
Abstract
High levels of mental disorder have consistently been identified among prisoner populations [1–4]. A recent meta-analysis of over 60 studies found that prison inmates were more likely than the general population to have a psychotic illness, major depression, or a personality disorder [5].
Explanations for the mentally ill being in prison include a lack of adequate diversionary options in the community, the reluctance of general psychiatric services to accept mentally ill patients from the courts, society's intolerance of deviant behaviour by the mentally ill, the high threshold for admission to general psychiatric facilities, co-morbid substance use problems and a low tolerance by the courts for this class of offenders [6].
No studies have compared the prevalence of a range of mental disorders in prisoners with community controls. Following the completion of the Australian National Survey of Mental Health and Wellbeing, itwas decided to use the National Survey interview with a large prisoner sample. Prisoners, and other institutionalized populations, are routinely excluded from community surveys.
We compare the 12-month prevalence of 18 mental disorders among prisoners and community respondents interviewed with the same screening instrument [7, 8].
Method
Screening for anxiety, affective and substance use disorders was undertaken using the Composite International Diagnostic Interview-Auto [9]. The interview yields 12-month and 1-month diagnoses for International Classification of Diseases-Version 10. Personality disorders were assessed with the International Personality Disorders Examination Questionnaire [10]. Symptoms of psychosis in the past 12 months were assessed using a screener incorporated into the program [11].
The 12-item Short-Form Health Survey (SF-12) was used to examine general physical and mental well-being and role limitations due to physical and mental health in the 4 weeks prior to assessment [12]. Two summary scales, the physical health summary scale (PCS-12) and the mental health summary scale (MCS-12) are derived from the SF-12; low scores indicate poor functioning. The Kessler Psychological Distress Scale (K10) consists of 10 questions on non-specific psychological distress and anxiety and depressive symptoms in the 4 weeks prior to assessment. The Brief Disability Questionnaire (BDQ) was also administered.
The prison study has been described elsewhere [8, 13]. One part, the reception sample, consisted of a consecutive sample of prisoners admitted into the state's correctional system over a 4-month period and assessed within 24 hours of admission (n=916). Men were assessed primarily at the state's main remand facility in the Sydney metropolitan area which processes around 80% of new admissions to the correctional system. Three small rural sites were also used. Women were assessed at the state's main reception centre for women in Sydney. The age range of the prisoner sample was 18–65 years for men and 18–56 years for women.
Data for the community were obtained from the 1997 Australian National Survey of Mental Health and Wellbeing, a nationwide household survey of adults. The overall methodology has been reported in detail elsewhere [14]. Data were collected for 10 641 persons of ages 18 years and above. Of those approached through a stratified multistage sampling process; 78.1% agreed to participate. The age range of the community sample was set to be the same as the prisoners for all analysis (n=8 168).
Demographic characteristics of the prison and community samples were compared using
Results
Consistentwith the known characteristics of prisoner populations, the inmate group tended to be younger than the community group, more likely to be men, less likely to be married, and have lower educational attainment (Table 1).
Demographic characteristics of prisoners (n = 916) and the community (n = 8168) (unweighted)
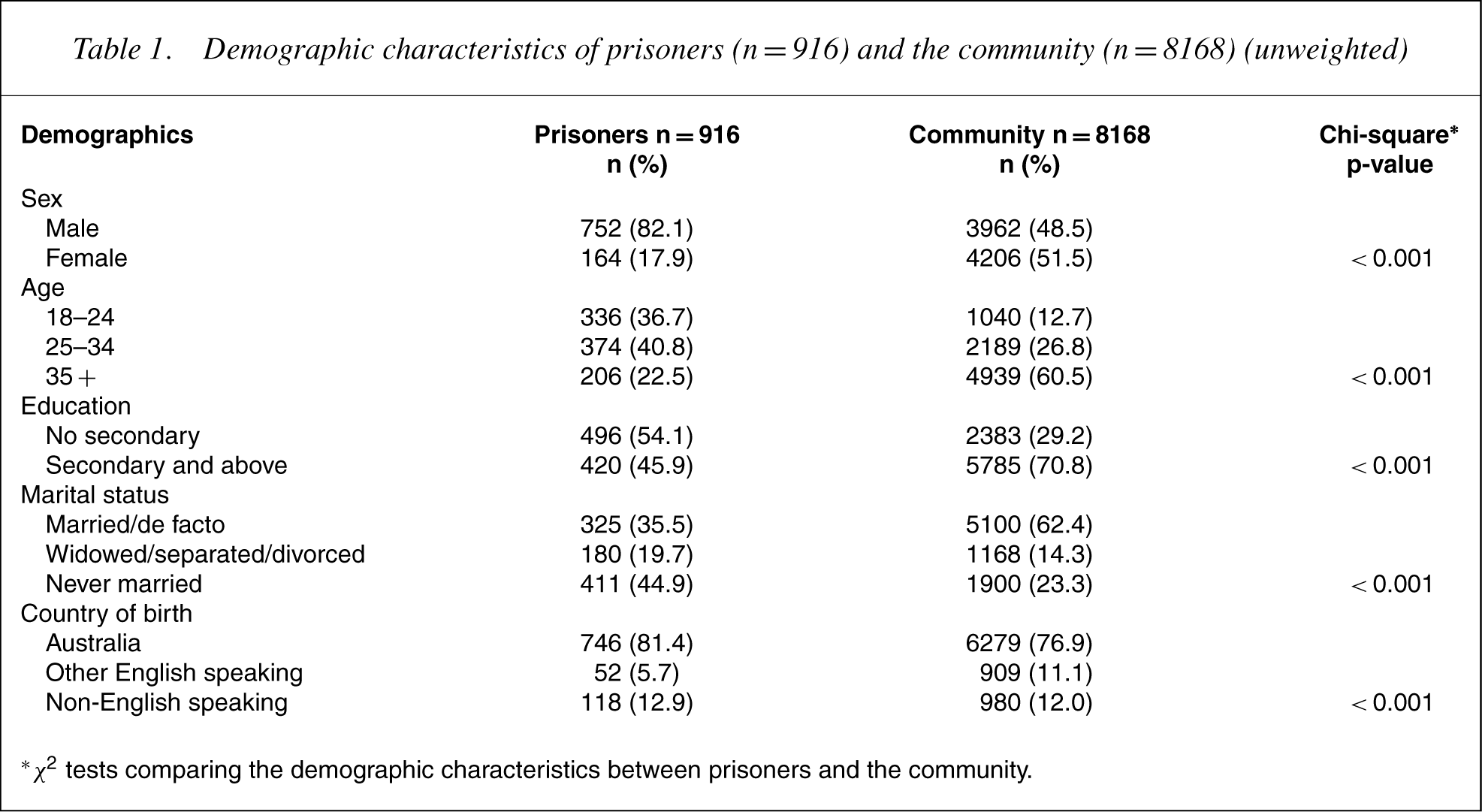
∗ χ2 tests comparing the demographic characteristics between prisoners and the community.
Across all major diagnostic categories, the prevalence of mental disorders in the prisoners exceeded both the crude andweighted prevalence in the community (Table 2). The overall prevalence of any psychiatric illness was 80% for prisoners and 31% (weighted) for the community. The contrast between prison and the community was most pronounced for substance use disorder (66% vs. 18%). Posttraumatic stress disorder (PTSD) was diagnosed in 26% of prisoners. Social phobia was the only diagnosis to be more prevalent in the community.
Crude and weighted† 12-month prevalence (%) of psychiatric disorders in the prisoner and community samples and adjusted‡ odds of prisoners (n = 916) having a psychiatric disorder compared with the community (n = 8168)
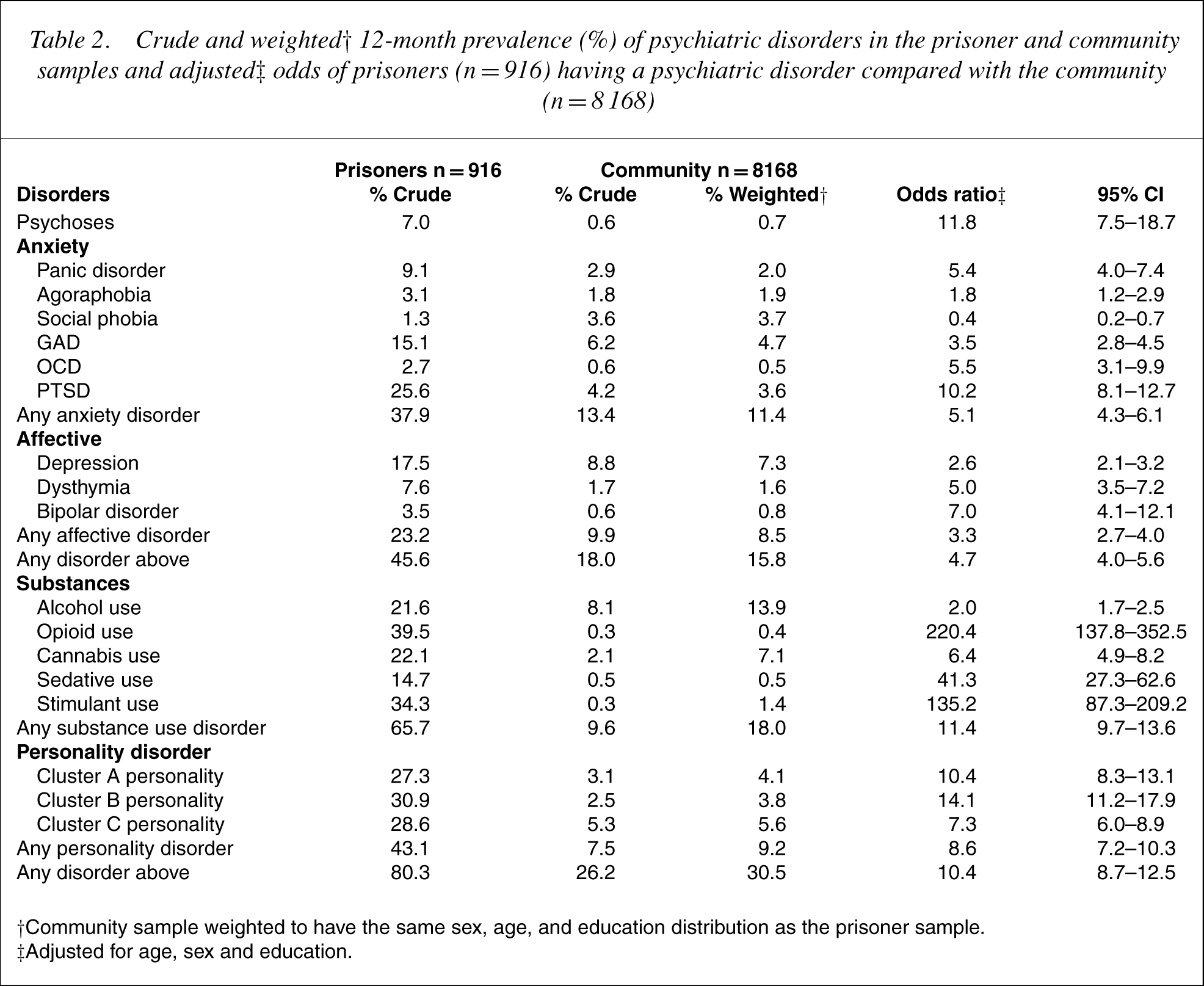
†Community sample weighted to have the same sex, age, and education distribution as the prisoner sample.
‡Adjusted for age, sex and education.
Substantial psychiatric morbiditywas detected among prisoners compared with the community after adjusting for age, sex and education. There was a strong positive association between being a prisoner and reporting symptoms of psychosis or PTSD in the previous 12 months. There was an overwhelming association between opioid or amphetamine use disorder and being a prisoner.
Prisoners had similar levels of physical functioning to the community group according to the SF-12, but a significantly lower score on the mental health component, further confirming the poor mental health of prisoners (Table 3). Increased psychological distress, as detected by the K10, was found in the prisoner group. The prisoner group also had significantly higher scores on the BDQ and reported a greater number of disability days in the month prior to admission than the community sample.
Adjusted† means for SF-12, K10 and BDQ in prisoners (n = 916) and the community (n = 8168)
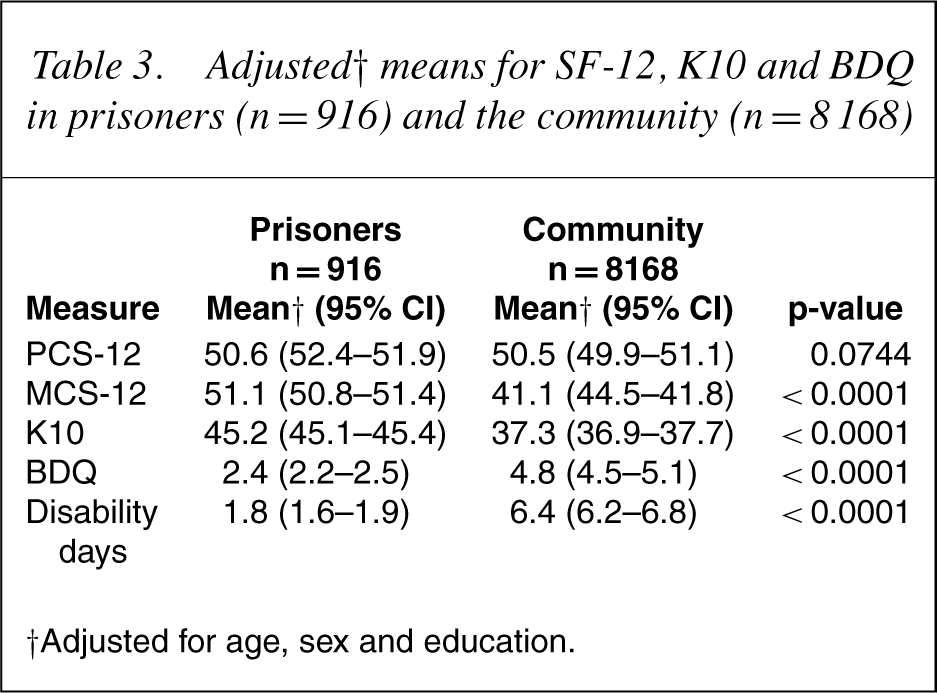
†Adjusted for age, sex and education.
Discussion
This study directly compares the results of national psychiatricmorbidity survey with a prisoner sample using the same diagnostic interview and, for the first time, controls for demographic variations in the samples. Our findings present a bleak picture of the mental health of Australian prisoners and supports the findings of other prisoner mental health studies [1–3,5].
Abuse of substances, particularly opioids and amphetamine, were much more common among prisoners than in the community sample and highlights that drug use is a crime and, on its own, or coupled with related property crime or violence, often leads to incarceration. Symptoms of psychosis and personality disorder were both more common in the prisoner sample in line with previous reports [1, 15]. Both personality disorder and symptoms of psychosis are associated with violent crime and again the preponderance is not surprising.
One-quarter of all prisoners met the criteria for PTSD. The wider community perceives prisoners as traumatizers. However, due to the social environment that they inhabit, prisoners are also a highly traumatized group. Social phobia was the only condition that was uncommon in prisoners, presumably because they are too shy and withdrawn to pursue criminal careers.
Leaving aside the illicit drug users and those people with psychosis or a personality disorder who have been violent, our findings suggest that many offenders who have a mental disorder are channelled into the correctional system. Priorities are in diverting some people who have committed minor offences away from the criminal justice system and providing community support for ‘high risk’ and forensic psychiatric patients after they are discharged into the community [16].
The prisoner group we used to compare with the community was a reception sample screened soon after entry into the correctional system and therefore should reflect their mental health status while in the community. Previous work found that the prevalence of mental disorder among a separate group of sentenced prisoners screened at the same time (median time in prison at interview 1.01 years) was lower than in the reception group [8]. While the explanations for this are likely to be complex and differ between diagnoses, it confirms that many prisoners received into the correctional system are highly distressed. It may also support the view that incarceration is an opportunity for those with mental health problems to be screened and receive treatment.
Limitations of this study include the use of self-report. However, previous research among prisoners has tended to dispel the myth of prisoners as unreliable survey respondents [17]. The results are also consistent with findings from numerous other studies highlighting mental illness and substance use disorders among prisoners [18–20]. Prisoners scored similar to the community with regard to physical health, suggesting therewas no attempt by them to exaggerate poor health. Data for the community was only available nationally not by state so comparisons were made between the Australian community and prisoners in NSW. The national community sample had an under-representation of young men with no secondary school qualifications and prevented a direct comparison with the community sample. This factor reinforces the notion that very disadvantaged groups tend to be underrepresented in community surveys and demonstrates the need for separate studies to examine these groups in settings such as prisons.
The psychosis screener we used is sensitive to the presence of psychotic symptoms due to any cause, but does not differentiate between the different types of psychotic disorders (drug-induced psychosis, brief episodic psychosis, and functional psychotic illness). Thus it was not possible to determine the prevalence of functional psychotic mental illness (schizophrenia, schizophreniform psychosis, schizoaffective disorder, delusional and affective psychosis), using the psychosis screener alone. Further work is required to determine the actual presence of psychotic mental disorder in the prisoner population.
The mentally ill too often revolve through prisons, with periods of incarceration interspersed with spells in the community [21]. Prison does represent an opportunity for intervention and treatment and, in some cases, may be the only time certain individuals are in contact with treatment services [22]. Notwithstanding this, it is unlikely that prison is the best therapeutic environment for those suffering from a mental illness.
Footnotes
Acknowledgements
The Forensic Mental Health Section of Justice Health NSW funded this project. This project would have been impossible to complete without the dedication and commitment of the nurse interviewers – David Cain, Dale Owens, Chris Muller, Lee Trevathan, Michael Harris, Alison Lee, Peter Sadler, Rebecca Gibson, and Eli Baxter. We wish to thank the NSW Department of Corrective Services for providing custodial staff to assist with retrieving inmates, particularly Mr Brian Kelly from the MRRC, and Ms Lee Downes from Mulawa. We also wish to thank all the participants for their valuable contribution to this project.