
Abstract
Objective:
Major depressive disorder commonly co-occurs with one or more anxiety disorders or with clinically significant levels of anxiety symptoms. Although evidence suggests that anxious forms of depression are prognostic of poorer antidepressant outcomes, there is no clear definition of anxious depression, and inferences about clinical outcomes are thus limited. Our objective was to compare and evaluate definitions of anxious depression and anxiety-related scales according to clinical and antidepressant outcome criteria.
Method:
A total of 1008 adults with a current diagnosis of single-episode or recurrent, nonpsychotic, major depressive disorder were assessed at baseline on clinical features. Participants were then randomised to one of three antidepressants and reassessed at 8 weeks regarding remission and response of the 17-item Hamilton Rating Scale Depression (HRSD17) and the 16-item Quick Inventory of Depressive Symptomatology (QIDS-SR16). Anxious depression was defined as major depressive disorder with one or more anxiety disorders or major depressive disorder with a HRSD17 anxiety/somatisation factor score ⩾7. Anxiety-related scales included the HRSD17 anxiety/somatisation factor and the 42-item Depression Anxiety Stress Scales (DASS42) anxiety and stress subscales.
Results:
Anxious depression definitions showed poor agreement (κ = 0.15) and the HRSD17 anxiety/somatisation factor was weakly correlated with both DASS42 anxiety (r = 0.24) and stress subscales (r = 0.20). Anxious depression definitions were also associated with few impairments on clinical features and did not predict poorer antidepressant treatment outcome. However, higher DASS42 anxiety predicted poorer HRSD17 and QIDS-SR16 remission, and item-level analysis found higher scores on items 9 (situational anxiety) and 23 (somatic anxiety) of the DASS42 predicted poorer treatment outcome, even after adjusting for covariates and multiple comparisons.
Conclusion:
Common definitions of anxious depression show poor agreement and do not predict poorer treatment outcome. Anxiety symptoms may be better characterised dimensionally using DASS42 when predicting treatment outcome.
Keywords
Anxiety disorders and clinically significant levels of anxiety symptoms co-occur in approximately half the major depressive disorder (MDD) population (Gaspersz et al., 2018; Ionescu et al., 2013). These anxious forms of depression have been associated with more severe illness and poorer antidepressant treatment outcomes (Ionescu et al., 2013, 2014). However, the validity and interpretability of associated clinical outcomes have been limited by the diversity of criteria used when characterising anxiety and defining anxious depression (Gaspersz et al., 2018; Ionescu et al., 2013).
Ionescu et al. (2013) reviewed the most common definitions of anxious depression and their associated clinical outcomes. The authors suggested that either a syndromal or a dimensional approach best differentiated anxious from non–anxious depression on clinically relevant measures. The syndromal approach was defined as MDD comorbid with at least one anxiety disorder. Syndromal anxious depression was associated with an earlier onset, more severe depressive episodes, and worse physical, social, and occupational outcomes (Ionescu et al., 2013). The dimensional approach was most commonly defined as MDD comorbid with a score of ⩾7 on the anxiety/somatisation factor of the 17-item Hamilton’s Rating Scale for Depression (HRSD17; Cleary and Guy, 1977). Dimensional anxious depression was characterised by longer current depressive episodes, more concurrent anxiety disorders, more medical comorbidities and more melancholic/endogenous features, even after adjusting for severity of depression (Fava et al., 2004, 2006, 2008). The authors concluded dimensionally defined anxious depression was characterised by poorer clinical outcomes and was more clinically relevant than the syndromal definition (Ionescu et al., 2013).
Gaspersz et al. (2018) extended Ionescu et al. (2013) review by including more recent studies and the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) anxious distress specifier definition (i.e. MDD and at least two out of five anxious symptoms). People with anxious depression were associated with poorer course trajectories and worse clinical outcomes, which included having a greater depression severity, higher suicidal risks, lower quality of life, and impaired social and occupational functioning compared to their non-anxious counterparts (Gaspersz et al., 2018). However, the anxious distress specifier has been shown to have poor agreement with both the syndromal (κ = 0.09) and dimensional definitions (κ = 0.21; Gaspersz et al., 2017). The anxious distress specifier has also been shown to be only moderately correlated with the HRSD17 anxiety/somatisation factor score (r = 0.50; Zimmerman et al., 2018). In addition to the anxious distress specifier, other common measures of anxiety have been shown to be associated with treatment outcome.
The Depression Anxiety Stress Scale (DASS) is a self-reported scale designed to measure the three related negative emotional states of depression, anxiety, and stress (Lovibond and Lovibond, 1995). The DASS anxiety subscale corresponds most closely to the symptom criteria for the various anxiety disorders, except for generalised anxiety disorder (GAD), which is covered by the DASS stress subscale (Brown et al., 1997; Gloster et al., 2008). In the International Study to Predict Optimised Treatment in Depression (iSPOT-D) trial, DASS anxiety was the only baseline characteristic associated with poor antidepressant treatment outcome, independent of depressive severity, diagnostic comorbidity, or side effects (Saveanu et al., 2015). Together, these results suggest that the DASS anxiety and stress subscales characterise anxiety-related symptoms with a clinical use for predicting antidepressant treatment outcome.
The aim of this study was to compare and evaluate common definitions of anxious depression and anxiety-related scales, in the same well-powered patient sample, according to external clinical and antidepressant outcome criteria. Definitions were evaluated in a large patient sample from the iSPOT-D study who were unmedicated at the pre-treatment baseline and then randomised to one of three antidepressants (Williams et al., 2011). We hypothesised that, in line with Gaspersz et al. (2017) and Zimmerman et al. (2018), there would be low agreement between anxious depression definitions and weak correlations between anxiety-related scales. We also hypothesised that, in line with Ionescu et al. (2013) and Gaspersz et al. (2018), people with HRSD17 defined anxious depression would show poorer clinical outcomes compared to people with syndromal anxious depression. Finally, given the DASS anxiety and stress subscales assess a wider range of anxiety-related symptoms, are self-reported and have been associated with poor treatment outcome (Lovibond and Lovibond, 1995; Saveanu et al., 2015), we hypothesised the DASS anxiety and stress subscales would be associated with poor antidepressant treatment outcome.
Method
Study overview
The International Study to Predict Optimised Treatment for Depression (iSPOT-D) is a phase-IV, multi-site, international, randomised, open-label trial designed to identify markers of treatment response to commonly prescribed medications in an adult depressed, outpatient population. All participants were either antidepressant medication naive or washed out. Assessments were collected at pre-treatment and post-treatment at 8 weeks. The iSPOT-D trial was designed with no placebo arm and participants were aware of the medication that they were taking to best match real-world practice. In this way, findings also reflect treatment regimens that exist in routine practice and promote the translatability of the findings. For more details on the study protocol design, rationale and methods, see Williams et al. (2011).
Participants
Participants (N = 1008) were adults (18–65 years old) with a current diagnosis of single-episode or recurrent, nonpsychotic, MDD as diagnosed on the Mini-International Neuropsychiatric Interview–Plus (MINI-Plus; Sheehan et al., 1998) according to the DSM-IV criteria (American Psychiatric Association, 1994; see CONOSRT chart, Supplementary Figure 1). All participants required a 17-item HRSD17 score >16 at entry. Participants provided written informed consent after receiving a complete description of the study. The study was approved by institutional or ethical review boards at each site, and its protocols followed International Conference on Harmonisation and Good Clinical Practice principles, the US Food and Drug Administration Code of Federal Regulations, the Helsinki Declaration of 1975 (as revised in 2008) and country-specific guidelines.
Protocol treatment
Participants were randomised to receive escitalopram, sertraline, or venlafaxine-extended release (venlafaxine-XR) with equal probability. All psychotropic medications (except sleep aids and anxiolytics) were discontinued and washed out prior to baseline assessments. Antidepressants were prescribed and doses were adjusted by the participant’s treating physician according to routine clinical practice. Additional medication for associated symptoms (e.g. insomnia) or medication-induced side effects (e.g. nausea) were allowed as they reflect common practice. Any treatment for concurrent general medical conditions, except medications contraindicated with the study-assigned antidepressants, were allowed and recorded.
Baseline measures
Clinical features
Symptom severity scores were assessed at baseline by research assistants independent of the prescribing clinicians using the HRSD17 (Hamilton, 1960), the self-rated 16-item Quick Inventory of Depressive Symptomatology (QIDS-SR16; Rush et al., 2003; Trivedi et al., 2004) and the self-rated 42-item Depression Anxiety and Stress Scale (DASS42; Lovibond and Lovibond, 1995). The anxiety subscale includes 14 items measuring autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious affect. The stress subscale includes 14 items measuring difficulty relaxing, nervous arousal, and being easily upset/agitated, irritable/over-reactive and impatient. Sociodemographic measures were collected as part of the clinical interview and included age, sex, years of education and race. Family history of illness, early life stress (ELS) events, relationship status and work status were collected in computer-based self-report questionnaires. Course of illness and comorbidities were collected at baseline using the MINI-Plus (Sheehan et al., 1998).
Psychological profile
Psychological profile was assessed using the self-reported NEO-Five Factor Inventory (NEO-FFI; Costa and Mccrae, 1989) and Emotion Regulation Questionnaire (ERQ; Gross and John, 2003). The NEO-FFI is a 60-item questionnaire that examines five personality traits: openness, contentiousness, extraversion, agreeableness and neuroticism. The ERQ is a 10-item scale designed to measure respondents’ tendency to regulate their emotions through cognitive reappraisal and expressive suppression.
Functional capacity and Quality of Life
Functional capacity was assessed using the clinician-rated Social and Occupational Functioning Assessment Scale (SOFAS; Goldman et al., 1992) and the self-report World Health Organization Quality Of Life (WHOQOL)-BREF scale (Harper et al., 1998). The SOFAS is a continuous scale ranging from 0 to 100 that rates social and occupational functioning from excellent functioning to grossly impaired functioning. The WHOQOL-BREF is a 26-item questionnaire assessing quality of life in four domains: physical health, psychological, social relationships and environments.
Resilience and wellbeing
Resilience and wellbeing was assessed using the self-report Brief Risk-Resilience Index for Screening (BRISC; Williams et al., 2012) assessment, the Satisfaction with Life Scale (SWLS; Diener et al., 1985), and the composure, positivity, achieving and satisfaction subscales of the Composure Own-worth Mastery Positivity Achieving Satisfaction-Wellbeing (COMPAS-W; Gatt et al., 2014) scale. The BRISC is a 45-item scale assessing three core domains of self-regulation: negativity bias, emotional resilience and social skills. The SWLS is a 5-item scale designed to measure global cognitive judgements of one’s life satisfaction. The COMPAS-W is a 26-item scale that measures both subjective and psychological wellbeing in the domains of composure, own-worth, mastery, positivity, achieving and satisfaction.
Anxious depression definitions
Syndromal anxious depression
Syndromal anxious depression was defined as a DSM-IV MDD diagnosis and one concurrent MINI-Plus identified anxiety disorder (23.8%, 261/1005), including generalised anxiety disorder, panic disorder, agoraphobia, social phobia and specific phobia (Ionescu et al., 2013).
HRSD anxious depression
HRSD anxious depression was defined as a DSM-IV MDD diagnosis and a HRSD17 anxiety/somatization factor score of ⩾7 (41.9%, 422/1008; Ionescu et al., 2013). The anxiety/somatisation factor was derived from a factor analyses of the HRSD17 by Cleary and Guy (1977) and includes six items: hypochondriasis, insight, general and gastrointestinal somatic symptoms, and psychic and somatic anxiety.
Post-treatment measures
Outcome measures were remission and response. Remission was defined as a week 8 HRSD17 score <7 or a week 8 QIDS-SR16 score <5 (Rush et al., 2003; Trivedi et al., 2004). Response was defined as a >50% decrease from baseline on the HRSD17 or QIDS-SR16. Study site personnel contacted participants by telephone at day 4 and weeks 2, 4 and 6 to monitor antidepressant dosage, compliance, concomitant medications and adverse events.
Statistical analysis
Missing baseline data (<10%) were imputed using multivariate imputation by chained equations (MICE, where m = 10), a multiple imputation technique able to handle both continuous and categorical data (Van Buuren and Groothuis-Oudshoorn, 2011). Models were run on each imputed dataset and then combined according to Rubin’s (1987) rule. However, to avoid predicting group membership, people with missing data on measures used to create definition groups (n = 3) were first excluded.
Cohen’s kappa coefficients were used to assess agreement between anxious depression definitions. Bivariate logistic regression models were used to test whether baseline measures predicted anxious depression for each anxious depression definition and whether anxious depression predicted antidepressant dosage or treatment outcome. All models were also adjusted for age, sex, years of education, study site, depression severity (as measured by the HRSD17 score with items from the anxiety/somatisation factor removed), recurrent MDD and sleep aids/anxiolytics to assess whether the results occurred independent of these covariates. Multiple comparisons for planned analyses were controlled for using the Benjamini and Hochberg (1995) procedure. Multiple comparisons for post hoc tests were controlled for using the Holm (1979) method, a method uniformly more powerful than the Bonferroni method.
All analyses were conducted using R 3.5.1 (R Core Team, 2018). Cohen kappa coefficients were calculated using the ‘rel’ package in R (Martire, 2017). Multiple imputation was performed using the ‘mice’ package in R (Van Buuren and Groothuis-Oudshoorn, 2011).
Results
Demographics
Table 1 provides the covariate demographics for the iSPOT-D sample and anxious depression groups. Definition group mean ages ranged between 37.02 (standard deviation [SD] = 13.16; HRSD anxious depression) to 38.44 (SD = 12.11; HRSD non-anxious depression). People with syndromal anxious depression were significantly less educated (p < 0.001), had less cases of recurrent MDD (p = 0.004) and used more sleep aids/anxiolytics (p = 0.011) compared to their non-anxious counterparts. People with HRSD anxious depression were significantly more depressed than their non-anxious counterparts (p < 0.001).
Covariate demographics for the iSPOT-D sample and anxious depression groups.
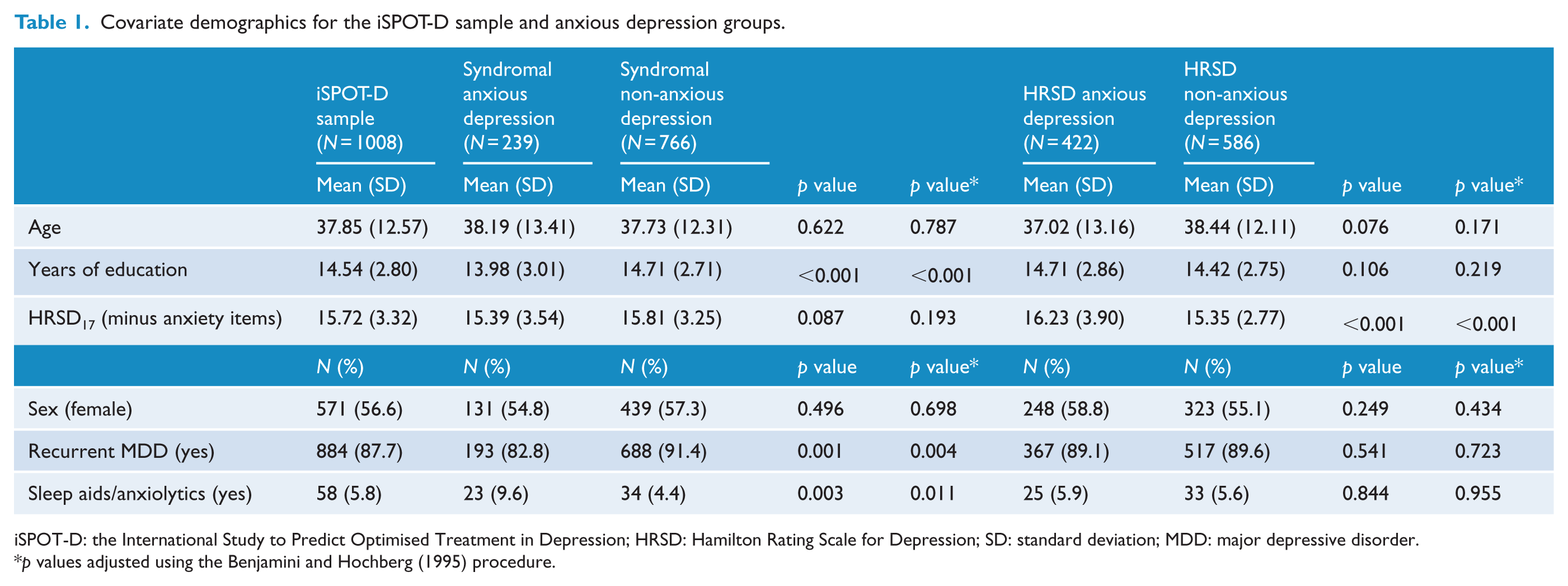
iSPOT-D: the International Study to Predict Optimised Treatment in Depression; HRSD: Hamilton Rating Scale for Depression; SD: standard deviation; MDD: major depressive disorder.
p values adjusted using the Benjamini and Hochberg (1995) procedure.
Definition overlap and anxiety scale correlations
Figure 1 provides an area proportional Venn diagram showing overlap between anxious depression definitions. 52.4% (528/1008) of the iSPOT-D sample met criteria for at least one anxious depression definition and 47.6% (480/1008) did not meet criteria for any anxious depression definition. 0.002% (3/1008) could not be assigned to at least one definition group due to missing data. 23.8% (261/1005) met the criteria for syndromal anxious depression, 41.9% (422/1008) met criteria for HRSD anxious depression and 13.2% (133/1008) of participants met criteria for both definitions of anxious depression. There was low agreement between the syndromal and HRSD definitions (κ = 0.15, 95% confidence interval [CI = 0.09, 0.20], p < 0.001). The HRSD17 anxiety/somatisation factor was also weakly, but significantly correlated with the DASS anxiety (r = 0.24, p < 0.001) and stress (r = 0.20, p < 0.001) subscales.
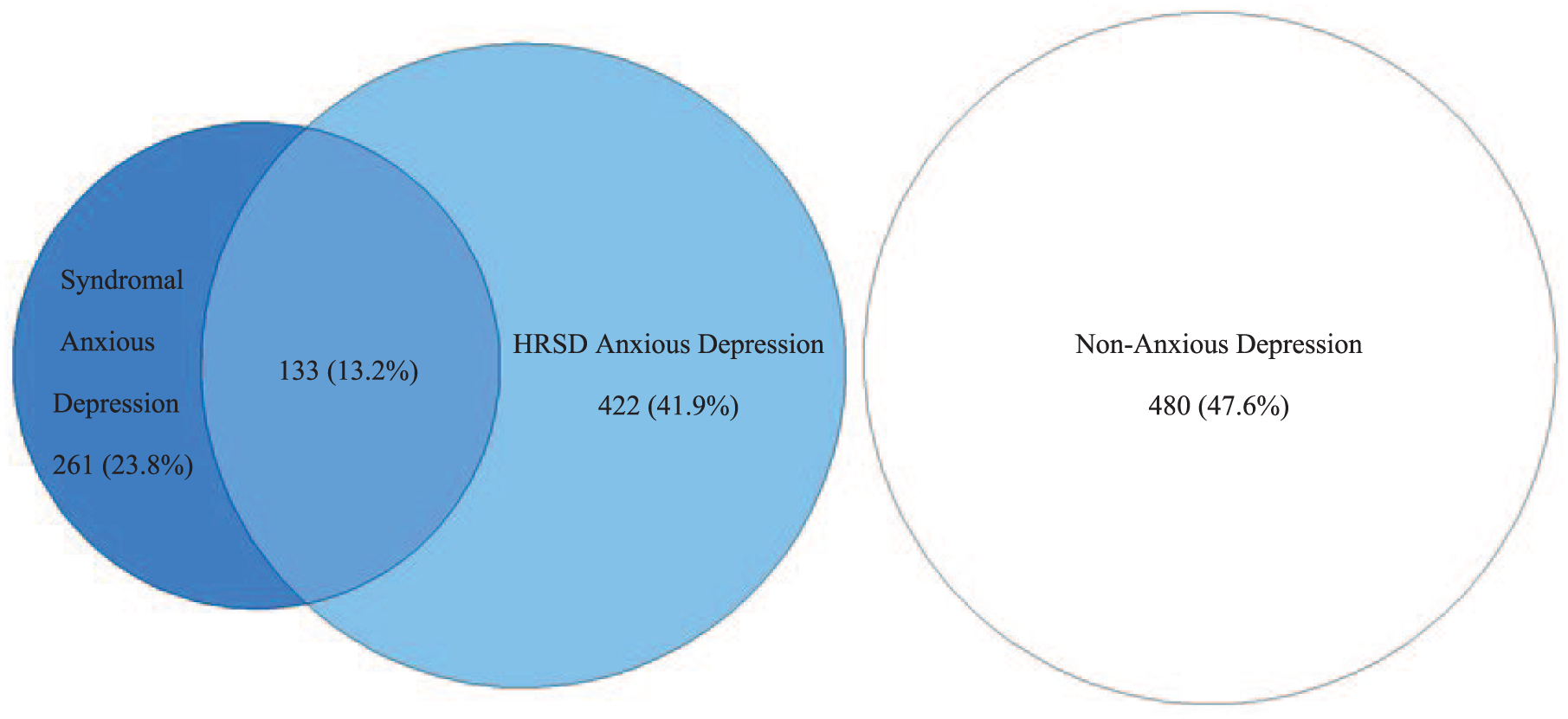
Area proportional Venn diagram showing overlap between anxious depression definitions.
Baseline measures
Table 2 provides the results of significant covariate and multiple comparison–adjusted logistic regression models testing whether baseline measures significantly predicted syndromal and HRSD anxious depression (see Supplementary Tables 1 and 2 for all results). Syndromal anxious depression was associated with lower scores on the SOFAS (p = 0.004), NEO-FFI Extraversion (p = 0.034), BRISC Negativity Bias (p < 0.001), COMPAS-W Composure (p = 0.022) and Satisfaction (p = 0.017) scales, and higher scores on the QIDS-SR16 (p = 0.007), DASS stress (p < 0.001) and DASS anxiety (p < 0.001) scales.
Results of significant covariate and multiple comparison–adjusted logistic regression models testing whether baseline measures significantly predicted syndromal and HRSD anxious depression.
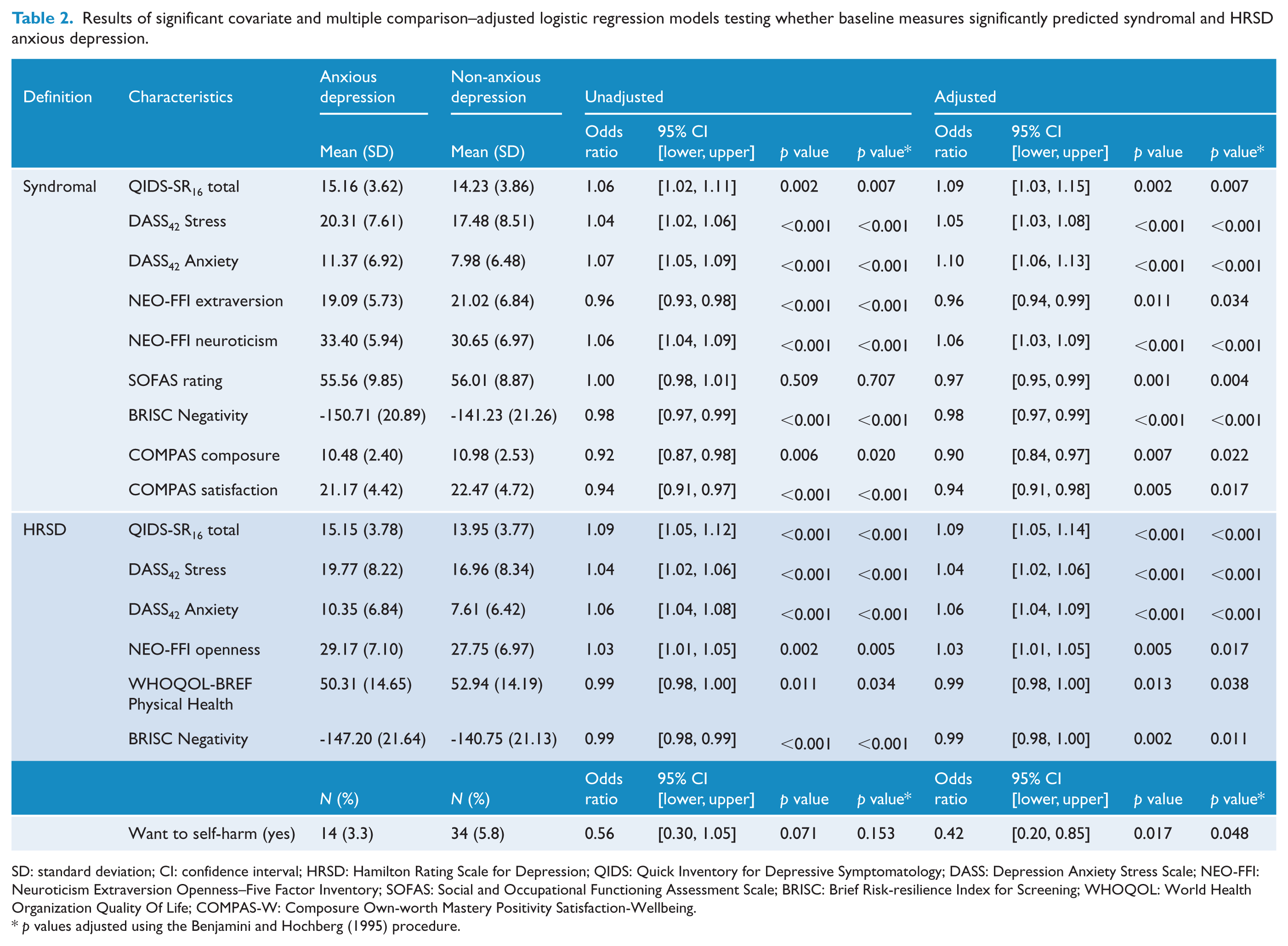
SD: standard deviation; CI: confidence interval; HRSD: Hamilton Rating Scale for Depression; QIDS: Quick Inventory for Depressive Symptomatology; DASS: Depression Anxiety Stress Scale; NEO-FFI: Neuroticism Extraversion Openness–Five Factor Inventory; SOFAS: Social and Occupational Functioning Assessment Scale; BRISC: Brief Risk-resilience Index for Screening; WHOQOL: World Health Organization Quality Of Life; COMPAS-W: Composure Own-worth Mastery Positivity Satisfaction-Wellbeing.
p values adjusted using the Benjamini and Hochberg (1995) procedure.
HRSD anxious depression was associated with lower scores on the WHOQOL-BREF Physical Health (p = 0.038) and BRISC Negativity Bias (p < 0.011) scales, and higher scores on the QIDS-SR16 (p < 0.001), DASS stress (p < 0.001), DASS anxiety (p < 0.001) and NEO-FFI Openness (p < 0.001) scales. People with HRSD anxious depression also had lower proportions of people wanting to self-harm (p = 0.048).
Anxious depression definitions predicting treatment outcome
Anxious depression definitions did not interact with antidepressant treatment type in predicting treatment outcome (see Supplementary Table 3), so treatments were pooled together. Table 3 provides the results from unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether anxious depression predicted HRSD17 or QIDS-SR16 remission or response. Syndromal anxious depression predicted better QIDS16 response after adjusting for covariates (p = 0.011) and multiple comparisons (p = 0.034). HRSD anxious depression predicted poorer HRSD17 remission before (p = 0.030), but not after adjusting for covariates (p = 0.275). Importantly, anxious depression did not predict study dropout or interact with treatment type in predicting study dropout (see Supplementary Table 4).
Results from unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether anxious depression predicted HRSD17 or QIDS-SR16 remission or response.
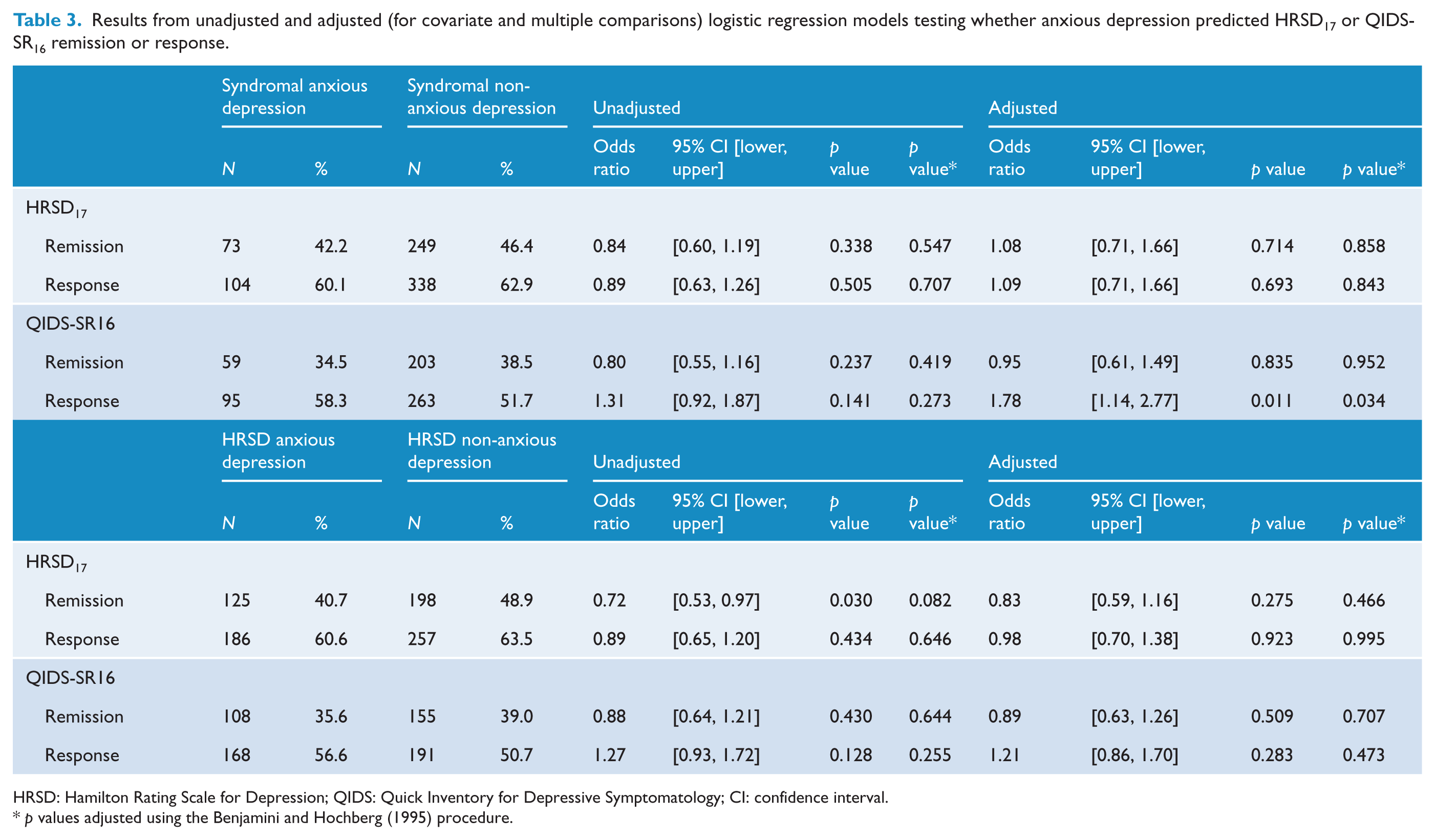
HRSD: Hamilton Rating Scale for Depression; QIDS: Quick Inventory for Depressive Symptomatology; CI: confidence interval.
p values adjusted using the Benjamini and Hochberg (1995) procedure.
Anxiety scales predicting treatment outcome
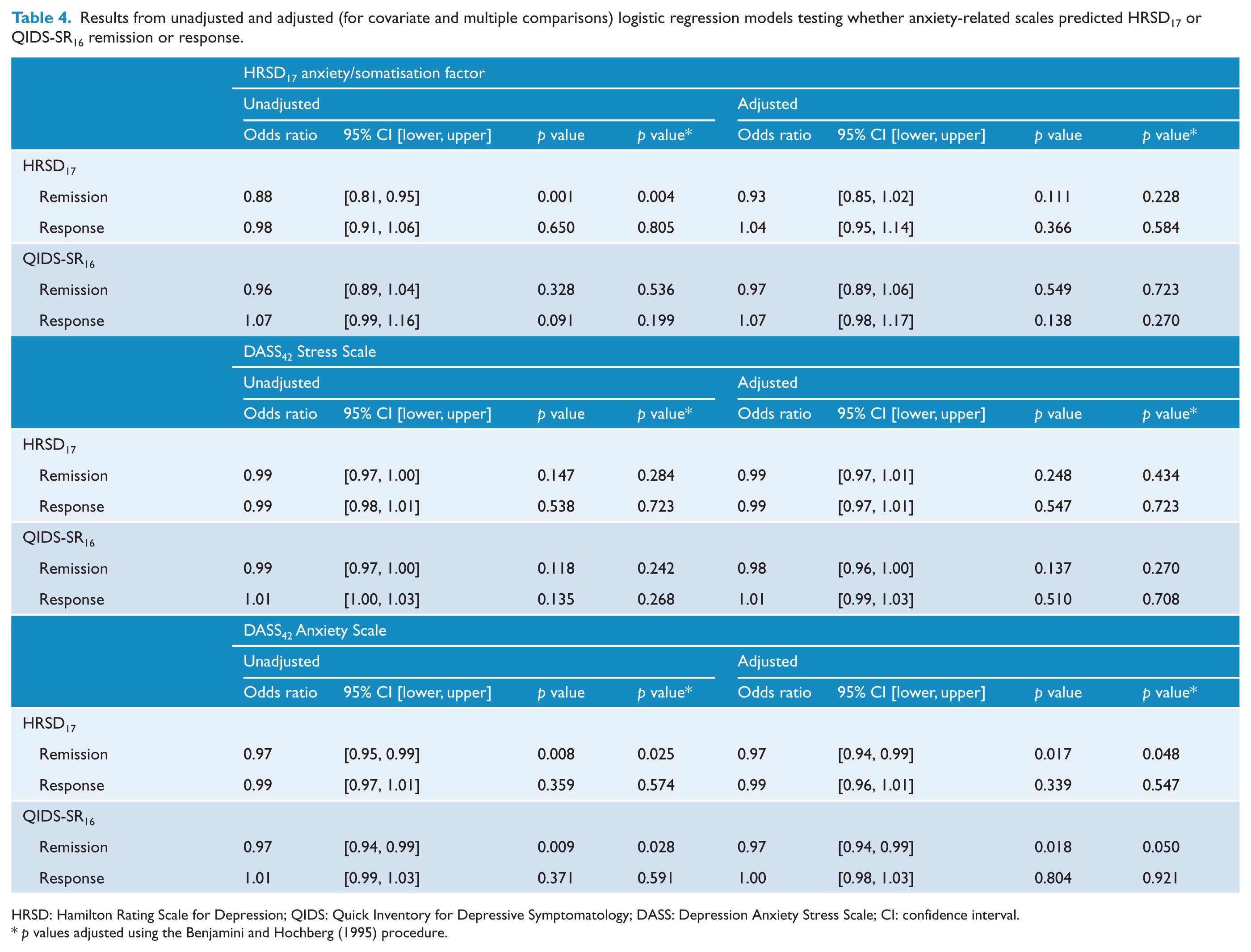
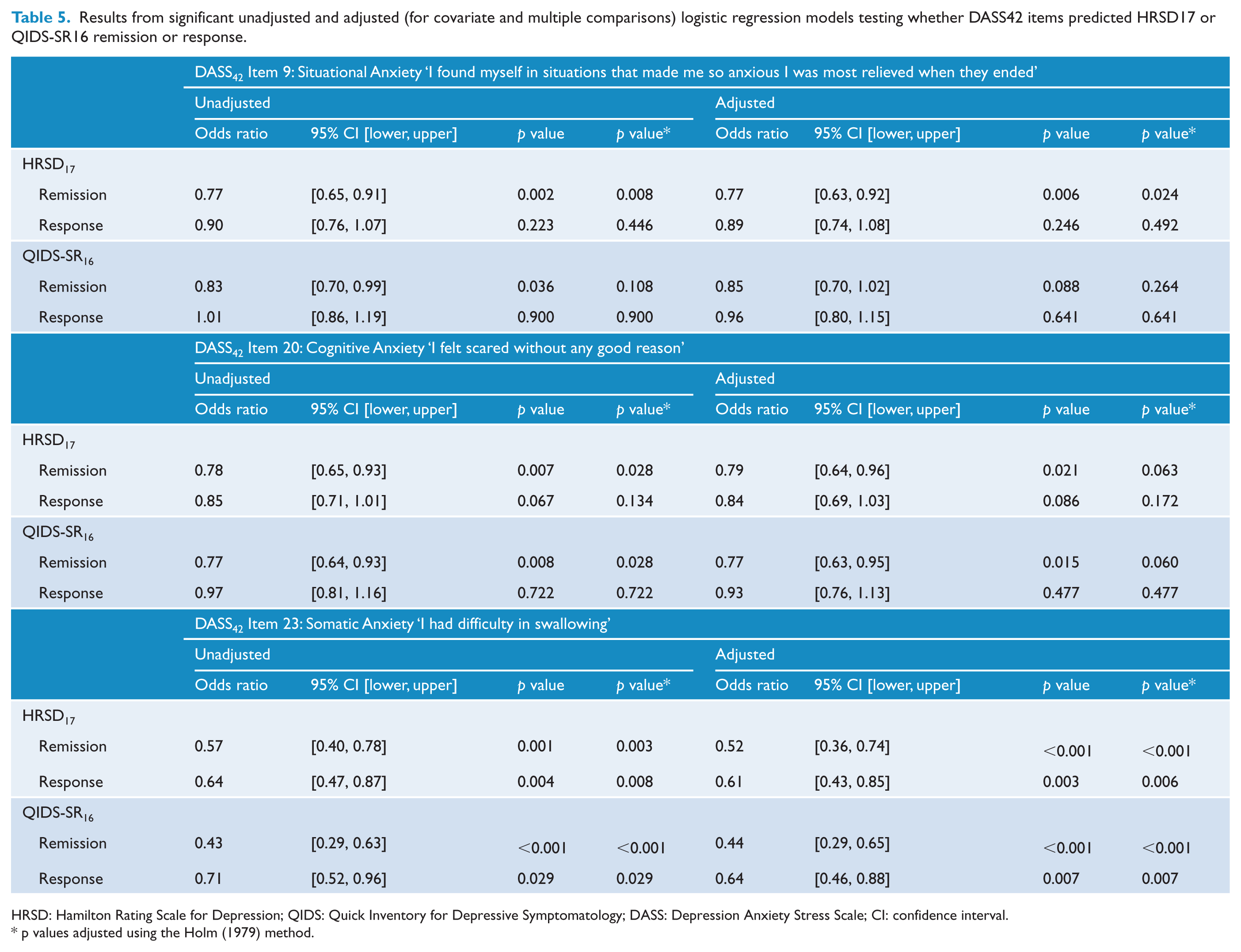
Anxiety subscales did not interact with antidepressant treatment type in predicting treatment outcome (see Supplementary Table 5), so treatments were pooled together. Table 4 provides the results from unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether anxiety-related scales predicted HRSD17 or QIDS-SR16 remission or response. Higher HRSD17 anxiety/somatisation predicted poorer HRSD17 remission before (p = 0.004), but not after covariate adjustment (p = 0.111). Higher DASS42 anxiety predicted poorer QIDS-SR16 remission (p = 0.008) and response (p = 0.009), even after adjusting for covariates (p = 0.017 and p = 0.018, respectively), and multiple comparisons (p = 0.048 and p = 0.050, respectively). To further investigate which items were contributing to predicting treatment outcome, post hoc logistic regressions were run on the individual DASS42 anxiety subscale items. Table 5 provides the results from unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether DASS42 anxiety subscale items predicted HRSD17 or QIDS-SR16 remission or response. Three items predicted both HRSD17 and QIDS-SR16 remission, including DASS42 items 9 ‘I found myself in situations that made me so anxious I was most relieved when they ended’ (hereafter referred to as ‘situational anxiety’), 20 ‘I felt scared without any good reason’ (hereafter referred to as ‘cognitive anxiety’) and 23 ‘I had difficulty in swallowing’ (hereafter referred to as ‘somatic anxiety’). After adjusting for covariates and multiple comparisons, higher situational anxiety predicted poorer HRSD17 remission (p = 0.024) and higher somatic anxiety predicted poorer HRSD17 and QIDS-SR16 remission (both p < 0.001) and response (p = 0.006 and p = 0.007, respectively). Cognitive anxiety no longer predicted treatment outcome after adjusting for covariates and multiple comparisons.
Results from unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether anxiety-related scales predicted HRSD17 or QIDS-SR16 remission or response.
HRSD: Hamilton Rating Scale for Depression; QIDS: Quick Inventory for Depressive Symptomatology; DASS: Depression Anxiety Stress Scale; CI: confidence interval.
p values adjusted using the Benjamini and Hochberg (1995) procedure.
Results from significant unadjusted and adjusted (for covariate and multiple comparisons) logistic regression models testing whether DASS42 items predicted HRSD17 or QIDS-SR16 remission or response.
HRSD: Hamilton Rating Scale for Depression; QIDS: Quick Inventory for Depressive Symptomatology; DASS: Depression Anxiety Stress Scale; CI: confidence interval.
p values adjusted using the Holm (1979) method.
Discussion
We found that common definitions of anxious depression showed poor overlap, were associated with few impairments on clinical outcomes and were not associated with poorer antidepressant treatment outcome. However, higher DASS42 anxiety and specifically items related to situational and somatic anxiety predicted poor treatment outcome, even after adjusting for covariates and multiple comparisons.
The syndromal and HRSD definitions of anxious depression were characterised by few impairments on clinical outcomes. While some characteristics associated with syndromal anxious depression were consistent with previous findings, such as poorer social and occupational functioning (Das-Munshi et al., 2008) and higher neuroticism (Van Der Veen et al., 2015), others such as earlier age of onset (Penninx et al., 2011), poorer health (Das-Munshi et al., 2008), lower quality of life (Zhou et al., 2017), increased risk of suicide (Dold et al., 2017) and suicide attempts (Das-Munshi et al., 2008) were not. Surprisingly, many characteristics previously associated with HRSD anxious depression were not in the current study, including longer current depressive episodes (Seo et al., 2011), more concurrent anxiety disorders (Fava et al., 2004; Malhi et al., 2002), poorer social and occupational functioning (Lin et al., 2014), lower quality of life (Seo et al., 2011) and increased risk of suicidal ideation and suicide attempts (Fava et al., 2004, 2008); for reviews, see (Gaspersz et al., 2018; Ionescu et al., 2013).
The lack of observed differences between people with anxious and non-anxious depression may be associated with the more restrictive recruitment and eligibility criteria used for iSPOT-D. For example, exclusion criteria for the iSPOT-D study included people with scores >7 on the suicidality section of the MINI–Plus (Williams et al., 2011), while minimal exclusion criteria was used for STAR*D and similar studies (Fava et al., 2004, 2008; Ionescu et al., 2013). The suggestion of a more restrictive, less heterogeneous sample is also reflected in the lower proportions of syndromal (23.8%) and HRSD (41.9%) anxious depression groups compared to the commonly reported ~50% (Fava et al., 2004, 2008; Ionescu et al., 2013). Furthermore, we corrected for multiple comparisons and covariates not accounted for in previous studies, such as age, sex, years of education, recurrent MDD and the use of sleep aids/anxiolytics (Fava et al., 2004, 2008).
Neither definition of anxious depression was associated with poor treatment outcome after correcting for covariates. Outcomes from previous studies using the same treatments have been mixed (for a review, see Ionescu et al., 2014), with some finding anxious depression to predict poorer antidepressant treatment outcome when compared to their non-anxious counterparts (Fava et al., 2008; Wu et al., 2013), while others have not (Arnow et al., 2015; Farabaugh et al., 2010; Russell et al., 2001). However, most studies do not directly compare treatment outcome between people with anxious and non-anxious depression, and those that do have limited sample sizes (Ionescu et al., 2014). Furthermore, we found syndromal anxious depression predicted better treatment outcome after adjusting for covariates and multiple comparisons. This may reflect the fact that antidepressants are also the first-line pharmacological treatment for most anxiety disorders (Craske and Stein, 2016; Malhi and Mann, 2018), resulting in MDD and anxiety disorders being simultaneously treated. Nonetheless, the current study suggests that, when sufficiently powered and controlled for, common definitions of anxious depression do not predict poorer treatment outcomes.
Comparatively, higher DASS42 anxiety and specifically higher situational and somatic anxiety item scores predicted poorer treatment outcome after adjusting for covariates and multiple comparisons. The DASS42 is a commonly used self-reported community measure and our results suggests it better predicts antidepressant treatment outcome than either syndromal or HRSD17 criteria. Furthermore, characterising anxiety using dimensional criteria is in line with recent efforts to understand mental disorders within transdiagnostic frameworks (Insel et al., 2010; Malhi et al., 2018; Malhi and Porter, 2016). Finally, identifying the specific underlying symptoms that contribute to predicting treatment outcome can better inform targeted therapies (Malhi et al., 2019).
This study has several limitations. iSPOT-D was designed as a practical study and recruited participants who were actively seeking antidepressant treatment to reflect real-world practice (Williams et al., 2011). While this increases the generalisability of our results, other studies using more severe populations may find prevalence rates and clinical characteristics more closely aligned to those reported in previous studies (Fava et al., 2004, 2006, 2008). Treatments were assessed together due to tests showing no significant interactions between anxious depression definitions and treatments. However, some tests approached significance and future research may wish to consider exploring treatments separately. Furthermore, our findings are limited to the three antidepressants used in the study, with other classes of antidepressants and psychological treatments requiring further investigation. Finally, participants were diagnosed with DSM-IV criteria, and we could not approximate the DSM-V anxious distress specifier symptom criteria with our data (Gaspersz et al., 2017). Therefore, the DSM-V anxious distress specifier definition was not assessed.
In conclusion, our results suggest common definitions of anxious depression show poor agreement and do not predict poorer treatment outcome. Furthermore, anxiety symptoms and their use in predicting treatment outcome may be better conceptualised dimensionally using the DASS42. Future research should explore how DASS42 anxiety and its items predictive of treatment outcome interact with biological markers to better characterise disease states and produce more effective targeted therapies.
Supplemental Material
Supplementary_Material_6MAR19 – Supplemental material for Characterising anxiety in major depressive disorder and its use in predicting antidepressant treatment outcome: An iSPOT-D report
Supplemental material, Supplementary_Material_6MAR19 for Characterising anxiety in major depressive disorder and its use in predicting antidepressant treatment outcome: An iSPOT-D report by Taylor A Braund, Donna M Palmer, Leanne M Williams and Anthony WF Harris in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We acknowledge Evian Gordon, PhD MD, as sponsor principal investigator; Claire Day, PhD, as the global trial manager (2008-2014); Anna Campain, PhD, for her help on earlier revisions of the manuscript; and contributions of the principal investigators and research teams at each study site.
Declaration of Conflicting Interests
T.A.B. and D.M.P. report salaries from The Brain Resource Company outside the submitted work. L.M.W. reports personal fees from BlackThorn Therapeutics, Humana, and Psyberguide, outside the submitted work. A.W.F.H. reports personal fees from Janssen Australia, Lundbeck Australia, Servier, and Sumitomo Dainoppon Pharma outside the submitted work.
Funding
T.A.B. was supported by a NSW Health PhD scholarship. iSPOT-D was sponsored by Brain Resource Company Operations Pty Ltd. Brain Resource personnel coordinated the research sites and data quality control, but did not participate in the collection of any data.
Trial registration
The clinical trial is registered with ClinicalTrials.gov (registration number: NCT00693849).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.