
Abstract
Keywords
We previously reported the clinical effectiveness of community treatment orders (CTOs) in terms of reduced relapses and readmission rates, decreased length of stay, and increased contact with Community and Crisis Teams in two groups of patients with schizophrenia [1]. These groups consisted of patients on depot or oral antipsychotic medication. One factor contributing to poor outcome in community settings is lack of adherence to prescribed treatment. A response to non-adherence is the use of legislation-based involuntary outpatient commitment [IOC) [2–4]. In England and Wales an amendment to the Mental Health Act (1983) was made and in October 2008 an IOC in the form of supervised community treatment (SCT) was introduced into clinical practice [5]. Despite such increasing use of IOC, outcomes that may be associated with improved quality of life such as a reduction in problem behaviours and improved social functioning in patients subject to CTOs are rarely examined.
Behavioural change and quality of life
Increased suicide rates among patients with schizophrenia have been a consistent finding in the literature. A meta-analysis by Palmer et al. in 2005 estimated that 4.9% of people with schizophrenia commit suicide during their lifetime, usually near the illness onset [6]. Further, deliberate self-harm is a strong predictor of suicide among patients with schizophrenia [6].
Schizophrenia is now well established as a risk factor for violence. Walsh et al. concluded that 10% of societal violence may be attributable to schizophrenia [7]. The prevalence of community violence in discharged patients has been estimated to be 9% [8]. Swanson et al. found a reduced incidence of violent behaviour among patients subject to IOC [9].
Reduction in episodes of deliberate self-harm and suicide and of violent or aggressive behaviours among people with schizophrenia would be important indicators of improved outcomes of patients with schizophrenia subject to CTOs.
Social functioning and quality of life
Studies of rates of schizophrenia among homeless persons give ranges between 15% and 46% [10,11]. Schizophrenia was found to be a significant risk factor for homelessness by Folsom et al. [12]. Compton et al., in a sample of 204 patients with serious mental illness, found a significant short-term decrease in the risk of homelessness in patients subject to IOC versus those who were not [13]. Compared with homeless people with mental illness, those who have stable accommodation were not only more satisfied with their living arrangements, they were also more satisfied with family relations, finances and daily activities [14]. In a study by the same group, persons with severe mental illness who were treated assertively spent 31% more days in stable housing compared with those receiving care by usual services [15].
Based on these studies, the authors would hypothesize that a CTO may enable more assertive treatment for patients who would otherwise refuse treatment and this may positively impact on their accommodation status.
Family relationships may be regarded as an important outcome indicator in patients treated with IOC, because many patients reside with their families. It is plausible that, when CTOs are clinically effective, this may enable family relationships to be repaired. Mullen et al. in qualitative interviews with 27 families of patients with serious mental illness subject to compulsory treatment orders, found that families were generally in favour of compulsory community treatment due to perceived positive influence on their relative, on themselves, on family relationships, and on relations with the clinical team [16]. The authors were unable, however, to identify studies that examine family relationships among involuntary patients in the community.
High unemployment among persons with severe mental illness is well recognized. An unemployment rate of >75% in a sample of 16–64-year-old Australians with psychosis has been reported [17], suggesting that better occupational and vocational services may benefit this group. The value of employment in terms of improved self-esteem and quality of life among people with severe mental illness is increasingly recognized [18].
In this paper we aim to examine behavioural and social outcomes of a group of patients with schizophrenia subject to a CTO. This sample was described in a previous publication [1]. Information was gathered from case notes that might provide external indicators of the social functioning and problem behaviours of patients with schizophrenia before and after the instigation of a CTO. These indicators included recorded episodes of aggression and suicide attempts as well as documented periods of homelessness and employment and documented comments regarding frequency and quality of interaction between the patient and family members. We hypothesized that CTOs reduce problem behaviours such as self-harm and attempted suicide and violence, and that CTOs would improve social functioning through reduced periods of homelessness, higher employment and improved quality of family relationships.
Methods
This was a naturalistic retrospective mirror image study of case notes with each case serving as its own control. Behavioural and social outcomes of patients diagnosed with schizophrenia and treated under a CTO were examined. The study was conducted in three mental health services covering urban and suburban areas in metropolitan Melbourne. Eligible patients attended any of these services, were diagnosed with schizophrenia, and placed on a CTO during the study period. Cases were identified by a manual search of Mental Health Act reports of current and past patients placed on CTOs. The sample was divided into two subgroups consisting of patients treated with either oral or depot antipsychotic medication. A more detailed description of the method is provided by Muirhead et al. [1], including inclusion and exclusion criteria.
Data collection
Data were collected by retrospective medical record review for the period of 12 months before the implementation of a CTO (the pre-CTO year) and for the period of 12 months following the implementation of the CTO (the CTO year). A data collection instrument was developed specifically for this study. Variables were selected that would give the most reliable indicators of outcome considering the potential unreliability of medical records, and including those deemed to be important in outcome research in related studies. Variables included number of episodes of aggression and suicidal and self-harming behaviour, number of episodes of homelessness, frequency of contact with family members and the overall quality of relationship between family and patient, as judged using all available information, and finally, employment status. Data were extracted from the notes guided by the following parameters: (i) episodes of aggressive behaviour included physical force used against others or property, intimidating behaviour and verbal aggression sufficient to cause others to be fearful of their safety; (ii) suicidal or self-harming behaviour was recorded but not suicidal ideation due to perceived lack of reliability of recording of this latter information in the medical records; (iii) homeless episodes were recorded when there was a basic lack of shelter or patients were living in temporary or emergency accommodation; (iv) the overall quality of the relationship between the patient and their family was assessed, making use of documented observations such as whether the patient was participating in, or withdrawing from, family interaction and activities; (v) frequency of contact with family was estimated from reports in the clinical file; and (vi) best employment status whether unemployed, voluntary, part time or full time work was recorded.
Interrater reliability
Two researchers were involved in collecting the data for this study (GI, DM). Data collection from case note studies can be notoriously unreliable. In order to estimate the reliability of the data that were collected, the researchers both independently assessed a randomly chosen 10% of notes previously assessed by the other. These two sets of data were used to calculate interrater reliability scores (expressed as either Spearman's ρ or Kendall's τ).
Statistical analysis
All data were analysed using SPSS version 14.0 (SPSS, Chicago, IL, USA). For all results p<0.05 was considered statistically significant. Repeated-measures tests were used to compare data from the pre-CTO year with the data from the CTO year for the total group, the first experimental subgroup (oral medication) and the second experimental subgroup (depot or combination medication). The distribution of the bulk of the ordinal measures was highly skewed and the Wilcoxon signed rank test was therefore used to determine statistical significance. The feasibility of performing a repeated-measures ANOVA with time (pre-CTO vs CTO year) as a within-subject variable, and group (depot or not) as a between-subject factor, was explored. Because the data were highly skewed, an attempt was made to transform the relevant variables. Only one of these six variables (episodes of aggression in pre-CTO year) could be transformed by any method (log, square root and inverse of zero methods). Because we were unable to adequately fulfil the underlying assumptions, we did not proceed with this analysis. Significant changes in categorical repeated measures were investigated using the marginal homogeneity test because several cells had low numbers.
Results
Of the sampling frame of 212 patients placed on a CTO for at least 10 months, 94 were identified as meeting the inclusion criteria. The majority of patients were excluded because they did not have a diagnosis of schizophrenia [1].
An overview of the characteristics of the entire patient group and the two subgroups is documented in our previous publication [1]. In brief, the mean age of the total sample was 39 years (range = 18–66 years). Most were male, almost two-thirds had never married, and just over half lived with families. Mean length of illness for the total sample was 13 years (range = 1–39 years). Secondary diagnoses within the sample were relatively rare; for example, 16 (17.0%) had a secondary diagnosis of alcohol misuse and 29 (30.1%) had a diagnosis of substance misuse. Comparisons between the two subgroups (oral and depot) on demographic and clinical variables showed no statistically significant differences, except for a significantly higher antipsychotic dose prescribed to the oral subgroup in the CTO year (Mann Whitney Z=−2.608, p = 0.009) [1].
When comparing the ratings made by the two researchers to assess interrater reliability, the following correlation coefficients were obtained: for aggressive episodes in the pre-CTO year, σ = 0.71 and in the CTO year, σ=0.81; for suicide attempts in both the pre-CTO and CTO years, σ = 1; for episodes of homelessness in the pre-CTO year, = 0.8, and in the CTO year, σ=1. The interrater reliabilities for the remaining measures were: frequency of family contact in the pre-CTO year and the CTO year, τ = 0.96; quality of family contact in the pre-CTO year, τ = 0.05, and in the CTO year, τ = 0.32; and employment status in the pre-CTO year, τ = 1, and in the CTO year, τ = 0.66. Quality of family contact was excluded from further consideration due to poor interrater reliability.
There was a significant reduction in the number of episodes of aggression (by approx. half in each instance) when comparing the pre-CTO and CTO year in the total patient group (Z=−3.494, p = 0.0001), the oral group (Z=−2.157, p<0.05) and the depot group (Z=−2.707, p< 0.01; Table 1). The number of suicide attempts made during the year of CTO was not reduced in any of the three groups. There was a significant reduction in the number of episodes of homelessness in the total patient group (Z=−2.111, p<0.05), but significance was not achieved for the oral (Z=−1.732, p = 0.083) and depot subgroups (Z=−1.414, p = 0.157) alone.
Aggression, suicidal behaviour and homelessness before and during the CTO year
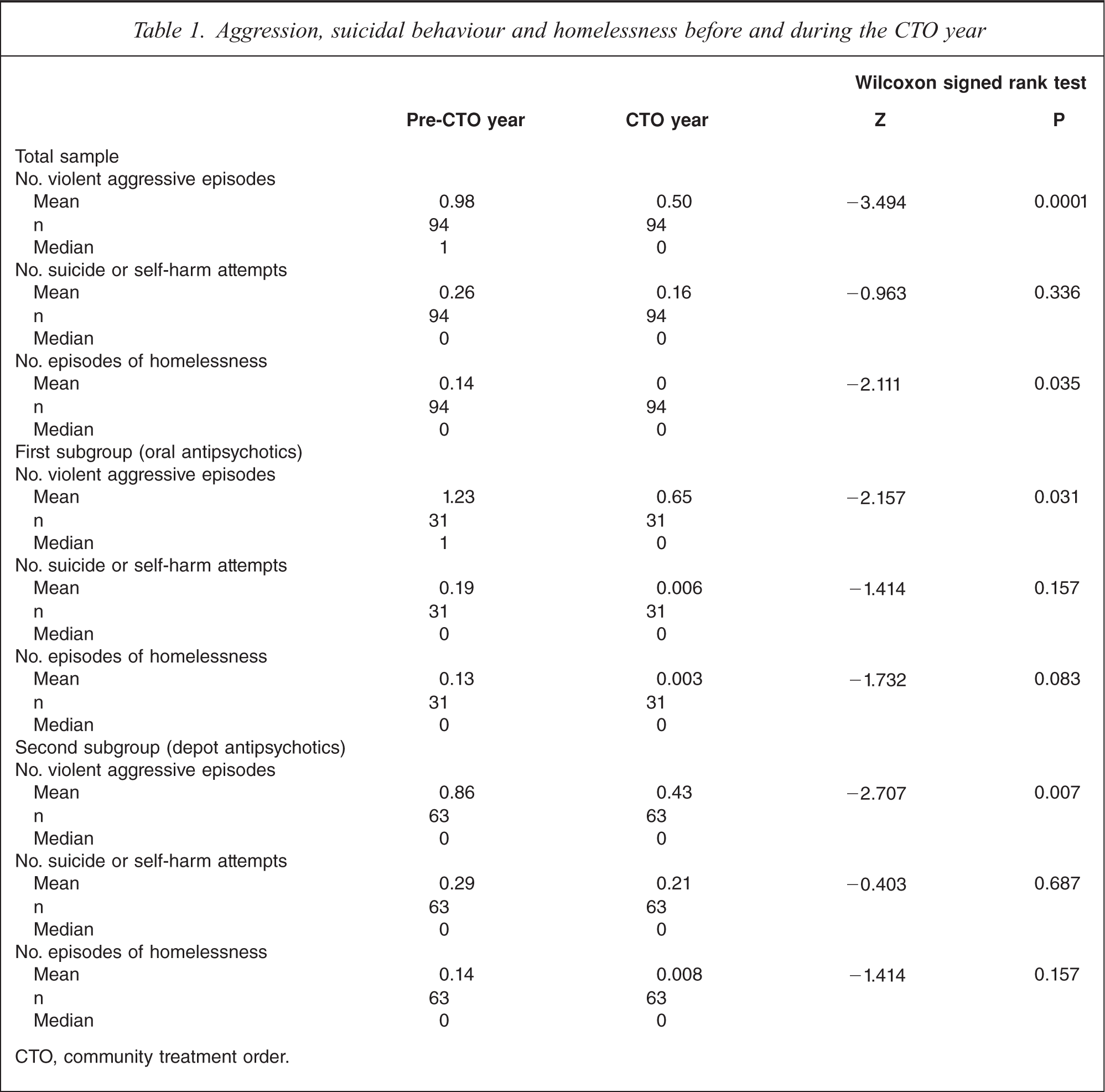
CTO, community treatment order.
There was no improvement in the frequency of contact between patient and family for the total, oral or the depot group (Table 2). Finally, there was little change in employment status for all three groups, although there was a trend towards fewer patients having fulltime work in the total and depot subgroups during the year of operation of the CTO (Table 3).
Frequency of contact with family before and during the CTO year
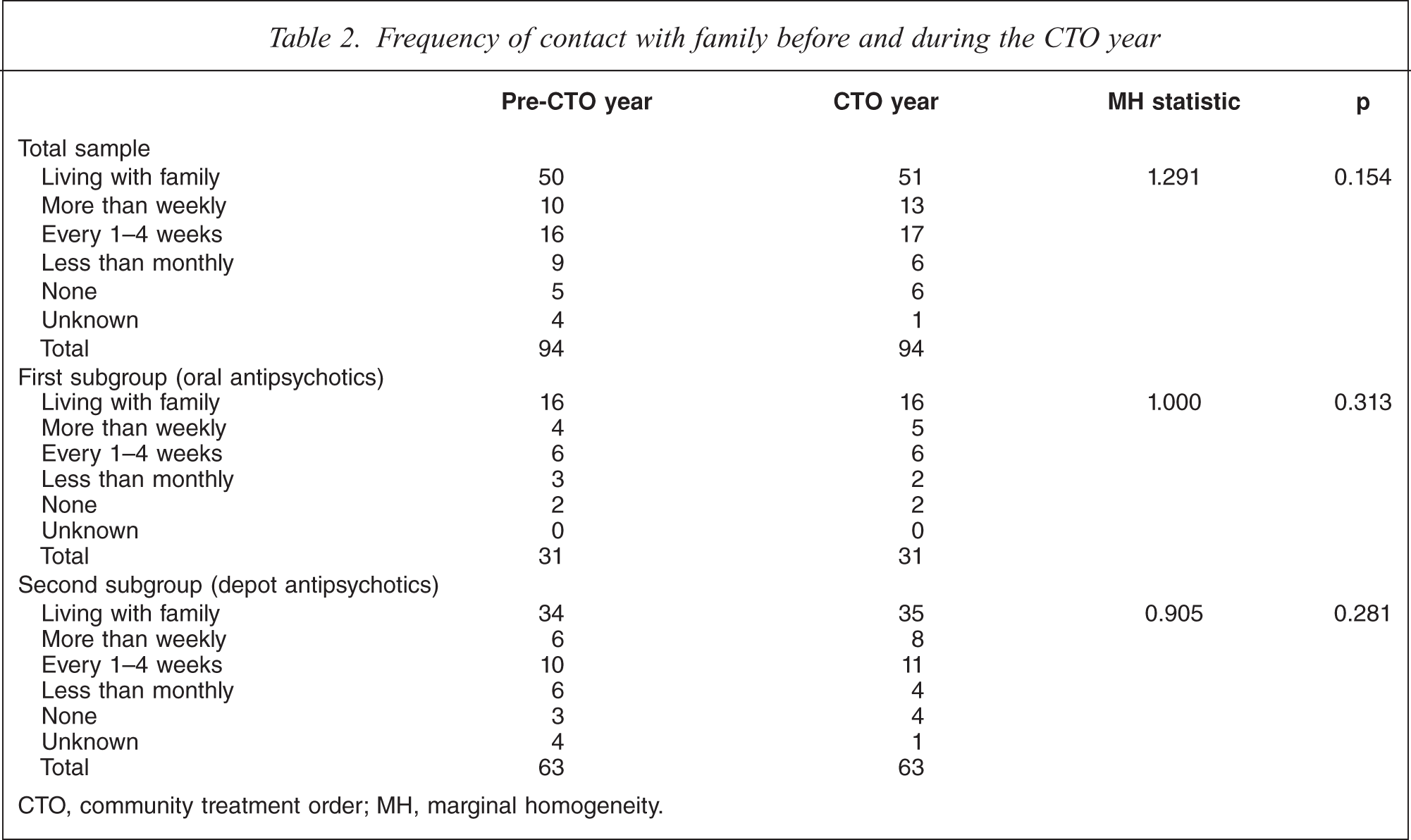
CTO, community treatment order; MH, marginal homogeneity.
Best employment status before and during the CTO year
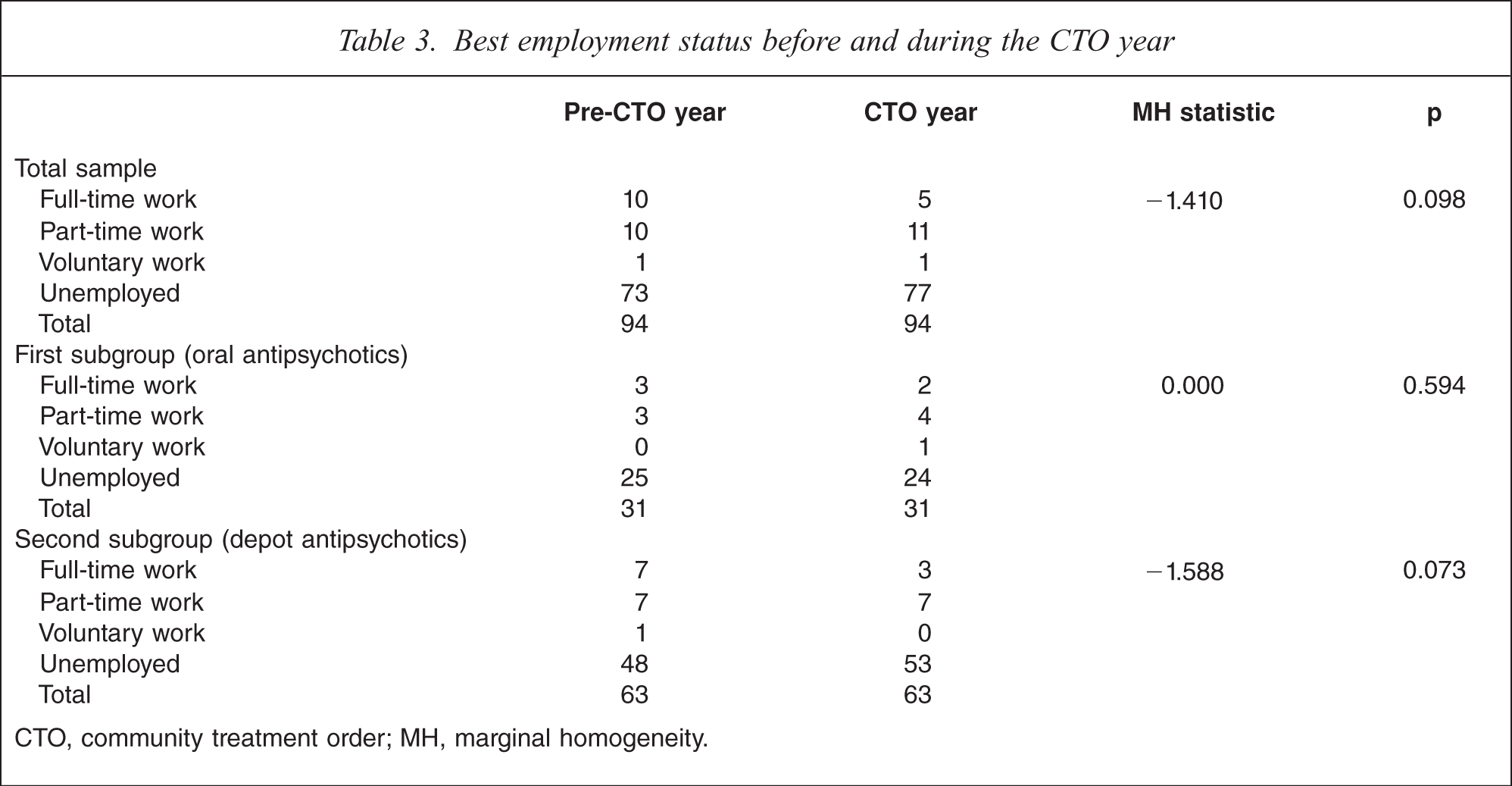
CTO, community treatment order; MH, marginal homogeneity.
Discussion
Strengths and limitations of the study
The strengths of this study include that it is a real-world study of rarely examined outcomes that may be associated with the use of CTOs. The study was conducted in a setting in which the use of CTOs is well-established. Further, there were few study exclusions. Limitations include the mirror image, retrospective design using relatively low numbers of case notes to obtain data. Also, some of these data are open to assessor bias. Interrater reliability for some outcomes is poor (notably quality of family relationships). We also note the relatively low rate of comorbid conditions (notably alcohol and drug abuse); there may be a problem in identifying comorbid conditions retrospectively from case notes due to poor documentation. There may be problems of regression to the mean affecting the outcomes, as outlined by Churchill et al. [19].
We have previously reported that CTOs may be effective in reducing relapse rates and time spent in hospital for selected persons with schizophrenia [1]. These results might be seen as suggestive of improved quality of life but provide only indirect support for such a notion. The present study examines whether there is improvement in measures that might provide preliminary evidence of enhanced social outcome and a reduction in problem behaviours (which are suggestive of enhanced quality of life). The present findings suggest that reduced periods of homelessness and reduced episodes of violence occur during treatment with a CTO compared with the preceding year without CTO treatment. Past justification for the use of CTOs has been sought on the grounds of decreasing risk (20–22), reducing relapses and reducing time spent in hospital, but these findings provide an argument for their potential value in improving social outcomes as well as reducing problem behaviours.
The present study showed a significant reduction in violence in all three patient subgroups during the CTO year. This replicates findings in other studies (9,23). Further, the New York State Office of Mental Health audit found a reduction in harmful behaviours in the first 6 months of a CTO [24].
Patients with schizophrenia had a significant reduction in homelessness in the CTO year. This is consistent with the findings of the New York State Office of Mental Health audit [24]. Homelessness is quite often associated with unemployment, poverty and social isolation, and particularly estrangement from family. It should be noted that the majority of patients in the present study lived with their families. This may also explain the lack of signifi-cant increase in family contact during the CTO year.
As we have previously reported [1], this postulated treatment effect of using a CTO might be mediated by increased clinical contact with the patient as well as increased medication adherence. We suggest that this might facilitate earlier intervention in the event of relapse, enabling therapeutic intervention before violence and other adverse events have occurred, including homelessness.
Episodes of self-harm and suicidal behaviours and changes in employment showed no improvement when comparing the pre- and post-CTO year. One explanation may be the low incidence of such events and a sample size that was insufficient to demonstrate any positive benefit. The slight worsening of overall employment status among the patients in the present study during the CTO year requires further investigation. It is plausible that regaining employment requires interventions in addition to the treatments that are most closely linked with the use of a CTO.
Ethical controversy has prevented the introduction of CTOs in Europe, although their introduction in England and Wales has occurred following their introduction in Scotland in 2005. A review for the UK Department of Health of international experience with CTOs highlighted that evidence of a positive treatment effect, for example reduction in length of stay in hospital, may not provide sufficient justification for CTO use without an additional appraisal of the associated benefits and harms [19]. The lack of robust randomized controlled trials as highlighted by Kisely et al. and Kisely and Campbell emphasizes that good-quality studies assessing efficacy of CTOs are lacking [25,26]. But as O’Reilly pointed out, this attitude may be slightly naïve in that assessment of CTOs hardly compares with assessment of a drug effect and is a more complex process requiring a more creative and flexible approach to methodology [27]. A further problem complicating comparison of studies is that the legislative framework supporting CTOs and the powers to intervene conferred on mental health services vary significantly between the different countries or jurisdictions where they have been introduced. Additionally there is substantial variation in the clinical procedures involved with how CTOs are implemented in clinical practice. The authors suggest that the evidence within the present study might be seen to mitigate concerns about the infringement of civil rights involved in the implementation of involuntary treatment in the community [2–4].
Conclusion
The present study reports on the reduced homelessness and reduced violent episodes that may be associated with the use of a CTO. The argument that CTOs may be effective is reinforced and could be seen to counterbalance concerns about infringement of civil rights. Further research into the impact of involuntary community treatment on quality of life is required, making use of larger samples and, where practicable, prospective and randomized designs.