
Abstract
In recent years there has been growing concern about the use of illicit drugs in young New Zealanders. This concern has been reflected in a number of government and local initiatives aimed at reducing the use of illicit drugs and minimizing the harm caused by illicit drug use [1, 2]. These plans acknowledge the extent to which the use and misuse of illicit drugs represents a critical social issue with implications for the health and safety of a large number of New Zealanders.
The importance of the issue of illicit drug use is illustrated by periodic cross-sectional surveys of illicit drug use in New Zealand. These surveys have provided evidence that illicit drug use is common among New Zealanders, is particularly common in young people, and may be increasing. For example, Wilkins et al. [3] reported that approximately 52% of respondents aged 15–45 had reported using cannabis on at least one occasion in their lives. For illicit drugs other than cannabis, 4% of respondents reported having used opiates, 15% reported using hallucinogens and 11.9% reported using stimulants (including cocaine, amphetamine/methamphetamine and derivatives of these) at least once in their lives [3]. Furthermore, Wilkins et al. [3] reported that patterns of use appeared to be age dependent with the highest incidence of use in the previous year being reported by those in the 18–24 years age range. In this group, approximately 35% of the sample had reported using cannabis on at least one occasion in the previous year, and 21% reported having used other illicit drugs on at least one occasion in the previous year [3]. Comparisons between 1998 and 2001 surveys suggested that there was an increase in the rates of other illicit drug use, particularly for hallucinogens and stimulants [3]. The percentage of the sample reporting having used hallucinogens on at least one occasion increased from 12.8% to 15%, while the percentage of those reporting having used stimulants increased from 9% to 11.9% [3].
It should also be noted that a number of studies examining the prevalence and incidence of illicit drug use in New Zealand and overseas have been cross-sectional studies. Although these have provided valuable data on illicit drug use, it would be of particular importance to examine prospective, longitudinal data on illicit drug use. Longitudinal data provide more accurate estimates of cumulative use over the life span than retrospective reports of past use [4], as well as more accurate estimates of such factors as age of onset and the timings of the occurrence of other risk factors [5].
In light of these concerns and methodological issues, there is a need for further detailed information on patterns of illicit drug use among adolescents and young adults. To address this, the present paper reports on the results of analyses of cumulative measures of illicit drug use and dependence in a birth cohort of young New Zealanders studied to the age of 25. The specific aims of this investigation were:
To derive life table estimates of the probability that, by a given age, a young person: (i) would have used an illicit drug; and (ii) will report dependence upon an illicit drug. To describe the range of illicit drugs used by young people, and derive life table estimates of the probability that by age 25 a young person would have used or become dependent upon a particular kind of drug. To determine the demographic distribution of illicit drug use and dependence by gender, ethnicity and education level. To explore the extent to which family and social factors may contribute to an increased the risk of illicit drug use and dependence.
Method
Data were collected as part of the Christchurch Health and Development Study (CHDS), which is a longitudinal study of a birth cohort of 1265 children born in the Christchurch, New Zealand urban region during mid-1977. This cohort has been studied at birth, 4 months, 1 year, at annual intervals up to age 16, and at ages 18, 21 and 25 years.
Measures
Cannabis and other illicit drug use
At each assessment (15, 16, 18, 21 and 25 years), sample members were questioned about their use of cannabis and other illicit drugs, including the age at which they first reported using these drugs, and the different types of other illicit drugs they had used in each year from age 14–15 to age 24–25 years. The cohort members were questioned about their use of a range of illicit drugs, including cannabis, solvents (glue, petrol, paint); amphetamine-type stimulants (including methamphetamine and amphetamines); barbiturates; prescription medications that were illicitly obtained; opiates, including both heroin and morphine; cocaine (in any form); hallucinogens including ecstasy, LSD and PCP; and any other substances, primarily plant extracts, including psilocybin mushrooms and datura. The questions regarding the use of individual classes of drugs were non-specific to allow comparison across assessment periods. Reports of cannabis and other illicit drug use were used to derive life table estimates of the cumulative risk of cannabis and other illicit drug use (and overall illicit drug use) over the period 14–25 years.
Cannabis and other illicit drug dependence
In addition, respondents were questioned about symptoms of cannabis and other illicit drug dependence using questions based on the generic DSM-IV [6] criteria for substance dependence derived from the Composite International Diagnostic Interview (CIDI) [7]. This questioning was not started until age 16 years; thus the earliest estimates of cannabis and other illicit drug dependence are reported from age 18 years.
Demographic factors
At age 21 years, an assessment of the ethnic identification of Māori members of the cohort was conducted using the 1996 New Zealand census questions on ethnicity as well as a questionnaire designed by the Ngai Tahu Māori Health Research unit. Fifteen per cent of the cohort reported Māori descent, while 11% reported Māori cultural identification. In this paper those reporting a Māori cultural identification were classified as Māori.
At age 18, cohort members were assessed as to the extent of their educational qualifications. Those who reported having left secondary school without achieving qualifications were classified as having left without qualifications (19% of the sample). Gender was recorded at birth.
Risk factors
To examine predictors of illicit drug use, measures of social, family and childhood circumstances were considered. These included family social background, family functioning, individual characteristics, adolescent behaviours and peer affiliations. Initial analyses revealed that the following measures were significant predictors of illicit drug use or dependence:
Peer substance use – Assessed on the basis of participant reports of the extent to which their friends used tobacco, alcohol, or illicit drugs or had problems resulting from alcohol or illicit drugs, α =0.69–0.77.
Parental history of illicit drug use – Parental illicit drug use was assessed at age 11 (24.9% of the sample were thus classified) via parent self-report and scored as a dichotomous measure.
Novelty-seeking (age 16) – Assessed at age 16 using the noveltyseeking items from the Tridimensional Personality Questionnaire [8], α =0.76.
Frequency of cigarette smoking (age 14) – Assessed at age 14 on a five-point scale ranging from non-smoker to daily smoker via young person self-report.
Frequency of alcohol use (age 14) – Assessed at age 14 via selfreported number of occasions of alcohol use over the previous 3months via young person self-report.
Childhood sexual abuse – Assessed via young person self-report at ages 18 and 21 for the period up to and including 15 years, spanning an array of abusive experiences, resulting in a four-level classification of severity [9].
Conduct problems (age 14) – Assessed via parent and child reports of child behaviour issues at age 14 using items from the Rutter et al. [10] and Conners [11, 12] behaviour scales, and from the Diagnostic Interview Schedule for Children [13], α =0.90.
Statistical analyses
All analyses were based on all cohortmembers assessed at each point of observation. Sample sizes were as follows: 15 years (965); 16 years (953); 18 years (1025); 21 years (1011); and 25 years (1003). These samples represented between 75% and 81% of the original cohort of 1265 participants and over 85% of study participants resident in New Zealand at each age.
Rates of cannabis and other illicit drug use by cohort members were used to calculate life table estimates of cannabis, other illicit drug, and any illicit drug (either cannabis or other illicit drug) use and dependence, in order to estimate the cumulative risk of using or being dependent upon cannabis and other illicit drugs by ages 15, 18, 21 and 25. These life table estimates were then tested for demographic differences in illicit drug use and dependence (gender, Māori and education level) using a univariate log-rank test. Finally, proportional hazards regression models were fitted to the data to identify childhood and family factors that were predictive of the onset of illicit drug use or dependence.
Results
The development of illicit drug use
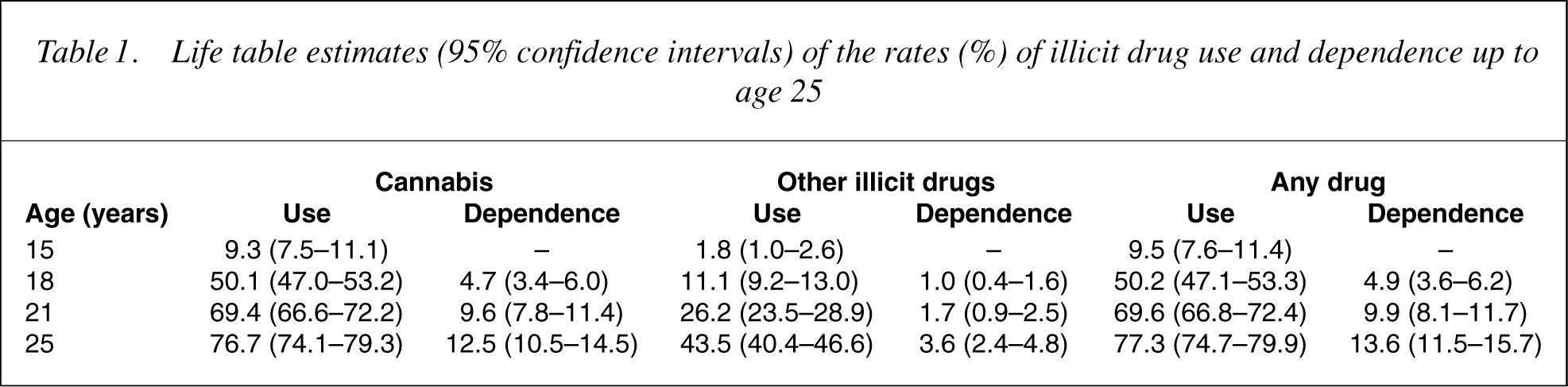
Table 1 presents life table estimates of risks of cannabis and other illicit drug use and dependence over the period from 15 to 25. The table shows a high level of use of both cannabis and other illicit drugs. By the age of 25, almost 77% of the cohort had used cannabis and 43.5% had used other illicit drugs. Overall rates of dependence were relatively high with nearly one in seven (13.6%) meeting diagnostic criteria for substance use dependence; 12.5% met criteria for cannabis and 3.6% met criteria for other drug dependence. The table also shows that there was a rapid growth in illicit drug use and dependence over the period from 15 to 18.
Life table estimates (95% confidence intervals) of the rates (%) of illicit drug use and dependence up to age 25
Types of illicit drugs used
Table 2 shows the types of other illicit drugs used by the cohort and the percentage of cases in which each type of drug was used in cases of dependence by age 25. Other illicit drug use in the cohort was dominated by hallucinogens, including LSD and ecstasy (36.2%) and amphetamine-type stimulants (26.9%). However, a substantial minority had used harder drugs including cocaine (9.1%) and opiates (3.7%). There was also a high rate of use of other substances, primarily plant extracts including psilocybin mushrooms and datura.
Estimated cumulative risk (%) of various other illicit drug use and dependence by age 25
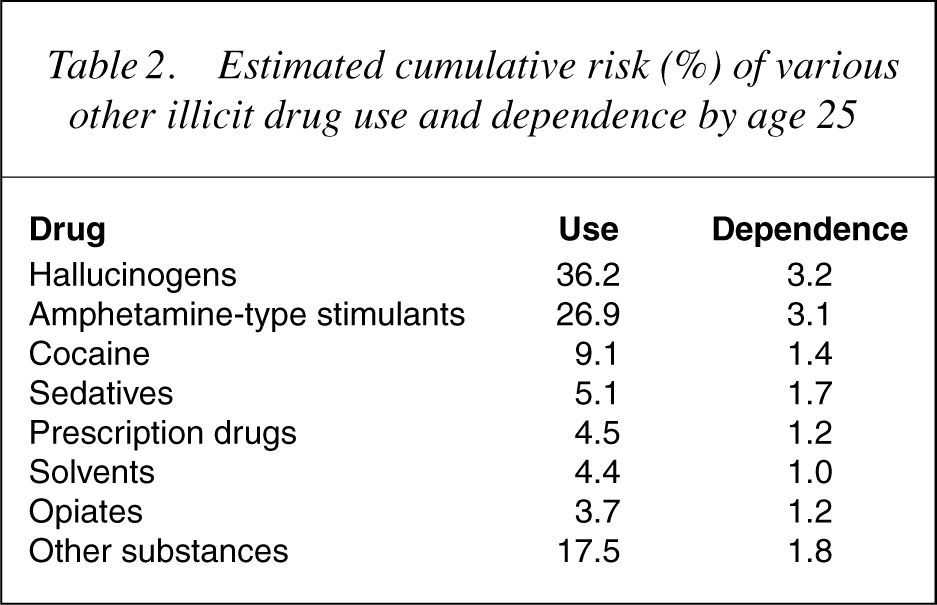
It will be noted that the percentages of other illicit drugs used exceeds the percentage (43.5%) of those using any other illicit drugs. This reflects the fact that those using other illicit drugs tended to use more than one other illicit drug. Those using other illicit drugs reported a mean of 2.4 other illicit drugs used by age 25.
Differences in illicit drug use by gender, ethnicity and education
Table 3 shows life table estimates of the rates for use and dependence on cannabis and other illicit drugs by age 25, classified by: (i) gender; (ii) ethnicity; and (iii) education level. The table shows that:
Males were significantly more likely than females to report: (i) cannabis dependence (p<0.0001); (ii) using other illicit drugs (p<0.05); (iii) using any illicit drugs (p<0.05); and (iv) dependence on any illicit drugs (p<0.0001). Cohort members identifying themselves as Māori were significantly more likely than non-Māori to report: (i) using cannabis (p<0.0001); (ii) cannabis dependence (p<0.05); (iii) using any illicit drugs (p<0.0001); and (iv) dependence on any illicit drugs (p<0.05). Those cohort members who left school without qualifications were significantly more likely than those achieving qualifications to report: (i) using cannabis (p<0.0001); (ii) cannabis dependence (p<0.0001); (iii) dependence on other illicit drugs (p<0.01); (iv) using any illicit drugs (p<0.0001); and (v) dependence on any illicit drugs (p<0.0001).
Estimated cumulative risk (%) of cannabis and other illicit drug use and dependence by age 25 for gender; ethnicity; and education
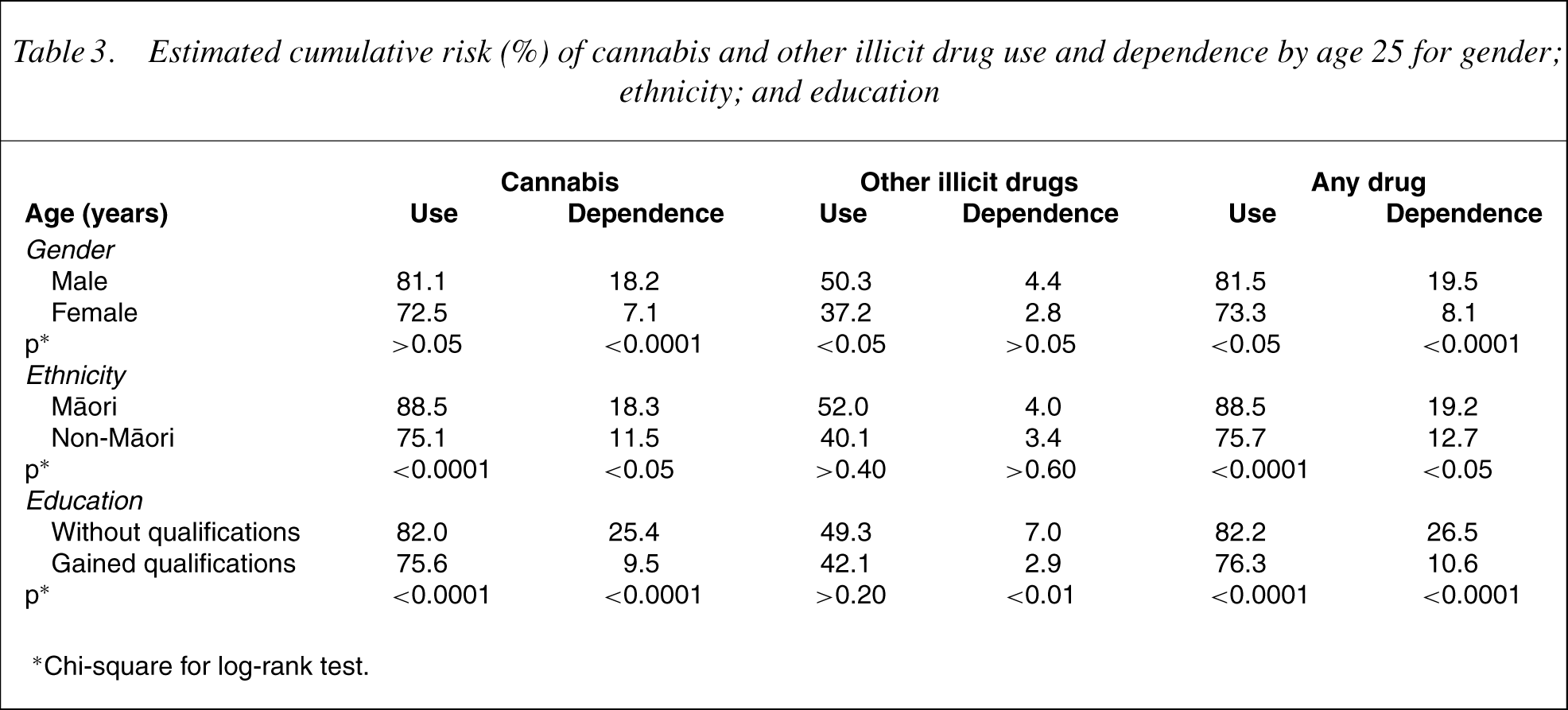
∗Chi-square for log-rank test.
Risk factors for illicit drug use and dependence
The results above raise issues about the extent to which patterns of illicit drug use and dependence could have been predicted from factors present by age 15 years. This issue was explored by fitting proportional hazards regression models in which the hazards or instantaneous risks of onset of cannabis and other illicit drug use and dependence by age 25 years were modelled as log-linear functions of a range of social, childhood and related risk factors. The results of these regression models are presented in Table 4, which shows parameter estimates, standard errors, and significance levels for the statistically significant demographic factors and risk factors for any illicit drug use and dependence. The table shows that:
Illicit drug use was predicted by: (i) male gender (p<0.0001); (ii) Māori identification (p<0.05); (iii) association with substanceusing peers (p<0.0001); (iv) a parental history of illicit substance use (p<0.001); (v) novelty-seeking (p<0.0001); (vi) frequency of cigarette smoking at age 14 (p<0.0001); and (vii) frequency of alcohol consumption at age 14 (p<0.0001). Illicit drug dependence was predicted by: (i) gender (p<0.0001); (ii) association with substance-using peers (p<0.0001); (iii) a parental history of illicit substance use (p<0.05); (iv) childhood sexual abuse (p<0.0001); (v) novelty-seeking (p<0.0001); and (vi) conduct problems at age 14 (p<0.05).
Parameter estimates, standard errors and significance levels for proportional hazard models of any illicit drug use and dependence by age 25
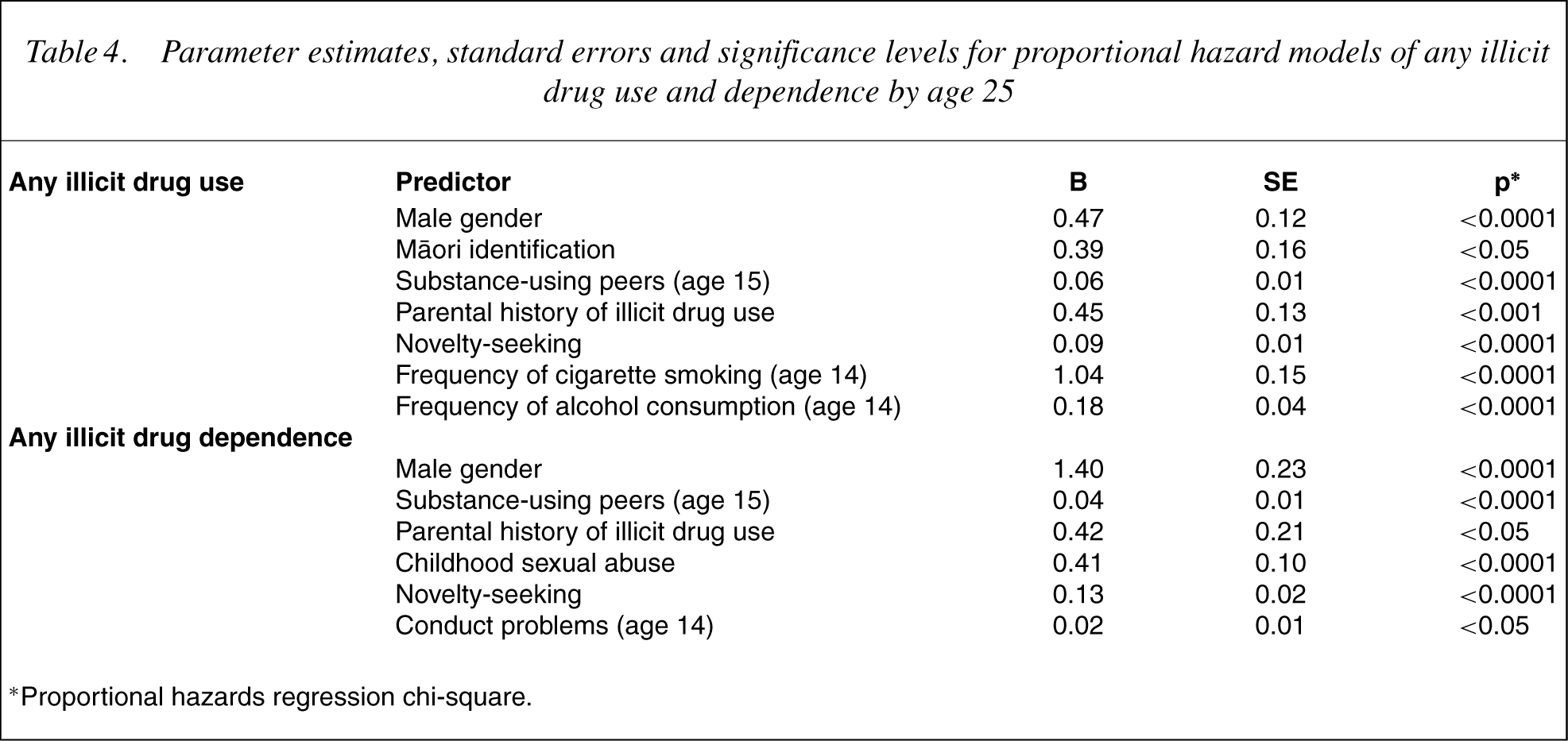
∗Proportional hazards regression chi-square.
The results suggest that the association between education, ethnicity, and illicit drug use and dependence reported in Table 3 were partially mediated by the other risk factors shown in Table 4. In particular, after adjustment for these factors, education level was no longer a predictor of illicit drug use while ethnicity remained predictive of illicit drug use. In contrast, both education level and ethnicity were no longer predictive of illicit drug dependence after risk factors had been taken into account. However, gender remained a predictor of illicit drug use and dependence in the proportional hazards regression model, even after control for risk factors, suggesting that males were more susceptible to use and misuse of illicit drugs.
Similar proportional hazards regression analyses were carried out for cannabis use and dependence, and other illicit drug use and dependence. A similar pattern of findings emerged for cannabis and other illicit drug use and dependence as were reported in Table 4.
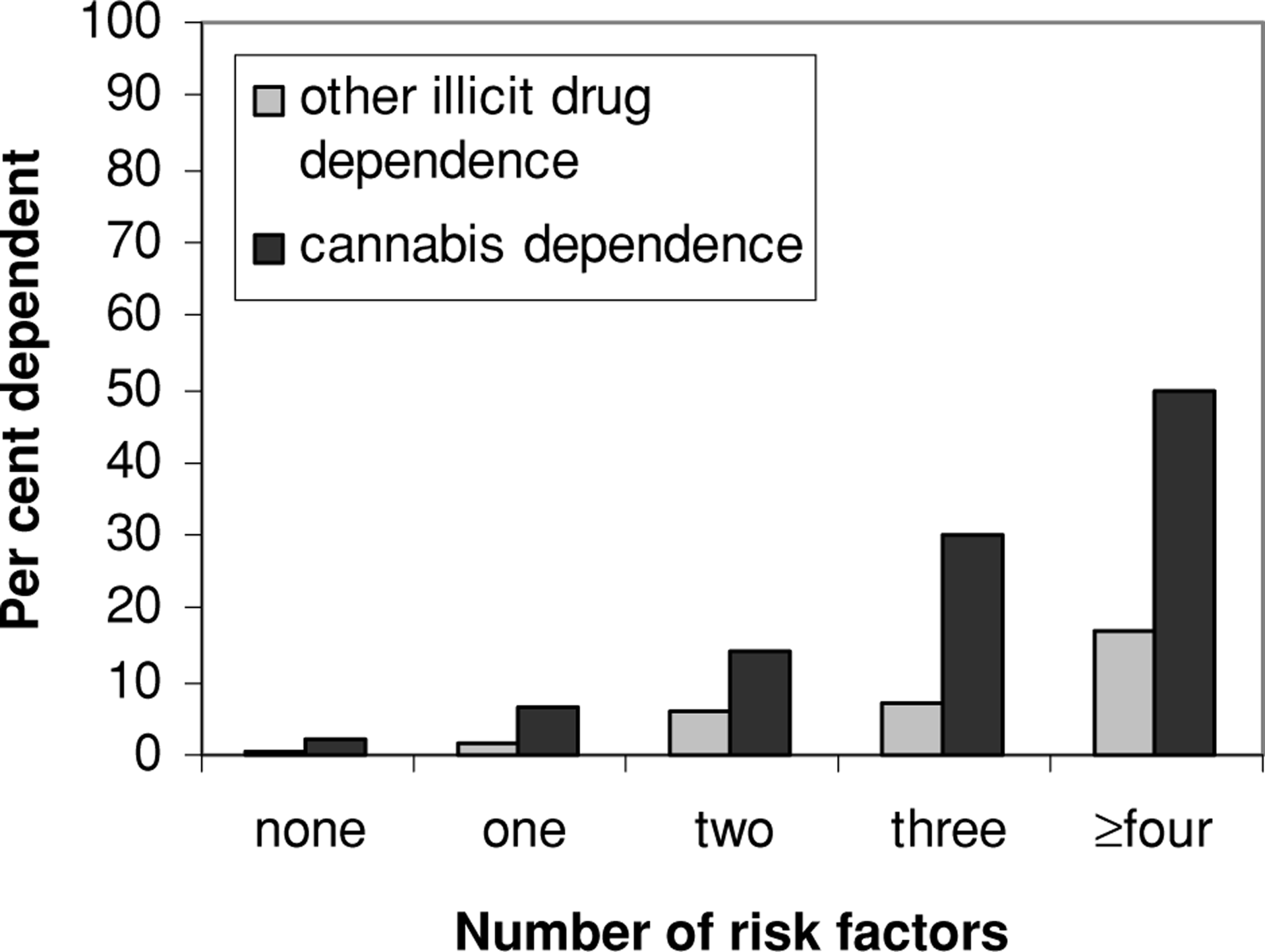
The results of the fitted regression models for illicit drug use and dependence are illustrated in Figs 1 and 2, which depict rates of cannabis and other illicit drug use (Fig. 1) and dependence (Fig. 2) classified by the number of risk factors present in cohort members. Risk factors were dichotomized as: (i) present or absent, in the case of (male) gender, Māori identification, parental history of illicit substance use, and sexual abuse; or (ii) the cohort member scoring in the highest decile on the risk factor measure, in the case of peer substance use, novelty-seeking, frequency of cigarette smoking and alcohol use, and conduct disorder at age 14. The dichotomized risk factor scores were summed to give a total number of risk factors present for each cohort member. The results for illicit drug use show clear trends in which increased exposure to risks is associated with increased use of both cannabis and other illicit drugs. Those with three or more risk factors (38% of the cohort) had over a 95% chance of using cannabis and a better than 60% chance of using other illicit drugs. The results for illicit drug dependence show a similar pattern of increased exposure to risks being associated with increased dependence. Those with four or more risk factors (11% of the cohort) had a 50% risk of cannabis dependence and a greater than 15% risk of dependence on other illicit drugs.
Relationship between rates of illicit drug use (%) and number of risk factors. Relationship between rates of illicit drug dependence (%) and number of risk factors.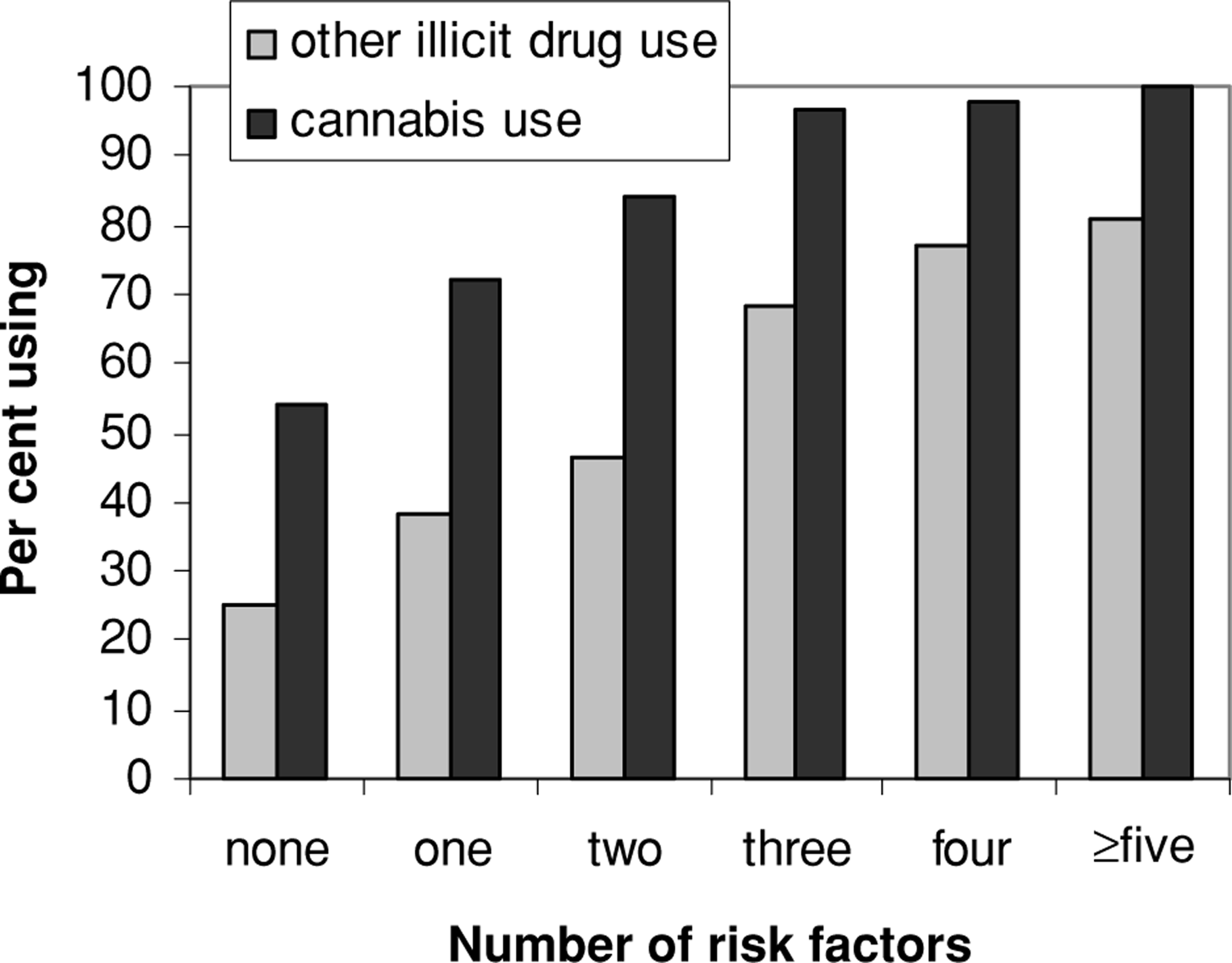
Discussion
This paper has presented a longitudinal description of patterns of illicit drug use by members of the CHDS cohort up to the age of 25 years, and an examination of the risk factors for illicit drug use and dependence among cohort members. A number of major themes and issues emerged from the analyses.
The principal findings of this study were of high lifetime rates of illicit drug use, with nearly 80% of the cohort using an illicit drug by the age of 25. This high lifetime rate of illicit drug use is consistent with that found in other New Zealand studies. Thus, the Dunedin Multidisciplinary Health and Development Study [14, 15] found that by age 26, 70.1% of cohort members had used cannabis at some point in their lives (compared with 76.7% in the current study). Similarly, the 2001 National Drug Use surveys [3] found that nearly 60% of New Zealanders aged 18–24 reported using cannabis on at least one occasion. Because the National Drug Use survey is based on retrospective reports derived from cross-sectional data, it may underestimate the lifetime use of illicit drugs by young adults. In comparison with observed international rates of illicit drug use, drug use by young New Zealanders appears to be relatively high. For example, US and European studies suggest rates of illicit drug use in young people that range from 44% to 55% [16–19]. The high rate of illicit drug use in New Zealand is largely explained by the high rate of cannabis use.
As might be expected from high lifetime rates of illicit drug use, life time rates of illicit drug dependence in this cohort were comparatively high, with 12.5% meeting DSM-IV criteria for cannabis dependence and 3.6% meeting criteria for other illicit drug dependence by age 25. These figures are similar to those reported by the Dunedin Multidisciplinary Health and Development Study, who found that 9.4% of the sample had met DSM-III and DSM-IV criteria for cannabis dependence by age 26 [15]. There has been growing international interest in rates of illicit drug dependence, and in particular cannabis dependence. Comparisons suggest that Australia and New Zealand tend to have higher rates of illicit drug dependence, ranging from 12% to 9% [15],20– [22], than the US and Europe, with rates ranging from 3.4% to 2.2% [19, 23, 24]. Although the precise reasons for these differences are unknown, it is possible that certain cultural or social factors unique to Australasia lead to higher rates of illicit drug dependence in this area. In the present cohort, high levels of substance use may be one reason for the observed high levels of dependence, as suggested by Degenhardt et al. [25].
The results also show that the CHDS cohort members had experience with awide array of drugs. The most commonly used drugs, aside from cannabis, were hallucinogens (36.2%) and amphetamine-type stimulants (26.9%), with a minority of the cohort using ‘hard’ drugs such as cocaine (9.1%) and opiates (3.7%). In addition, there was clear evidence of poly-drug use among those using other illicit drugs. In this group the average number of different types of illicit drugs (other than cannabis) used by age 25 was 2.4.
Overall these results reinforce concerns about the apparently growing utilization of illicit drugs by adolescents and young people. The findings of this study suggest:
The use of illicit drugs by young people has reached a point where drug use at some point in the life span is part of normal experience. Although the majority of illicit drug users are occasional recreational users who do not develop dependence, nearly one in seven young people develop dependence on an illicit drug by age 25. In most cases this dependence involved cannabis.
In agreement with a number of other studies, illicit drug use and dependence was more common among males, Māori and young people lacking formal educational qualifications [15, 22,26–28].
Subsequent analyses of this cohort suggested that while gender remained a predictor of illicit drug use and dependence, the associations between ethnicity and education level and illicit drug use and dependence reflected the influence of a series of mediating factors. These factors included family and childhood factors, peer factors, and personality factors. Specifically, those factors that were found to predict illicit substance use and dependence included having parents who used illicit drugs, experiencing sexual abuse as a child, affiliating with substanceusing peers during early adolescence, cigarette smoking and alcohol consumption by age 14, novelty-seeking behaviours and conduct problems at age 14. Examination of the role of these factors in the development of illicit drug use and dependence suggests a cumulative risk model in which risks of use and dependence increased with increasing exposure to risk factors in childhood and adolescence.
Although the present study provides an overview of illicit drug use and dependence and the correlates of such use and dependence, the findings are subject to a number of caveats.
Measurement – First, all measurements were based on self-report data, and the accuracy of the reports depends upon the willingness of respondents to disclose illicit drug use and dependence. It is possible that this limitation may have led to some underreporting of illicit drug use and dependence, so the results of this study should best be interpreted as giving lower limit estimates of the actual incidence of illicit drug use and dependence among the CHDS cohort.
Sampling – This paper is based on the results for a cohort born at a specific point in time and in a specific geographic region, and measured at specific ages. The extent to which these findings can be generalized to other cohorts in other regions of New Zealand or elsewhere is unclear. In particular, there has been concern on the part of many about the increasing use of illicit drugs by adolescents, and it may be that findings from this study have underestimated the problem of the use of illicit drugs in the contemporary adolescent population.
These concerns notwithstanding, the present study suggests a disturbingly high level of use of, and dependence on, illicit drugs by young people in New Zealand, with particularly high rates of cannabis use. The findings should serve to alert psychiatrists and others dealing with this population that issues regarding illicit drug use are perhaps more pervasive than previously believed, and that more attention should perhaps be given to the role of cannabis in the development of drug problems. Recent advances in brief interventions for cannabis and other substance dependence [29–31] would suggest that, although the problems of drug use and dependence may be underestimated, they may indeed be tractable.
Footnotes
Acknowledgements
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.