networks as a whole, CAS workers were cutting themselves off from the community they served. In doing so they defined the community as an information zone where privacy and confidentiality were not governed by professionally defined rules. Here information about people flows back and forth and around, guided by more loosely defined notions of legitimate interest, family sharing or neighbourhood gossip. This is an ideal of a community as a place where people take an interest in one another, where people make it their business to know the business of others. The small Australian country town is often used to illustrate this ideal. In this sense, the symbol of community gathers up values of shared interest and shared knowledge.
Moving beyond the confines of the home, CAS workers scarcely ever engaged with neighbours. This is not to say that they would refuse to talk to neighbours who approached them, but they had no mandate to door-knock or discuss a client with his or her neighbours – privacy legislation made this illegal. Crisis and Assessment Service workers were effectively excluded from interacting with the neighbourhood. Thus, concepts of neighbourhood or geographical locale, long regarded by demographers as primary units of community, had no purchase in the delivery of community mental health services. This may help explain why the contemporary banner of ‘social capital’, beneath which policy makers at local government level have sought to enhance the capacity of neighbourhoods to support themselves [9], has never been a strong part of community mental health policy. In fact, neighbourhood and geographical locale were conspicuously absent from state-level mental health service planning. Service divisions within the state amounted to arbitrary lines drawn on a metropolitan map from an office high on one of the topmost floors of the health department. Cutting through suburbs, dividing one side of the street from the other, these lines bore a family resemblance to the lines drawn over Africa by the European colonial powers.
Conclusion
In our first paper, we showed how the summarizing symbol community was appropriated by the CAS service when engaged in organizational boundary work that defined their community service and the people they served in opposition to the hospital. Here, community stood for openness, freedom, responsibility, integration, autonomy, progress and development. Even when through a counter-narrative, CAS workers appeared critical of their community service, they nonetheless fell back on community when they transferred some of its attendant values on to a halcyon image of the asylum. The community–hospital boundary, we showed, was the principal site at which new developments in mental health took place. It was here that innovative clinicians and influential managers invoked community in the process of developing and reconfiguring the service in ever new ways.
In this second paper, we have shown how community was appropriated by the CAS service when engaged in professional boundary work that defined the relationship between CAS and the community it served. Here community accrued additional values of continuity, reciprocity, intimacy, shared interest and shared knowledge. These values were projected onto the client and their network, not the service itself.
By employing ethnographic methodology, and by focusing on symbol and value, the research on which these two papers are based has been able to offer a more rigorous definition of community than previous work in this area. By rigorous, we do not mean clear-cut – we offer no strict inclusion or exclusion criteria. This is because, as a symbol, community stands for a variety of values and, as we have shown, is invoked in a variety of circumstances. It is in the nature of symbols that their attendant values are not always neatly organized and consistent [4, 10]. They may, in fact, be logically contradictory. But even when invoked in logically contradictory ways symbols nonetheless carry conviction, transcending and summating these inconsistencies. In the first paper we showed how community simultaneously carried values of freedom and integration, and that these two stood in potential contradiction to each other (a comprehensive integrated service compromised individual liberty and freedom). The additional values that we have identified in this second paper create the possibility of yet additional inconsistencies: autonomy versus shared knowledge, progress versus continuity. It is possible therefore for competing organizational interests and agendas to run under the self same banner: community. We have shown how proponents of modernization and proponents of the ‘return to the asylum’ both invoke the value system of community. Conflicting identities too may be subsumed under this symbol. This is why it is possible to be, at the same time, a community health professional and not be a member of the community, or a community mental health nurse who works predominantly within a hospital setting.
This analysis has important clinical implications because the way in which community is invoked has consequences for those who work in the field of mental health. It determines the day-to-day nature of their clinical activities, the positions to which they are deployed, and the emergent structure of service innovations that perpetually reconfigure the landscape of mental health services. A striking change within the service we observed was the gradual elimination of the ‘open ward’, leaving just two options, the closed ward or the community. Hand-in-hand with this came a change in treatment practices. Provisions for ‘trial leave’ were used less often, and there was a greater tendency for patients to be discharged directly from the intensive care unit to their home.
Given the salience of the hospital–community boundary and its role in defining contemporary community mental health care, it is not surprising that much attention now focuses on shoring up this boundary. For example, ‘gate-keeping’ – ensuring that all but the most acutely ill people are kept out of hospital – has become an increasingly important aspect of mental health work. This is most conspicuously so for the staff who are strategically located at the various hospital entry points. It becomes their job to assess the community clients not only in terms of their illness and the risk it poses to them and those around them, but also in terms of how clients might be using their illness to gain admission to hospital. While symptoms and signs are still seen as surface manifestations of a client's underlying psychiatric disorder, they are to a greater extent seen as bargaining chips that this client may deal out in a game of getting hospital treatment. That is to say, we observe an increasingly strategic model of community clients, their illnesses and their personality structures.
Indeed, the most subtle but far-reaching consequence of the way community is invoked in mental health is that it posits a distinctive typology of persons. All the positive values that attach to community coalesce to form an ideal person-type that might be called the ‘client-in-the-community’. We have demonstrated that this idealized person exercises freedom, independence, individual responsibility and autonomy. He or she is self-directed, and can exert control over life decisions. Such a person is integrated into a domestic setting, surrounded by a social network and engaged in enduring reciprocal relationships that involve intimacy and monetary exchange. We have presented ethnographic data suggesting that people with mental illness are strongly encouraged to be this sort of person, not only with respect to how they manage their illness, but how they manage their lifestyle, indeed their life. As it is the symbol, community, which creates this ideal type of person, could the ‘client-in-the-community’ also contain contradictions – the injunction to be autonomous, the injunction to be integrated into a social network?
It is no accident that this ideal person-type partakes of and reinforces a definition of personhood that has become dominant in Australian society and in Western culture more broadly. But as community mental health workers themselves make clear, many people are unable to live up to these expectations. In our enthusiasm for community mental health care, are we unwittingly imposing a formulaic set of values that does not fit all? Given the stakes are so high, more attention needs to be paid to the question of what community actually means, especially in view of the scant empirical evidence for the efficacy of community mental health [5]. This anthropological analysis has been offered in the spirit of seeking to clarify and define community in its several guises: conceptual, symbolic and practical, in order that its appropriate place in mental health practice can be determined with more precision.
There are limits to the analysis we have provided here. In terms of the implications for mental health service organization and policy, further research is required to explore the extent to which there has been a change of professional dominance from the psychiatric profession (within the mental hospital) to nursing dominance (in the community) [11]. The strength of the community movement may derive, at least partly, from the way it has been embraced by an emergent nursing profession moving out from under the penumbra of the medical profession and into the more dominant role of health service management. Also missing from this paper is an analysis of the extent to which community mental health partakes of a broader ‘community’ movement in health care delivery, as evidenced by the move toward day-surgery, decreased length of stay in general hospitals and the development of medical hospital at-home programs. Larger cultural questions are raised by our analysis. What role does community play as a summarizing symbol in Australian society more broadly? To what extent does it underwrite a range of political, moral and economic agendas?
Finally, although we have referred several times in these two papers to Geoff Freeman, the CAS Team Leader, we have not focused sufficient analytical attention on the important role individual personalities can have in shaping ideas and structures of a community service, which in this instance could serve as a case example of the capacity for innovation and reform, and making a community service work in difficult circumstances.
Footnotes
Acknowledgements
Thanks to members of CAS for their commitment to this project. David Scott made a key contribution concerning syllogisms between narrative and counternarrative. We thank members of the Departments of Anthropology and Psychiatry at the University of Adelaide who critiqued this work. Mitra Guha and Bronwyn Norton undertook a careful reading for language and grammar.