
Abstract

Despite significant research on cannabis use, less is known about antecedents and effects of less prevalent patterns of use, such as early daily or dependent use. Cohort studies typically have insufficient samples (i.e. small cell sizes) and lack the statistical power to examine relationships between regular use and low prevalence adverse outcomes (e.g. suicide). Consequently, individual cohort studies offer limited opportunity to explore the causes and consequences of cannabis use patterns which confer the greatest burden of disease, namely, daily use and dependence (Curran and Hussong, 2009; Hofer and Piccinin, 2009).
One approach to addressing these limitations is to invest in new, large, prospective studies, capable of providing the power needed to examine less frequent events. However, such studies take decades to mature, are extremely costly and necessarily delay important health knowledge reaching the research field, clinicians, decision makers in government and the general population.
One alternative is to make use of the available data by harmonising and pooling individual participant data across individual cohorts. A multi-cohort consortium approach provides a number of potential advantages including: (1) efficiency in the use of existing data, time and resources; (2) the capacity to bring together expert knowledge from across a range of disciplinary boundaries; (3) increased opportunity for knowledge translation and dissemination; (4) the increased generalisability afforded by combining data collected by different researchers on different samples; and (5) the opportunity to combine data from a number of studies to answer questions that cannot be answered in individual cohorts. We provide an example of such an approach.
The Cannabis Cohorts Research Consortium (CCRC): An example of a multi-cohort consortium approach
The bi-national Cannabis Cohorts Research Consortium (CCRC) is an example of a research effort using integrated data analysis across multiple Australasian cohorts. The CCRC is a multi-organisational and multi-disciplinary international collaboration that brings together a number of the most mature longitudinal studies of child and adolescent development across Australia and New Zealand, including: the Australian Temperament Project (30 years/15 waves), the Christchurch Health and Development Study (37 years/23 waves), the Mater Hospital and University of Queensland Study of Pregnancy (33 years/8 waves), the Personality and Total Health Through Life Project (15 years/4 waves), the Victorian Adolescent Health Cohort Study (20 years/10 waves) and the Western Australian Pregnancy Cohort (Raine) Study (25 years/11 waves).
The CCRC was formed in 2006 and is coordinated by the National Drug and Alcohol Research Centre (NDARC) at UNSW Australia. The CCRC stemmed from a recognised need to better understand the link between cannabis use (particularly rarer patterns of high use) and other substance use, mental health problems and psychosocial outcomes. The CCRC has first focused on cannabis use across adolescence and young adulthood, in particular the impact of regular patterns of use (i.e. daily and dependent use). Here, we describe an approach to developing well-powered samples for the study of infrequent exposures and outcomes.
What cohorts are involved in the CCRC?
The Consortium brings together researchers from some of the largest and longest running longitudinal studies of health and wellbeing internationally. Details of the cohorts presently are:
How has the CCRC pooled data across cohorts?
There are two major approaches to data pooling. The first, commonly used method, combines study level results meta-analytically. This approach is relatively straightforward to apply when there is a clear research hypothesis, the exposure and outcome variables are clearly and consistently specified within and across studies, and the measure of effect size can be easily interpreted (Curran and Hussong, 2009). However, because meta-analyses are based on combining estimates at the study level, rather than at the individual participant level, investigation is limited by low sample size and power. That is, often the unit of analysis in meta-analysis is the study, when more power can be derived if the unit of analysis is the study participant.
The second approach to data pooling, pooling of participant-level data, is less commonly used because gaining access to study participant data is more complicated (ethically and practically) than combining available study-level results. It is, however, ideally suited to investigations of low frequency exposures and/or outcomes such as rarer behaviours (e.g. regular drug use) or genetic variants. The approach involves developing common scales of measurement across cohorts (harmonisation) and pooling participant-level harmonised data from multiple cohorts to create a single (large) integrated dataset of participants rather than studies. Data harmonisation and pooling allows models to be fitted directly to participant-level data and, therefore, provides a number of advantages over study-level meta-analysis. The major advantages of data harmonisation are that it (Curran and Hussong, 2009):
provides increased sample size which enables more powerful examination of less frequent exposures and outcomes;
becomes feasible to explicitly model sources of between-study heterogeneity at the level of the observed data;
improves the stability of model estimation and reduces the influence of outliers and study specific characteristics; and
provides greater precision, particularly for tests of interaction and subgroup analyses.
The CCRC has now developed a harmonised data set with over 20 variables, across four cohorts (ATP, CHDS, MUSP, VAHCS) with more than 7000 respondents, with the purpose of further examining questions around frequent or dependent cannabis use that may not be answered by analyses of individual cohorts. Selected PATH data on cannabis and depression have also been harmonised within this data set (Horwood et al., 2012). We intend to harmonise relevant data from all six cohorts in the CCRC subject to continued funding support. Table 1 provides an overview of the key domains of interest for data harmonisation, the availability of these data across the four main cohorts harmonised to date (ATP, CHDS, MUSP, VAHCS), and where data are available, the measures used in each of these cohort studies.
Summary of study measures and data availability among integrated cohort studies.
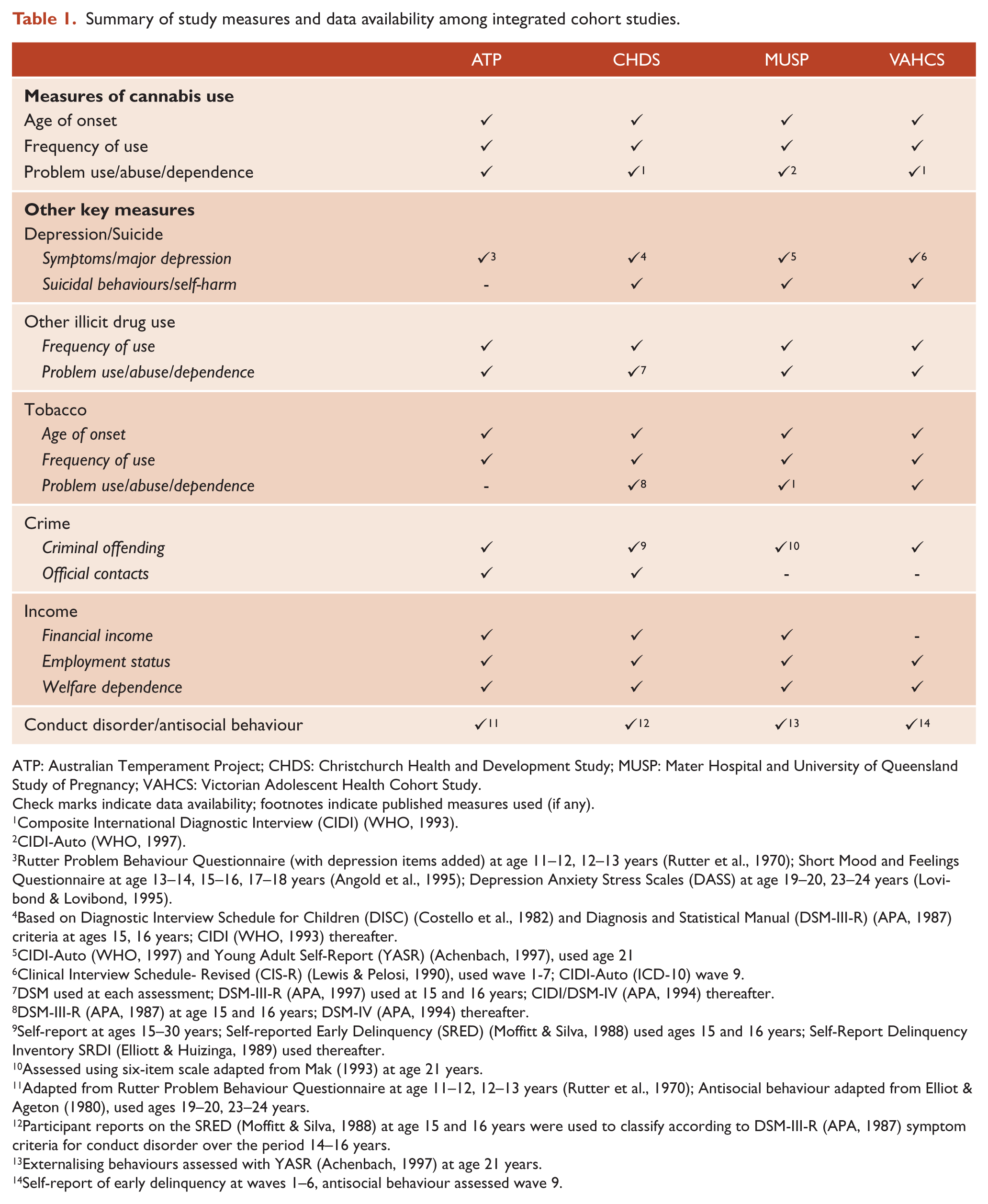
ATP: Australian Temperament Project; CHDS: Christchurch Health and Development Study; MUSP: Mater Hospital and University of Queensland Study of Pregnancy; VAHCS: Victorian Adolescent Health Cohort Study.
Check marks indicate data availability; footnotes indicate published measures used (if any).
Composite International Diagnostic Interview (CIDI) (WHO, 1993).
CIDI-Auto (WHO, 1997).
Rutter Problem Behaviour Questionnaire (with depression items added) at age 11–12, 12–13 years (Rutter et al., 1970); Short Mood and Feelings Questionnaire at age 13–14, 15–16, 17–18 years (Angold et al., 1995); Depression Anxiety Stress Scales (DASS) at age 19–20, 23–24 years (Lovibond & Lovibond, 1995).
Based on Diagnostic Interview Schedule for Children (DISC) (Costello et al., 1982) and Diagnosis and Statistical Manual (DSM-III-R) (APA, 1987) criteria at ages 15, 16 years; CIDI (WHO, 1993) thereafter.
CIDI-Auto (WHO, 1997) and Young Adult Self-Report (YASR) (Achenbach, 1997), used age 21
Clinical Interview Schedule- Revised (CIS-R) (Lewis & Pelosi, 1990), used wave 1-7; CIDI-Auto (ICD-10) wave 9.
DSM used at each assessment; DSM-III-R (APA, 1997) used at 15 and 16 years; CIDI/DSM-IV (APA, 1994) thereafter.
Self-report at ages 15–30 years; Self-reported Early Delinquency (SRED) (Moffitt & Silva, 1988) used ages 15 and 16 years; Self-Report Delinquency Inventory SRDI (Elliott & Huizinga, 1989) used thereafter.
Assessed using six-item scale adapted from Mak (1993) at age 21 years.
Adapted from Rutter Problem Behaviour Questionnaire at age 11–12, 12–13 years (Rutter et al., 1970); Antisocial behaviour adapted from Elliot & Ageton (1980), used ages 19–20, 23–24 years.
Participant reports on the SRED (Moffitt & Silva, 1988) at age 15 and 16 years were used to classify according to DSM-III-R (APA, 1987) symptom criteria for conduct disorder over the period 14–16 years.
Externalising behaviours assessed with YASR (Achenbach, 1997) at age 21 years.
Self-report of early delinquency at waves 1–6, antisocial behaviour assessed wave 9.
The annual attrition rate across the six cohorts was low; in the range of 0.5–3.9% per annum among the cohorts; the retained (contactable) sample rates at most recent follow-up in the range of 70–96% 1 . Although all studies showed evidence of some selection bias attributable to sample attrition, analysis of the implications of such biases for study findings have shown these to be minimal (Silins et al., 2014). Table 2 provides descriptive data on demographic and cannabis use characteristics in the harmonised sample.
Selected demographic and cannabis use characteristics of the CCRC harmonised cohort (n = 7253) in young adulthood. 1
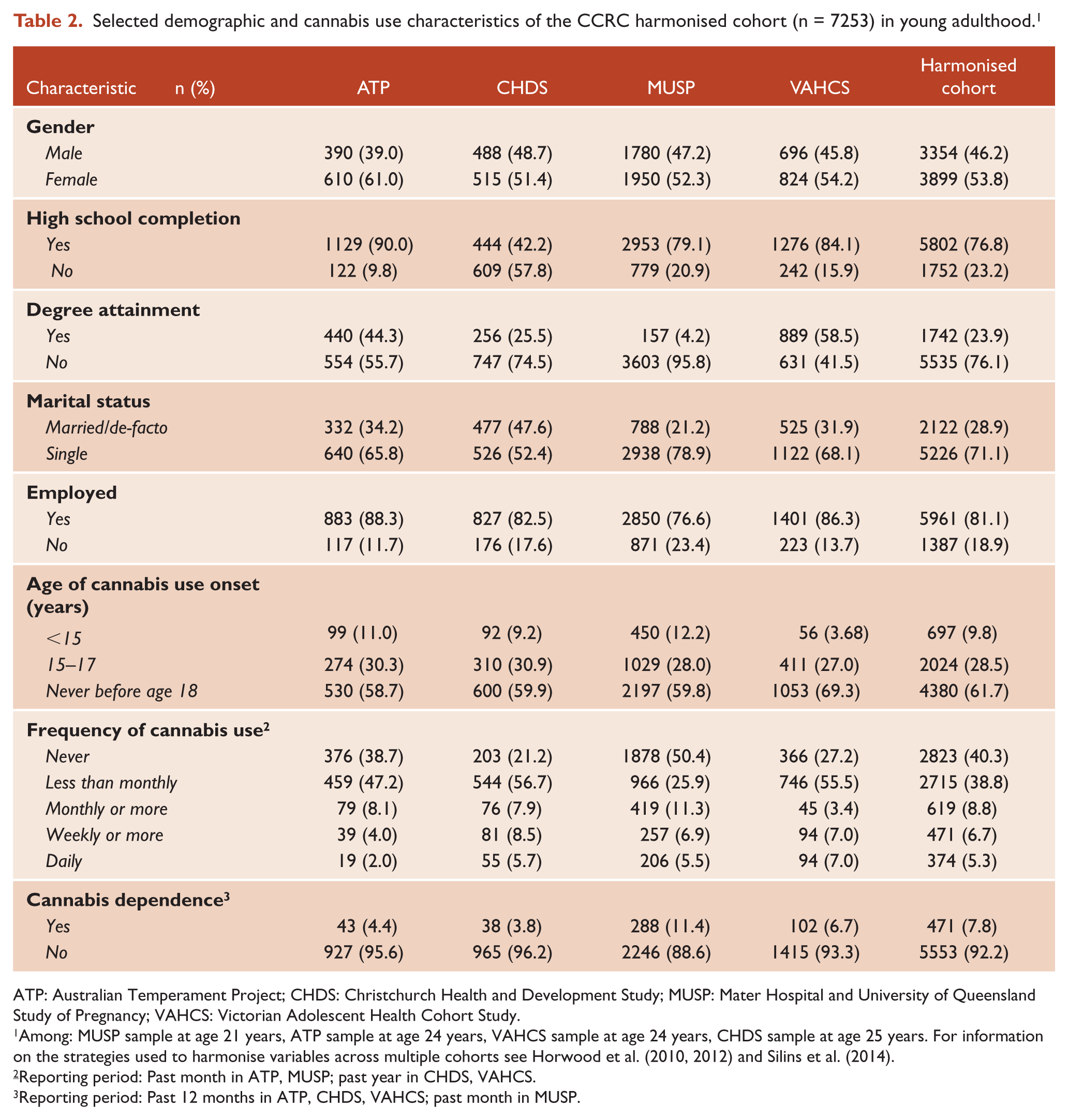
ATP: Australian Temperament Project; CHDS: Christchurch Health and Development Study; MUSP: Mater Hospital and University of Queensland Study of Pregnancy; VAHCS: Victorian Adolescent Health Cohort Study.
Among: MUSP sample at age 21 years, ATP sample at age 24 years, VAHCS sample at age 24 years, CHDS sample at age 25 years. For information on the strategies used to harmonise variables across multiple cohorts see Horwood et al. (2010, 2012) and Silins et al. (2014).
Reporting period: Past month in ATP, MUSP; past year in CHDS, VAHCS.
Reporting period: Past 12 months in ATP, CHDS, VAHCS; past month in MUSP.
What has it found? Key findings and publications
Findings from the analysis of the integrated data improved knowledge of the relationships between cannabis use, mental health, other substance use and social development in young people (Horwood et al., 2010, 2012; Silins et al., 2014). For example, the age of initiation of cannabis use was found to be a significant factor in educational attainment, with early use (i.e. <15 years) accounting for up to 17% of the failure rate (population attributable risk) in obtaining key educational milestones such as high school completion compared with those who had not used by age 18 years (Horwood et al., 2010). In relation to mental health, increasing frequency of cannabis consumption was associated with increased symptoms of depression, with the association strongest among adolescents (Horwood et al., 2012). Evidence has also been found for the adverse sequelae of adolescent cannabis use across a broad range of young adult outcomes, including cannabis and other illicit drug dependence and attempted suicide (Silins et al., 2014). Recently obtained additional NHMRC funding for the existing CCRC data sets will enable extension of this harmonisation work to alcohol, including the antecedents and consequences of less prevalent patterns of youth alcohol use.
What are the advantages and challenges?
Through the Consortium’s experience we have identified a range of advantages and challenges of the integrated data analysis and of the collaborative process by which the data set was formed. Advantages of the CCRC analytic process include: access to high-quality longitudinal studies that provide a rich pool of data across important developmental periods from childhood, through adolescence and into adulthood; increased sample size and statistical power to investigate rarer exposures and outcomes; the potential to compare model parameters to establish which effects are universal versus cohort specific; the efficient use of existing resources; the development of infrastructure and expertise in Australia and New Zealand in data harmonisation methodologies; the demonstrated feasibility of the approach and the potential applicability of the approach to a range of other mental health and substance use problems.
Advantages to the multi-cohort collaborative approach include: increased capacity to bring together expert knowledge from across a range of disciplines; the establishment of positive collaborative relations between study investigators and across the field; opportunities for mentorship and training of younger researchers by senior academics, including co-authorship; and the opportunity for significant knowledge dissemination and translation, with the potential to have greater impact than any one study alone. For example, media reporting of Silins et al. (2014) included 631 media citations in the month post-publication (including online = 373, radio = 170, television = 78 and print = 10), across 29 countries (e.g. United States, United Kingdom, Australia, New Zealand, Asia, Middle East, South America, Eastern Europe, Western Europe).
Challenges: One of the principal challenges for the CCRC is the cross study heterogeneity in multi-cohort analyses. Common sources of between study heterogeneity include use of different measures, sampling variation, timing of historical events and study design characteristics (Curran and Hussong, 2009). The CCRC cohorts do, however, have a number of advantages that reduce the effect of heterogeneity. Specifically, all cohorts: (1) are population based samples; (2) were born about the same historical time and are culturally similar; (3) adopted broadly similar data collection strategies (i.e. repeated measures interview and questionnaire assessments); and (4) have used broadly consistent measures of the primary outcomes and exposures (Table 1).
Harmonisation of data from these contemporary population studies across Australasia, with due allowance for differences in study design and variability, augments our ability to generalise our findings to the region more realistically than is possible for any individual study (Curran and Hussong, 2009). The prevalence of cannabis use in Australia and New Zealand appears to be reasonably consistent with countries such as the United States, Canada and Western Europe (Copeland and Swift, 2009; Murray et al., 2007) and generalisation of our findings to these high income countries would appear to be justified, allowing for the fact that the extent of possible confounding by variation in legislation between jurisdictions is unknown.
There are also challenges related to developing and maintaining this collaborative work. These include limited funding available in Australia and New Zealand for data harmonisation; the large investment in time, resources and statistical expertise required to harmonise data; limits to the number of cohorts that can be harmonised; the challenges of bringing people together and maintaining momentum, especially as the harmonisation process can be slow; and the need for clear understanding and rules about ownership of ideas, data and work product. There are also ethical constraints around data sharing (e.g. limitations on the extent to which data are directly available to researchers conducting the harmonisation work).
Conclusion
A data harmonisation approach to combining participant level data from large cohort studies provides a unique opportunity to examine salient cannabis-related or other questions that are not possible to address in individual cohorts or using meta-analytic approaches. Although acknowledging challenges to the combined cohort approach, the ongoing CCRC work has demonstrated the capacity of the researchers to collaborate in data harmonisation and that combining participant level data from several similar and large Australasian cohorts is feasible. Results from the CCRC study will allow cross-validation of important cannabis-related research questions in Australasia and internationally. Recent funding through the NHMRC will enable extension of the harmonisation work to alcohol, including the antecedents and consequences of less prevalent patterns of youth alcohol use. The work of the CCRC will produce more comparable and robust findings about the linkages between substance use, mental health and social development in young people. Importantly, it enables critical health related questions to be addressed which may not be adequately answered within individual cohorts.
Can I get hold of the data? Where can I find out more?
Information about the CCRC can be obtained through the National Drug and Alcohol Research Centre at the University of New South Wales (http://ndarc.med.unsw.edu.au/project/cannabis-cohort-research-consortium-ccrc). Specific enquires regarding the CCRC harmonised data set are coordinated with Data Custodians by Dr Delyse Hutchinson (
The Cannabis Cohorts Research Consortium
Includes the listed authors and: Steve Allsop, Carolyn Coffey, Jan Copeland, Wayne Hall, Trish Jacomb, Primrose Letcher, Kerri Little, Ann Sanson, Rachel Skinner, Tim Slade, Diana Smart and Maree Teesson.
Footnotes
Acknowledgements
We would like to acknowledge the following who have contributed to discussions about the CCRC: Dave Allsop, Anton Clifford, Alan Clough, John Howard, Caitlin Hughes, Kylie Lee, Eugene Mattes, Jenny Mountain, Paul Nelson, Meredith O’Connor, Andrew Percy, Marian Shanahan, Jenny Williams and Tim Windsor.
We would like to thank all individuals and families involved in the participating cohorts for their time and invaluable contribution to the study.
The ATP would like to acknowledge all who have contributed to the Australian Temperament Project, especially founding investigators Professor Ann Sanson, Diana Smart, and Professors Margot Prior and Frank Oberklaid. The ATP has received ongoing financial support from many funding agencies and institutions over the years, in particular the National Health and Medical Research Council and the Australian Research Council grant.
The CHDS has been supported by funding from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation, the New Zealand Lottery Grants Board, the University of Otago, the Carney Centre for Pharmacogenomics, the James Hume Bequest Fund, the US National Institutes of Health (MH077874), and the National Institute on Drug Abuse (DA/MH11301).
The MUSP would like to thank the data collection team and Greg Shuttlewood, the data manager of the University of Queensland. The core study was funded by the National Health and Medical Research Council (NHMRC) of Australia but the views expressed in the paper are those of the authors and not necessarily those of any funding body.
We thank Kaarin Anstey, Anthony Jorm, Bryan Rodgers, Simon Easteal, Nicolas Cherbuin, Andrew McKinnon, Trish Jacomb, Karen Maxwell and the PATH interviewing team for their contribution to PATH.
The Raine Study gratefully acknowledges the contribution of the Raine Study Team for cohort management and coordination, and the National Health and Medical Research Council (NHMRC) of Australia for funding contributions to the study over the last 23 years. We acknowledge The University of Western Australia (UWA), Telethon Institute for Child Health Research, Raine Medical Research Foundation at UWA, UWA Faculty of Medicine, Dentistry and Health Sciences, Women’s and Infant’s Research Foundation and Curtin University for core management funding.
We thank Christina O’Loughlin, John Carlin and Helen Romaniuk for their contributions to the Victorian Adolescent Health Cohort.
Funding
The development of the CCRC harmonised cohort was supported by the National Health and Medical Research Council (NHMRC) (APP1009381) with additional support from the Australian Research Alliance for Children and Youth (ARACY) Australian Research Council/NHMRC Research Network (Seed Funding 2009). The National Drug and Alcohol Research Centre and the National Cannabis Prevention and Information Centre at UNSW Australia are supported by funding from the Australian Government.
Peter Butterworth is supported by ARC Future Fellowship (FT1301014440). Louisa Degenhardt is supported by an NHMRC Principal Research Fellowship (APP1041742). Delyse Hutchinson is supported by a Vice-Chancellor’s Postdoctoral Fellowship from the University of New South Wales. Richard P Mattick is supported by an NHMRC Principal Research Fellowship (APP1045318). Craig Olsson is supported by an Australian Research Council Principal Research Fellowship (DP 1311459). George Patton is supported by an NHMRC Senior Principal Research Fellowship (APP1019887).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.