
Abstract
This paper is an ethnographic analysis of an emergency community mental health service that we have called the Crisis and Assessment Service (CAS). Community mental health is the dominant form of contemporary mental health care delivery [1]. Given the singular importance of ‘community’ in this form of care, one would expect considerable analytical attention to be paid to what is meant by community. Yet within the mental health literature, it is usually presented as a demographic or geographical given – a starting point for the study of service delivery [2]. This is the first of two papers that employ an anthropological perspective to study community as an object of enquiry in its own right. Anthropologically, it is the symbolism of community that is paramount (we adopt the convention of italicizing the word community when we refer to it as a cluster of symbolic meanings).
Symbols are concepts, places, activities or objects that stand for shared meanings. An influential development in the anthropological study of symbolism is Ortner's work on summarizing symbols [3]. They transcend context, are universally recognized and may carry a potent emotional cathexis (the Stars and Stripes is her example). Summarizing symbols stand for an agglomeration of social values (in the case of the Stars and Stripes, democracy, competition, progress, free enterprise), summing them up and expressing them in a tangible way.
Anthropological studies of communities have also demonstrated that it is along the boundaries of a community, where its identity is potentially most vulnerable, that symbolism becomes most concentrated [4–7]. While symbolic meanings appear to have a life of their own, they are never independent of intense human activity – interpreting them, challenging them, reshaping them. Abbott has used the term ‘boundary work’ to describe this type of human activity [8]. It is at these boundaries that the very definition of a community as an entity is forged. Boundaries, then, delimit the edge of a community and define its essence.
As we will show, community operates as a summarizing symbol and it is through boundary work that it is appropriated and put to use by members of a community mental health service.
Ethnographic methodology
Approval to conduct this research was granted by the hospital research ethics committee and attention was given to securing informed consent from individual participants and from the CAS service as a team [9]. Data were collected over a 12-month period using ethnographic fieldwork [10]. DP was responsible for most data collection. Participant observation was used to gather data on CAS worker–client interactions, clinical and administrative meetings and interactions between CAS workers and members of other agencies. This entailed entering into the daily work routines of the CAS service, making repeated observations to the point of data saturation. The initial period of immersion into CAS proceeded smoothly as a consequence of DP's experience as an ethnographer in a medical setting. Within 3 months, he was no longer seen as an outsider. Participant observation was supplemented by interviews with CAS workers, usually singly but also in groups of two or three. Always informal, these interviews would begin with direct questions on particular aspects of work at CAS, the focus of these questions shifting as the research unfolded. Care was taken to allow interviews to be participant-directed. Policy documents and mental health legislation were also used as data sources. Ethnographic data were primarily generated through interactions with mental health professionals, though we draw to a lesser extent on interactions with individuals designated as clients or patients (following ethnographic practice we use ‘native’ terms throughout: ‘client’ therefore denotes a person treated in the community, ‘patient’ denotes a person treated in hospital). Data were recorded in fieldwork notebooks closely following the event or activity under observation, then written up in more detail using a word-processor. We did not use audio or video recordings.
Both authors performed the ethnographic analysis. Recorded data were organized by means of an indexing system into recurring domains – those to which participants gave emphasis – be they activities (‘home visit’, ‘discharge’) or concepts (‘acuity’, ‘pressure on beds’). We searched these domains to identify specific day-to-day contexts in which the term community occurred, and to identify the values attached to it in that context (e.g. ‘freedom’ and ‘belonging’). Emphasis was placed on values that emerged across a range of contexts. With two analysts undertaking this study, we were able to triangulate the data and their interpretation by comparing values that we had separately identified. Similarities bolstered the analysis. Differences were discussed and the process of their resolution deepened the analysis. Thereby, we developed a composite account of community, the range of instances in which this symbol was employed, the values it stood for and the relationship of these values with each other (e.g. oppositional relationships such as ‘responsibility versus dependence’ were prominent). Cross-validation was accomplished within the study by comparing units of ethnographic data from these diverse contexts. Data collection continued during the analysis phase. Hence we were able to confirm or modify our interpretations in dialogue with research participants themselves. This is in keeping with Strauss' exegesis of grounded theory [11]. Earlier versions of this paper were presented to CAS workers as a group once analysis had begun. Their responses contributed to our final analysis. The data were further cross-validated in relation to comparable ethnographies of community mental health, including Estroff's Making It Crazy [12], Rhodes's Emptying Beds [13] and Lucas's Uncommon Lives [14]. All names and identifying information, including details of sketches to follow were changed to preserve anonymity.
The Crisis and Assessment Service (CAS)
The Crisis and Assessment Service had a brief to provide a 24-hour assessment, crisis intervention and shortterm community care service for a quarter of a million people living in one sector of an Australian city. It was one component of a Community Mental Health Service associated with the Royal Prince Andrew Hospital (RPA), an imposing, multistorey, public teaching hospital in the city (Fig. 1). The service included a psychiatric intensive care ward. The two ‘open’ wards were ‘M8 South’, in the south wing of the RPA, and Hannaford, located at Tennyson Park, a mental hospital with extensive grounds and heritage-listed buildings redolent of its 19th century origins as Tennyson Lunatic Asylum (Fig. 2). Other components included two Continuing Care Services, an Intensive Community Care Service and a range of facilities for rehabilitation and community accommodation.
The hospital – Royal Prince Andrew. Asylum – Tennyson Park.
Thirty people worked at CAS. There were 17 nurses, six social workers, three medical staff (two part-time consultant psychiatrists and one trainee psychiatrist), a psychologist, two administrative assistants and a Team Leader, Geoff Freeman, whose background was in mental health nursing. Compared with other areas of the service, positions at CAS carried a special prestige. Workers there were more senior and experienced, many hand-picked for the job, giving CAS a distinctive esprit de corps.
The headquarters was a low-profile suburban building, its front section formerly a private residence (Fig. 3). Referrals came by telephone from clients, family members, friends, general practitioners and police. The Crisis and Assessment Service received about 70 calls each day. Workers would drive out to provide face-to-face clinical intervention for clients, be it in their home, hostel or on the street. The average length of involvement with clients was less than a week. At any one time, CAS had 40 or more clients in active care. It was a busy service.
In the community – CAS headquarters.
The boundary between community and hospital
When describing the work of CAS, workers laid great store on its community focus. In keeping with the eth-nographer's practice of questioning the self-evident, DP began by asking what they meant by community. The early explanations coalesced into a coherent account of community that provided a rationale for daily practice. We recognized this to be an orthodox version of community, the official account for consumption by outsiders.
In this analysis we have identified this as a narrative of community. Our use of the term narrative moves beyond just a personal narrative, as used by Kleinman [15], to incorporate a collective narrative. Though found in local settings, such as the workplace, such narratives have a broader historical and cultural resonance as ‘the stories we (individually and collectively) tell ourselves, stories which provide the frameworks through which we act’ [16].
As DP became immersed in the field, he noted other ideas of community that subverted this orthodoxy, and did not seem to be compatible with the narrative. Further analysis demonstrated that these ideas together formed a counter-narrative. This paper identifies differences and underlying similarities between narrative and counternarrative of community.
The space of community and its signifiers
It is notable that CAS workers did not define the community in its own right. They always defined it in opposition to the hospital. For example: Community's whatever's not inpatients. When you think about it, it is an opposition.
When CAS workers elaborated on this opposition, they chiefly did so in spatial terms – the community lay outside the hospital. When it was first set up, CAS headquarters was located on the grounds of Tennyson Park, where workers felt enveloped by the identity of the institution. It was only when the headquarters moved out into the suburbs that the service realized its true community identity.
The ‘hospital’/‘outside-hospital’ opposition was principally described by CAS workers in terms of a closed/ open dichotomy. The hospital contained the ‘closed’ or ‘locked’ ward. The community was a wide-open space. There were intermediate zones such as the two ‘open’ wards, M8 South and Hannaford, where patients were freer to come and go. As the community arm of the service grew, siphoning financial resources from the inpatient sector, M8 South and Hannaford wards shrank from a total of 43 beds down to 32, leaving room to admit only the most ill or ‘high acuity’ patients. Eventually, the entrance to M8 South was locked and it became a de facto closed ward. Hannaford too began to lock its doors in the mornings. Thus, the community service absorbed what openness there was about the wards, sharpening the distinction between community as open and hospital as closed.
When CAS workers talked about the open space of the community, they invoked the social value of freedom: first and foremost, freedom of movement. Clients in the community were at liberty to move from one suburb to another, or even interstate. Confining people was avoided unless there were compelling reasons.
If it's their first episode then maybe being in hospital for a while might be a good thing. But if you take an older schizophrenic, they've been around a while, doing their own thing. They're alive. Why put them in hospital?
The concomitant of freedom was responsibility. The Crisis and Assessment Service workers maintained that to be a client in the community was to be a person who took responsibility for living arrangements, for managing their finances and for the consequences of their actions. During telephone contact, workers would encourage clients to ‘prioritize’ things, take ‘some control’ over their life and become more ‘self-directed’, not only to enhance their mental health, but also as a general strategy for living. The following exchange between three CAS workers about a ‘non-compliant’ client was typical: Amelia: We told her she'd have to be more self-directed, take some responsibility, as part of our overall treatment plan. Michael: Yesterday she drank half a bottle of Scotch. Simone: Yes, no one's likely to get anywhere until she stops drinking. But it's up to her.
Maintaining behaviours that adversely affected mental health – substance use, staying in damaging relationships, breaching residential tenancy conditions – was evidence that the client was failing to take responsibility for himself or herself. Sometimes this norm of ‘respon-sibility-in-the-community’ was so flagrantly breeched that CAS workers, feeling powerless to do anything, responded with exasperated humour. In a clinical discussion, one worker enacted a client's plea, mimicking his imploring tone: I've been taking methamphetamines. I haven't been taking my medication. Can you help me?
The Crisis and Assessment Service workers also depicted the community as a place of integration, in contradistinction to the hospital as a place of segregation. In the community, clients were integrated into their domestic niche, surrounded by family and friends; in the hospital they were segregated from those who were close to them.
The CAS service was proclaimed to be an integrated part of the integrated community [17–19]. An ethos of integration informed interdisciplinary relationships. The Crisis and Assessment Service workers went on home visits in pairs, comprising any combination of disciplines (a nurse and a social worker, or an occupational therapist and a psychiatrist). At the twice-daily clinical discussions, workers were seated in a circle and all would spontaneously contribute. There was a relative lack of professional demarcation. Within each professional discipline, super-ordinate–subordinate distinctions were attenuated, giving CAS a hierarchical structure that was relatively flat. After absorbing this ethos of integration for some time, CAS workers developed what they called a ‘community mindset’, an approach to mental health care that you just could not practise within the walls of the hospital.
The opposite of integration was segregation, and it was unsurprising that CAS workers found this quality in their ward counterparts who, they said, were cut off from the ‘real world’ of the community. Professional role demarcations were more sharply drawn in the ward. The staff hierarchy was more evident.
The dichotomies we have described – open versus closed, free versus confined, responsible versus dependent and integrated versus segregated – formed the principal opposing values through which the workers defined the community in relation to the hospital. They are represented schematically in the upper section of Fig. 4. Note that ‘autonomous’ versus ‘regulated’ formed another polarity. The Crisis and Assessment Service workers believed that they exercised more professional autonomy working in a community setting than in a ward and, at the same time, expected their clients to be autonomous.
Community as a summarizing symbol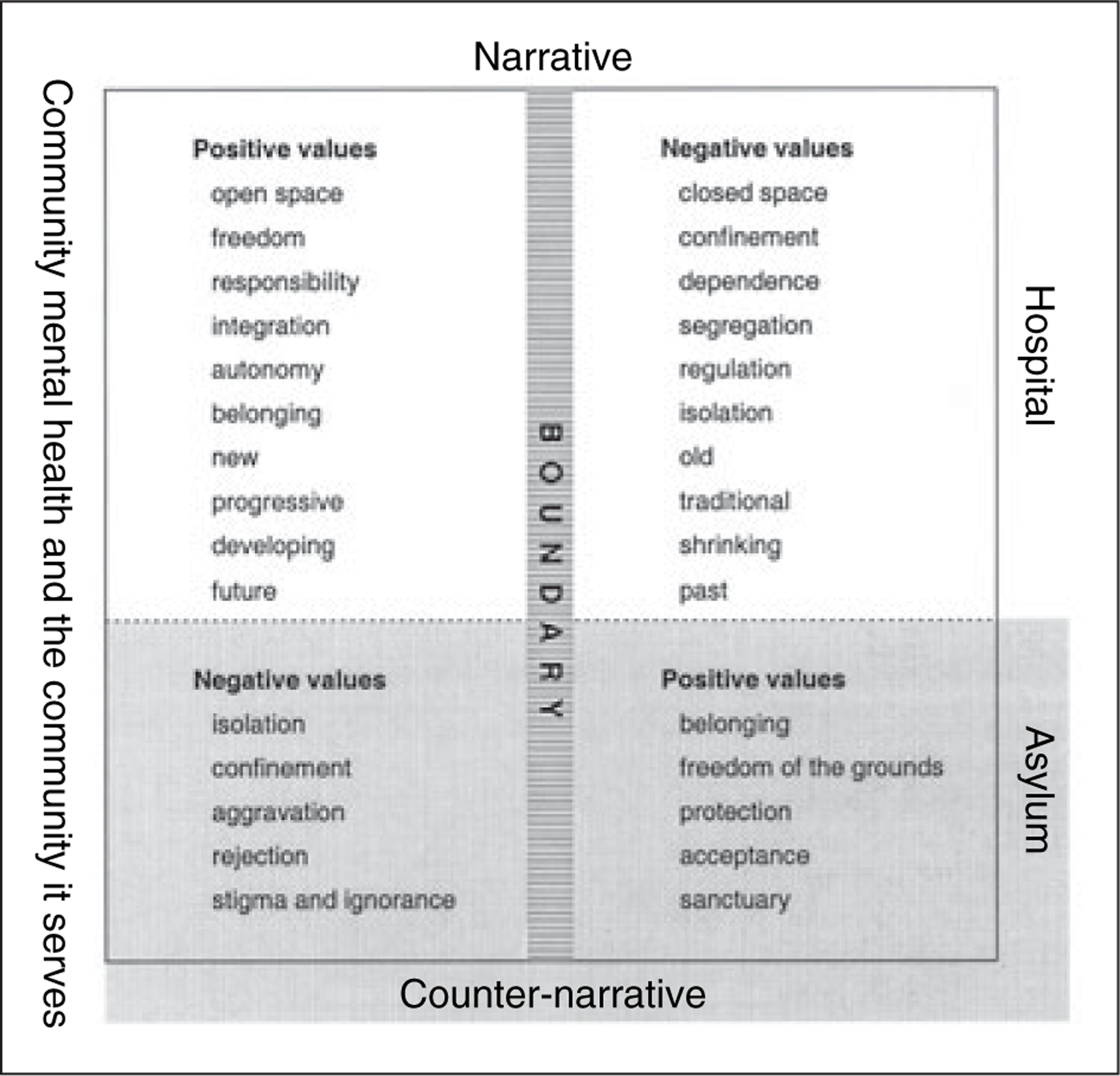
Within the orthodox narrative, community was a summarizing symbol because it stood for an agglomeration of values – openness, freedom, responsibility, integration and autonomy – that all CAS workers subscribed to. It was a potent symbol because the values it stood for were recognized and endorsed throughout the wider society. Within the service, community transcended contexts – it applied to the noun, community (the place in which clients lived) and the adjective community (describing a form of mental health service). And it had a compelling immediacy; it was like a banner.
So compelling was this summarizing symbol and its associated value system that it constituted two types of people under treatment. When a person was treated in the community, he or she became a client, and was perceived as internally integrated – a whole person. ‘We have a holistic approach; we treat the whole person.’ When in hospital, the same person would become a patient, here fragmented into an assemblage of parts (‘investigation results’, ‘mini-mental’, ‘behaviour on the ward’).
The time of community and its signifiers
The hospital and the community were distinguished from each other in time as well as spatially. The Crisis and Assessment Service workers portrayed the hospital as traditional, a thing of the past. The community was progressive, the shape of things to come. This contrast has surfaced repeatedly over the past four decades within the literature [20–22]. Both appropriate an ideology of progress, so central to modern society, and they give it a particular inflection, wherein hospital is to community as old is to new. At CAS, the most obvious expression of this was to be found in policy statements replete with phrases such as ‘service development’, ‘a new millennium’, ‘moving on’, ‘development of partnerships’, ‘emerging’, ‘directions’ and ‘expansion’. The Crisis and Assessment Service was the vanguard of the Community Mental Health Service – a conduit for change and innovation. In 3 years it grew by absorbing the Intensive Community Care Service and developing another two major service arms that we discuss below.
When locating community mental health within a narrative of progress, CAS workers limited themselves to the span of their professional memories and those of senior colleagues with whom they had once worked. One recalled: ‘When I started in the 1970s we were basically working with a 1930s 1940s model of the asylum.’ None spoke of community initiatives prior to the 1960s. Such histories are sometimes reproduced in the psychiatric literature, a recent example being the evangelical account by Feldman [23], who conveys the impression that community mental health is just 40 years old and that it started with John F. Kennedy's famous speech in 1963. Rossi has commented on this tendency to provide foreshortened histories, which assert ‘that community mental health philosophy and activities began almost de nouveau after World War II’ [17].
Yet community movements have a longer provenance. Psychiatry developed a community focus during both World Wars [18, 19]. Earlier still the mental hygiene movement developed a form of care orientated to ‘the natural units of community life’ [24]. In the mid-19th century, England inmates of the Devon lunatic asylum were placed in houses in surrounding villages [25]. More celebrated still was Gheel, in Belgium. In the early 19th century, it was at the centre of debate concerning the relative merits of community versus hospital care [26].
It is possible that the birth of community as a summarizing symbol, at least as it applies to mental health, coincides with the era in which asylums were established. Since then each generation has reinvented a community movement, harnessing the caché of community to its own project. The amnesia of each generation enables it to present its own version of community mental health as novel and progressive.
Boundary work as counter-narrative
The Crisis and Assessment Service workers also articulated a counter-narrative (the lower, shaded portion of Fig. 4) that appeared to contradict the orthodox view and cast doubt on the community approach. It emerged during casual conversations about CAS or discussions about clients who were ‘not coping’ in the community. You might hear expressions of the counter-narrative in the car on the way back from a home visit.
Within this counter-narrative, the archetypal client was the person who lived alone, isolated by their illness, not interacting with others, and with no real quality of life.
There might be a community of clients, a community of staff, and a community of suburbs, or whatever, but many of our clients don't interact with the community.
For these clients, the community mental health worker formed their only point of contact. That they were ‘free to choose’ to have friends, or that they had a ‘potential to be integrated’ with the community was considered by most workers to be ironic.
In the counter-narrative, the community was a space of confinement not freedom. First, clients could be legally confined by Community Treatment Orders. Second, CAS workers talked of clients who were locked within a delusional world, imprisoned by their illness. Third, hostels and supported accommodation facilities were seen as confining. Sometimes crowded four to a room, locked out of their bedrooms during the day with nothing to do but wander the streets, they were inmates of what were called ‘mini institutions in the community’.
Community members were not always perceived as helpful. Families might be so dysfunctional that they aggravated the client's illness. Friends could have a negative influence. Most CAS clients had comorbid polysubstance abuse. Clinicians agreed that illicit drugs counteracted antipsychotic medication. Drugs were usually bought from and taken with friends or acquaintances. Sometimes friends could act strategically against the community mental health team. One client, under a Community Treatment Order, lived at the end of a cul-de-sac. When CAS workers would arrive, other residents would alert the client, who would escape over his backyard fence. The neighbourhood, a core element of a client's community, was sometimes regarded as hostile. For example, representatives of one neighbourhood applied pressure to close a residential facility and this had to be resisted by senior members of CAS.
Within the counter-narrative, CAS workers could be as damning of the community service as they were of the community. Community services, they said, were not integrated – clients regularly ‘fell between the cracks’ and ‘continuity of care’ was a thing of the past. The RPA Community Mental Health Services worked to overcome service fragmentation by organizing staff development days and devising electronic clinical information systems. Their goal was a ‘seamless service’. But fragmentation was a necessary condition of community work, not merely an organizational shortcoming. Clients were defined as responsible individuals exercising freedom. It was impossible to provide a comprehensive, integrated service without restricting this freedom. The more CAS adhered to its ideology of individualism, the harder it was to achieve its ideal of integration.
Like the orthodox narrative, the counter-narrative pitted the community against the institution, but with two differences. First, it valued the community negatively. Second, it talked not of hospitals but of the old asylum. The positive values that, in the orthodox narrative, were attached to the community were transferred, in the counter-narrative, to the asylum. With its heritage-listed buildings, Tennyson Park served as a suitable halcyon image. The Crisis and Assessment Service workers were aware that Tennyson Park's days were numbered but did not concentrate on this. And they were aware of its grim, oppressive history, but did not mention this. Instead they talked of park-like grounds that allowed a measure of freedom, and how patients there enjoyed a sense of belonging because they were so well known to the staff and to each other.
In spite of differences between narrative and counternarrative, they were nonetheless homologous. The narrative posited a community of free, responsible, autonomous individuals, cozily integrated with one another, exaggerated to the same extent that the negative qualities of the hospital were exaggerated. The counter-narrative likewise posited an asylum of security and sanctuary, exaggerated to the same extent that the negative qualities of the community were exaggerated. Both invoked the symbol community and its system of values. In the narrative, these values were applied to the community and the community mental health service; in the counternarrative, nostalgic asylum imagery was evoked and imbued with community. Paradoxically, in the counternarrative, the community and the community mental health service were invested with values that were the antithesis of community. Finally, neither of these narratives positively valued the hospital: one invested the hospital with negative values, again the antithesis of community, whereas the hospital did not figure at all in the other narrative.
Practicing boundary work
Boundary work went beyond reflection and conceptualization; it was a form of practice. Clinically, organizing admissions and discharges across the hospital–commu-nity boundary was a major focus of CAS work, most of it over the telephone: ringing around for beds, going through inpatient lists, identifying who could be safely discharged in order to free up beds for new admissions.
Particular attention was paid to staff positions on the hospital–community boundary. Geoff Freeman filled these positions with mental health nurses who had worked long enough in the community to have a strong ‘community mindset’. The RPA Emergency Department was one such boundary site because it was a major entry point to the hospital. Four CAS mental health nurses were positioned there to give 24-hour coverage in a ‘gate-keeping’ role. It was recognized that they could easily undergo a shift in mindset and revert to thinking like hospital nurses. They might begin to err on the side of admitting patients rather than arranging community follow-up. Geoff therefore required that they maintain telephone contact, appraising CAS of decisions and liaising closely with community resources. The Crisis and Assessment Service thereby exerted control over decision-making at an important threshold on the boundary.
The Crisis and Assessment Service made further inroads into the RPA. With ongoing bed closures, the demand for psychiatric beds soon exceeded capacity, leading to patients being admitted as ‘outliers’ in medical and surgical wards, where there was a lack of specialized psychiatric expertise. When a mental health team was established to manage these patients, the pivotal role, that of the clinical nurse, was established under the aegis of CAS. Community mental health thereby encroached into the heart of the traditional teaching hospital.
The Crisis and Assessment Service also brought components of the hospital out to the community by establishing a ‘Hospital at Home’ service for clients who would otherwise be admitted to hospital, providing even higher levels of nursing care for these clients in their own homes. The Crisis and Assessment Service was appropriating a core hospital function – the management of the acutely unwell patient – and transferring it into the community domain.
The principal service developments occurring during this study were transformations across the hospital–com-munity boundary, whereby community services made inroads into the hospital, and hospital services were pulled out into the community. In mental health, the hospital only accrued positive value insofar as it was imbued with community.
Conclusion
This paper has focused on the boundary work whereby community is defined in juxtaposition and opposition to institutions (the hospital or the asylum). We have demonstrated that community draws together the positive values of openness, freedom, responsibility, integration and autonomy. Community mental health and the community it serves are imbued with these values, while the hospital is imbued with opposing, negative values, as if it were not part of the community. Through counter-narrative, nostalgic evocations of asylum are invested with the value system of community, while the community becomes its antithesis – the good is incorporated into the disappearing asylum, the bad externalized back out into the suburb. Ostensibly subversive, this counter-narrative does not undermine community as a summarizing symbol, for it works along the same boundary and articulates the same values and oppositions.
This analysis is extended in a companion paper that examines the impact of community symbolism at a professional versus personal level, and explores the consequences of this symbolism for mental health care.
Footnotes
Acknowledgements
Thanks to members of CAS, in particular David Scott who made a key contribution. Thanks to members of the Departments of Anthropology and Psychiatry at the University of Adelaide who critiqued this work. Mitra Guha and Bronwyn Norton undertook a careful reading for language and grammar.