
Abstract
Depression has been associated with cardiovascular disease in two principal ways, and with strong associations. Firstl, in leading to both fatal and non-fatal coronary artery disease (CAD) [1–3] and, specifically, to an increased risk of myocardial infarction (MI) [4]. Second, as depressive symptoms increase in the post-MI period so do mortality rates [5, 6], with a similar association demonstrated in depressed patients with unstable angina [7]. The association between depression and CAD is of similar magnitude to conventional risk factors such as smoking and hypercholesterolaemia [8]. Several explanations for such associations have been proposed. First, factors best viewed as consequences of depression, including poor compliance with cardiac therapies [9]. Second, differential treatment, with Druss et al. [10] suggesting that those with mental illness are less likely to receive cardiac procedures. Third, biological causes, such as abnormal platelet function [11, 12] and omega-3 polyunsaturated fatty acid deficiency [16].
We sought to pursue an alternate possibility. As ‘anxiety’ and ‘depression’ are highly correlated and as high trait anxiety (or ‘neuroticism’) disposes to both state anxiety and depression, we sought to consider the comparative influence of differing expressions of anxiety (and depression) on CAD morbidity. We now detail the logic for that proposition and our study design.
Prospective data in the Normative Aging Study [13] showed that high levels of worry were associated with an increased risk of CAD and higher baseline anxiety symptom scores with fatal CAD [14]. Carney et al. [15] identified an increased occurrence of ventricular tachycardia in patients with CAD and depression. Although an excessive heart rate is a physiological symptom of anxiety [16], a heightened sympathetic state in depression may lead to more premature ventricular contractions and low heart rate variability [17, 18], with low heart rate variability having been shown [19] to be predictive of sudden cardiac death. State anxiety levels of hospitalized patients with a myocardial infarct have been associated [20] with increased risk of ischemic and arrhythmic complications during their hospital stay. One review [21] established a high prevalence of panic disorder in CAD patients, allowing the possibility that panic disorder confers risk to and/or exacerbates CAD. Furthermore, whereas depression may have a prolonged mode of action on the occurrence of CAD, the psychophysiological effects of anxiety on CAD occurrence occur more acutely [22]. Finally, in a report published after we commenced our study, anxiety was identified as an independent predictor of cardiac events accounting for associations between depressive symptoms and prognosis following myocardial infarct. [23].
We therefore designed a study that, compared to previous CAD studies, investigated multiple manifestations of ‘anxiety’ and ‘depression’ to CAD morbidity, with the aim being to clarify the comparative influence of candidate variables.
Method
Overview
Patients admitted to the Cardiology unit at the Prince of Wales Hospital in Sydney with an acute coronary syndrome (ACS), including myocardial infarction (MI) and unstable angina, were all eligible for recruitment over the study period from May 2001 to July 2003. Our outcome ACS morbidity variables were to be 12-month rates of death, readmission for cardiac problems and recurrence of MI. This dictated (after estimation from the unit cardiologists) a minimum sample size of 400 subjects to have sufficient predictive power, but recruitment was extended for a period to ‘nest’ a final sample of 100 subjects for an ‘add on’ omega-3 polyunsaturated fatty acid study. The Cardiology unit provides basic care to the local government areas of Randwick, Botany and South Sydney, and tertiary services to both local and New SouthWales statewide patients (with the latter comprising about one-quarter of the referrals.
After admission, the patients underwent a baseline interview with a research assistant administering a structured diagnostic tool focusing on lifetime and current depressive and anxiety states. After the interview, the patients were also asked to complete a self-report questionnaire booklet assessing contributing psychological and psychosocial factors (as detailed shortly). Follow-up of subjects was to occur one month and 12 months following the baseline interview, and was designed to review depression variables and establish the patient's trajectory since baseline assessment—and thus the impact of cardiac state and other variables (particularly anxiety and depression) on survival, rehospitalization and both physical and psychological functioning.
All eligible subjects were asked to complete a brief one-page questionnaire designed to evaluate the possible presence of lifetime depression or anxiety. This allowed us to subsequently examine whether study ‘refusers’ differed in any significant way (in relation to their mood experience) compared to study participants.
Eligibility criteria
Primary eligibility criteria were a diagnosis of ACS as confirmed by a cardiologist, and included MIs with or without ST elevation, and unstable angina. The latter diagnosiswas confirmed by a more than 50% narrowing of more than one major coronary arteries from angiography results, whereas a diagnosis of MI was indicated by a rise in the blood troponin level—a standard maker of a myocardial infarction. Potential subjects were excluded if they did not speak English, were cognitively disabled, had visual or hearing impairments, or had a high mortality risk due to a severe medical condition (e.g. cancer, palliative care, severe congestive cardiac failure, severe renal failure). In addition, patients with a booked admission for a coronary artery bypass graft were also excluded.
Recruitment
Screening of potential participants was undertaken by Cardiology staff, who monitored admissions to the Cardiology department with the aim being for consecutive recruitment subject to staff availability and other factors. Cardiology staff identified 1630 patients admitted with either ACS, congestive cardiac failure (CCF) or atrial fibrillation (AF). Of these, 963 patients were approached by a research assistant between 0 and 22 days (mean=3.8 days; SD 3.0) after reaching a stable condition. Reasons for diagnostically eligible patients (albeit potentially ineligible on study criteria) not being approached included the patient being absent from the ward, having a medical procedure, having been admitted and discharged over a weekend or holiday periods when no research staff were available. There was no significant gender difference between those 1630 identified by Cardiology staff and the 963 approached (χ 2=3.03, p=0.082). There was, however, a slight difference in age between the two groups, with means of 69.4 years (SD=12.4) for those approached and 67.7 years (SD=13.5) for those not approached, significant (p=0.019) as a consequence of the large group numbers.
Of those approached, 59 patients had CCF and not ACS, 299 were excluded according to our criteria, 88 refused to participate, mostly due to self-reported fatigue and/or heightened anxiety and stress, 19 were deceased soon after being approached to participate and could not complete the study, and a further 9 patients started the study, but then withdrew. The remaining 489 patients met the inclusion criteria, had ACS and completed the study. After explanation of the study, all participants provided written consent. Of these, 452 patients had a primary diagnosis of ACS and a further 37 had CCF in addition to ACS. Table 1 reports the cardiac risk factors and diagnoses at discharge for all the 489 study subjects with ACS.
Ethics and informed consent
The study protocol was ratified by the Area Health Service and University of New South Wales ethics committees. A patient information statement detailed the study objectives and design for subjects, and written consent was obtained. If a participant was found to be suffering from significant depression or anxiety, this informationwas not released to the treating doctor without the participant informing us that he or she wished it to be known.
Data collection
Interviewing
A semi-structured clinical interview was conducted by one of four trained research assistants, lasting between 20 and 50 minutes, depending on each participant's history. This interview included the Composite International Diagnostic Interview (CIDI), version 2.154 Depression and Anxiety Disorder sections [24]. The CIDI was administered to rate lifetime and current presence of a major depressive episode, dysthymia, social phobia, agoraphobia, panic disorder, generalized anxiety disorder and obsessive-compulsive disorder according toDSM criteria. Patients that were currently depressed (at interview) and who had experienced two or more weeks of major depression and/or two or more years of dysthymia, were categorized as having current depression. That is, we imposed both DSM symptom and duration criteria to determine depression ‘caseness’. Those patients who might have developed clinical depression immediately before and/or after admission (and who met DSM major depression symptom but not duration criteria) were identified at the 1-month review and assessment period.
Research assistants also collected information on the use of antidepressant and anxiolytic medication, and risk factors for cardiovascular disease, including family history of cardiovascular disease, and participant risk variables (e.g. smoking, hypertension, hyperlipidaemia and diabetes). The patients' previous cardiac history was also charted on a time line with the sequence of onset of any episodes of depression and anxiety.
Self-report questionnaires
The self-report questionnaire booklet (containing nine measures) was administered immediately following the interview, commencing with sociodemographic variables. The 18-item Depression in the Medically Ill (DMI-18) measure [25], and validated in a cardiac population, assessed state depression, whereas the anxiety section of the Hospital Anxiety and Depression Scale (HADS) assessed state anxiety over the last 2 to 3 days in hospital [26]. A 15-item purpose-designed life events' measure examined life stressors (e.g. serious illness, legal problems, death of family member, death of friend) during the 12 months prior to admission—and the self-reported level of consequential stress (6-point assessment for events ‘overall’ and for the nominated event having the greatest impact). Social support was measured using the Multidimensional Scale of Perceived Social Support [27]. Neuroticism was assessed using the Eysenck Personality Questionnaire Revised (EPQ-R) Neuroticism subscale [28]. An additional personality measure developed by our unit (Parker et al., submitted) measured trait levels of internalized ‘anxious worrying’ and externalized ‘irritability’, as well as perfectionism, low self-esteem (‘self-criticism’), fear of abandonment and sociotropy (or need to please and rely on others). Five items from the Brief Measure of Worry Severity [29], as well as the consequences scale of the Illness Perception Questionnaire [30],which consists of 7 items assessing patients' perception of outcome of their cardiac condition, were administered. Finally, the 36-item Short Form Health Survey (SF-36) [31] was included to assess quality of life over the preceding four weeks.
Cardiac variables, medical details and biochemistry
Additional information was collected for each participant at baseline, detailing presenting cardiac symptoms, medical and/or psychiatric comorbidities, medications (beta-blockers, ACE-inhibitors, calcium channel blockers, long-acting nitrates, sedatives, anxiolytics and antidepressants), procedures, treatment or intervention in hospital, as well as medical complications and biochemical results. Left ventricular function and the number of diseased vessels on angiography were recorded at baseline as measures of disease severity. Biochemical analyses included troponin I, creatine phosphate, C-reactive protein and total cholesterol. Plasma phospholipid polyunsaturated fatty acid concentrations were also obtained for the final 100 participants.
One-month assessment and review
A 1-month assessmentwas undertaken to assess depression status (e.g. newincidence, duration of any depressive episode commencing around baseline admission) in the 4 weeks since assessment. This interview occurred over the telephone as a significant number of subjects were living outside of Sydney. Of the 489 subjects initially assessed, 11 had died and 11 were unable to be contacted. Thus, we obtained 1-month data on 97.8% of the available subjects.
End-points
The primary end-points for the study (when completed) will be cardiac-related death or myocardial infarct) with secondary end-points being cardiac-related hospital readmission, further non-MI ACS heart problems (e.g. angina), further cardiac procedures (e.g. revascularization), outpatient cardiologist contact, and quantified deterioration on the NewYorkHeartAssociation Functional Classification for CCF or deterioration on Canadian Cardiovascular Society Classification for angina. The principal follow-up period was 12 months after recruitment but we also anticipate a 3-year follow-up.
Results
In this paper, we report data on all patients assessed at baseline interview and depression ‘caseness’ data at the 1-month review. Of the 88 study refusers, 80 completed the screening form, with 26.3% indicating that they had suffered an episode of lifetime depression, 40.0% indicated they had suffered from anxiety or ‘nerves’ throughout their lifetime and 32.5% indicated they often felt worried or tense. As study participants also filled out the same questionnaire, we were therefore able to establish that no significant differences between refusers and acceptors were found for gender, lifetime depression frequency, depression before first cardiac problem, significant anxiety or ‘nerves’ over lifetime, worrying more than others or being a tense/highly strung person. Thus, study participants were unlikely to be disproportionately weighted to those with a high or low prevalence of depressive and/or anxiety disorders.
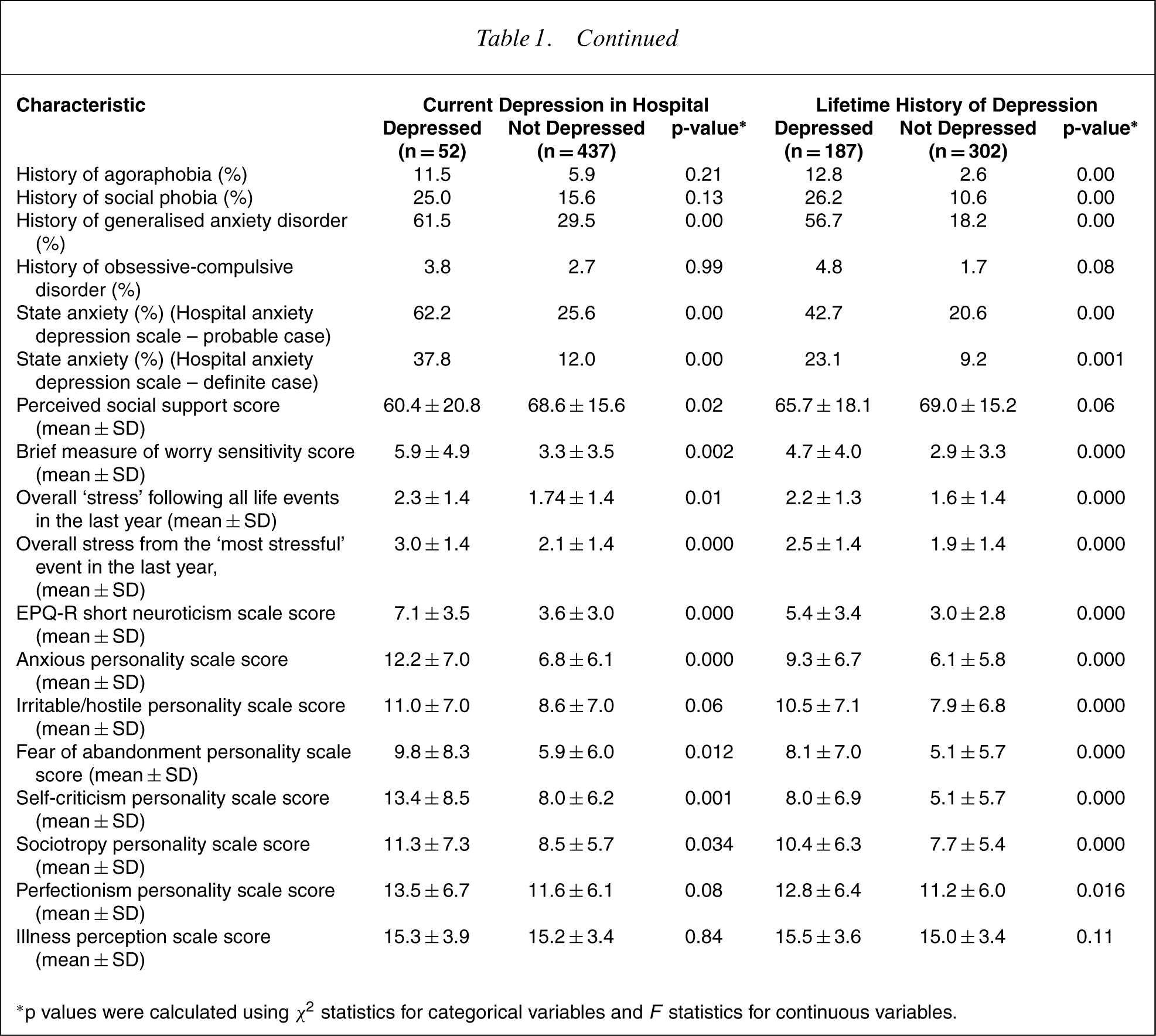
Table 1 considers baseline data on the 489 participants who had experienced an ACS (with constituent diagnoses tabulated), contrasting those rated as clinically depressed (Major Depression and Dysthymia) or non-depressed based on the CIDI interview. First, in relation to current depression (10.6% of the ACS subjects), those currently depressed did not differ from the non-depressed on any sociodemographic or cardiac diagnostic variable, or on any cardiac risk factor (other than being more likely to have had more previous admissions for CCF). They did, however, differ on nearly all psychosocial variables. In summary, they had distinctly higher levels of state anxiety, neuroticism, worry and life event-associated stress, scored higher on personality measures of internalized (‘anxious’) and externalized (‘irritable’) anxiety, self-criticism and perfectionism, as well as reporting lower levels of social support. They returned higher rates of all anxiety disorders assessed, but significant only for Panic Disorder and Generalized Anxiety Disorder.
Baseline characteristics of depressed and non-depressed patients during hospital admission for acute coronary syndrome (n = 489)
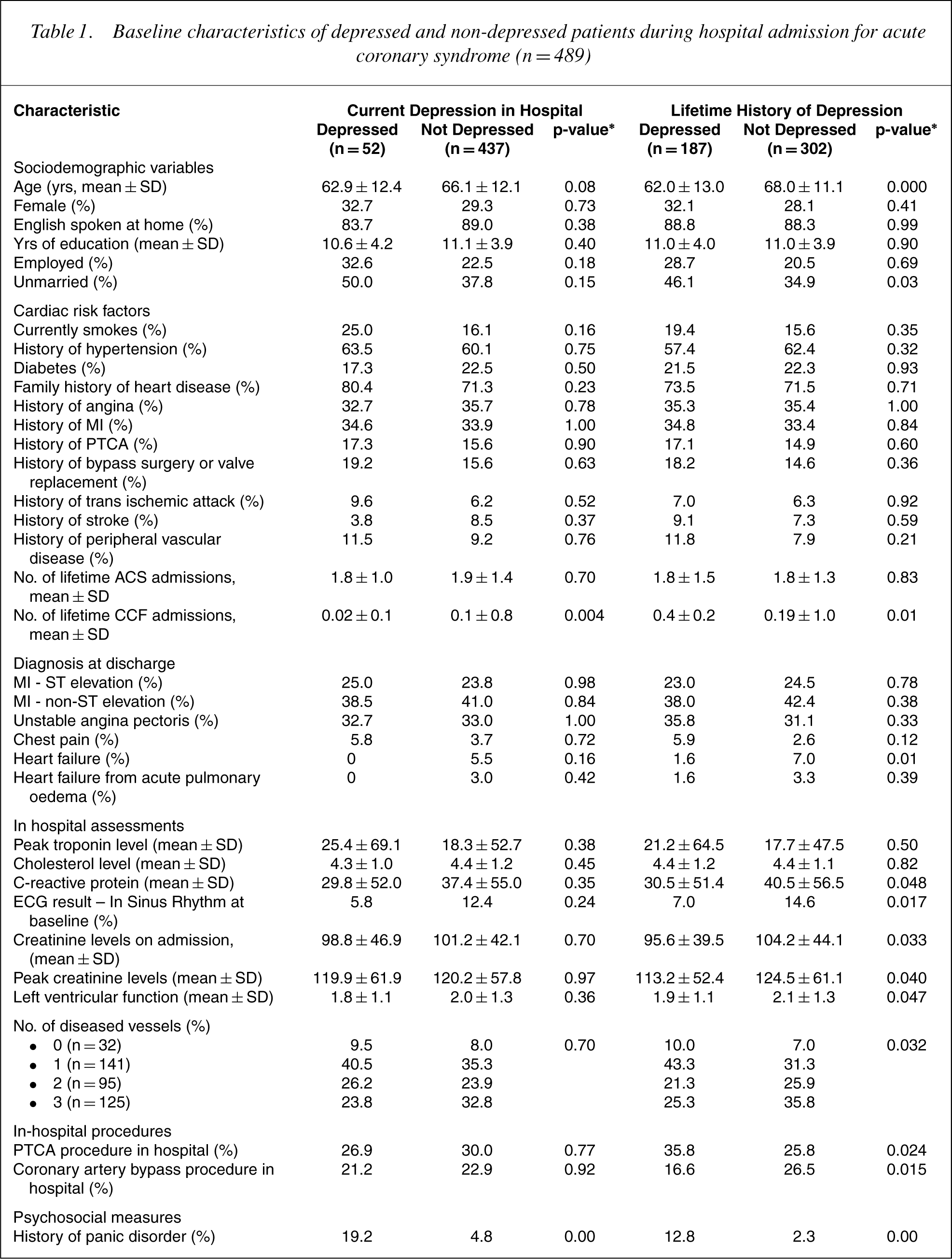
∗p values were calculated using X 2 statistics for categorical variables and F statistics for continuous variables.using
Table 1 data similarly contrast those who rated as having a lifetime episode of depression (38.3%) compared to residual subjects. Those with a history of lifetime depression were younger and less likely to be married. They had had fewer previous admissions to hospital for CCF and were less likely to have CCF at the baseline assessment, had lower C-reactive protein and creatine levels, fewer diseased vessels, better left ventricular function and were more likely to be in sinus rhythm when they had their electocardiogram in hospital. They were also more likely to have had a percutaneous transluminal coronary angioplasty procedure and less likely to have had a coronary artery bypass when in hospital. However, as they were significantly younger than the nondepressed group (by about 6 years on average), age may account for their better functional status on these variables. They were distinctly more likely to report greater anxiety on all CIDI-rated anxiety disorders apart from obsessive-compulsive disorder (which was just short of significance). They returned significantly higher scores on state anxiety, worry, neuroticism, life event-associated stress, as well as internalized and externalized levels of anxiety. They tended to report less social support, and scored higher on three personality styles having risk potential to depression (i.e. self-criticism, sociotropy and fear of abandonment), and also scored higher on a personality measure of perfectionism.
At the 1-month review 51 patients (10.7%) met criteria for major depression, 16 (3.3%) for dysthymia and 10 (2.1%) had major depression superimposed on dysthymia. Ignoring those patients with DSM-IV allocated minor depression (n=39) and bereavement (n=2), our 1-month rate for major depression and/or dysthymia was 16.1% for those assessed.
Discussion
This paper reports methodological nuances of a demanding study, whereby individuals with an acute coronary syndrome (ACS) were recruited over a 3-year period, and where short-term (1 month) and long-term (12 months and three years) review will examine whether post-ACS and lifetime depression status predicts death or significant cardiac morbidity. The study is designed to determine if such a long-standing and relatively consistent finding is replicated in an Australian sample. More importantly, we will pursue the hypothesis that certain expressions of anxiety (particularly trait anxiety) lead to an increased chance of post-ACS morbidity. If the latter is confirmed, we will undertake sequencing analyses (i.e. to what extent was ‘anxiety’ a predecessor of depression, a consequence or coterminous with depression), and seek to clarify the comparative contribution of ‘anxiety’ and of ‘depression’ to the onset of ACS (which will require recruitment of a control non-ACS sample) and to cardiac morbidity following ACS. Strengths of the study include the large sample size and the multi-dimensional and categorical expressions of anxiety and depression assessed.
Study findings can be briefly summarized. Of those screened, study refusers differed little from study acceptors, indicating that we obtained a representative sample, whereas analyses of those who were approached failed to identify distinct age and gender differences from the pool of potentially eligible subjects. One-third of the sample (38.3%) met the criteria for a lifetime episode of depression (major depression and/or dysthymia). There are no lifetime community estimates for the general Australian population but, in the recent US NCS Revised study [32] involving more than 9000 respondents, the lifetime rate for community subjects aged 60 years or olderwas 10.6% formajor depression, 1.3% for dysthymia, 1.0% for Bipolar I and II disorders and 11.9% for ‘any mood disorder’. Although our rate of lifetime depression appears high, until we make a comparison against an age- and sexmatched control sample of those without ACS, we are unable to comment as to whether our rate is distinctly higher, and confirming of the well-established finding that depression is a risk to CAD. We quantified a 10.6% prevalence rate for current depression in our ACS sample. However, as we imposed DSM duration criteria, this strategy would have excluded a percentage of individuals who developed clinical depression at or around the time of theirACS and admission, but did not meet the DSM duration criterion of 2 weeks. However, our 1-month review assessment (which established a prevalence of 16.5% for major depression and/or dysthymia) would have captured those individuals.
How do such rates compare with comparable studies? Sorensen et al. [33] recently reviewed 31 articles examining the impact of depression on post-myocardial infarction. In that data set, the prevalence rates of depression ranged from 1.5% to 50%, and when analyses were limited to studies using formalized case-finding techniques, prevalence rates ranged from 2% to 27%. Such ranges disallow any conclusion as to whether our rate is necessarily high or low when compared to previous studies. Our sample size (n=489) should be sufficient to allow the impact of depression on ACSmorbidity to be examined, when studies reporting such associations have comprised smaller samples. For example, the study by Frasure-Smith et al. [34] comprised 221 subjects, whereas there were 331 in the study by Kaufman et al. [35], 271 in the study by Bush et al. [5] and 153 in the study by Romanelli et al. [36].
The distinctly higher levels or rates of multiple expressions of anxiety (i.e. anxious personality, state anxiety, clinical anxiety disorders) in our lifetime and currently depressedACS subjects provides indirect support for pursuing the possible contribution of anxiety to both CAD and CAD morbidity. The role of anxiety has been examined in only a few studies. In one review [37], the authors considered five studies examining the impact of anxiety on post-ACS outcome, with four quantifying anxiety as exerting a significant risk (relative risk of 2.5, 2.5, 3.9 and 4.9). In a later review, Lane et al. [38] noted both the relatively few studies and their inconsistent findings. Furthermore, as noted earlier, whereas anxiety and depression were both individual predictors of outcome in the study by Strik et al. [23], only anxiety ‘survived in a multivariate analysis that tested both depression and anxiety’. In an intriguing review, Suls and Bunde [39] noted that as three ‘affective dispositions’ (i.e. depression, anxiety and anger-hostility) have been identified as putative risk factors for CAD, there is the need to develop ‘more complex affect-disease models’, and that the overlap of the three constructsmight argue that a general disposition of ‘negative affectivity’ may be more important than any specific affect. Our study, comprising multiple measures of anxiety and anxious personality styles, allows that hypothesis to be tested. In our subsequent analyses, it will be of particular importance to determine if associations between depression and ACS remain after controlling for differing expressions of anxiety.
Our principal analyses will seek to determine which study variables are associated with an increased chance of post-ACS mortality and cardiac morbidity at a 1-year follow-up and, respecting their interdependence, determine the higher-order variable. More finely focused analyses will examine the moderating impact of a range of possible mediating factors, including psychosocial factors (e.g. life event stress, social support, personality variables), cardiac variables (as detailed here), sociodemographic variables (e.g. gender), dietary factors (e.g. fish consumption) and treatment variables (e.g. exposure to antidepressant drugs, cardiac strategies). This methodological paper details both the argument for broadening the inquiry from ‘depression’ per se and provides suggestive data implicating a link whereby anxiety as much as to depression may dispose to cardiac morbidity.
Footnotes
Acknowledgements
This study was supported by an NHMRC Program Grant (222708) and an Infrastructure Grant from the NSW Department of Health. We thank Penny Sawdy for data coding. We would like to thank Geane Sharman, Marissa Anne Greco, Marisa Madigan and Anne Russell from the Department of Cardiac Services' Clinical Trials office for help with data entry and patient screening.