
Abstract
‘The most common diseases are the toughest to crack’ [1] noted a recent Science editorial. Such common illnesses are multifactorial in etiology and often have poorly limited boundaries [2]. Unipolar depression is such an illness; it is an ill-defined disorder overlapping with the major anxiety disorders and it is polygenic in etiology [3], [4]. Yet, viewed in terms of the global burden of disease, depression ranks fourth in disability adjusted life years (DALY) [5].
Although clearly familial, the multiple genetic markers putatively linked with depression have been difficult to replicate [6]. A decade ago, a 60-year prospective study of 268 college men, the Study of Adult Development at Harvard, reported that maternal grandfather longevity (MGFL) was negatively associated with clinical depression in probands [7]. This relationship appeared independent of ancestral longevity in relatives other than the maternal grandfather. The mean MGFL of college men with a history of clinical depression was 60.4 years. This was almost 17 years less than the mean MGFL of 77.0 years of men with presumably low affective distress (stable personalities in college who subsequently neither sought psychiatric help nor abused alcohol). Significantly, the MGFL (69.6 years) of 26 men with alcohol abuse without known pre-existing psychopathology was not significantly different from the MGFL (68.8 years) of the remaining non-alcoholic men who were neither high nor low in affective distress. This relationship suggested that MGFL was relatively specific in its association with affective illness.
In our original report, MGFL was significantly and negatively associated with six independent measures of affective distress: midlife psychosocial adjustment, symptoms of depression, Goldberg's General Health Questionnaire (GHQ) [8], the depression scale of the NEO Personality Inventory [9] and two other definitions of psychiatric ‘caseness’ [7]. Maternal grandfather longevity was not significantly correlated with the number of known relatives with either depression or alcoholism. None of the six measures of affective distress were significantly associated with longevity of any of the other five first-degree ancestors.
Since, to date, no one has confirmed or refuted our findings, the current report tests our 10-year-old original finding in three ways. First, if our speculative assumption of a recessive X-linked trait is correct, the brothers of probands with the shortest MGFL should be more anxious/ depressed than the brothers of men with long MGFL. Second, MGFL and affective illness in the probands' mothers should be uncorrelated. Third, in order to characterize the personality trait that appears associated with high and low MGFL the report examines specific personality questionnaire trait items. Finally, the addition of 10 more years of prospective follow-up allowed us to examine in the probands themselves the possible association of longevity with high and low affective distress.
Between 1939 and 1942 Harvard University Health Services chose 268 college sophomores for intensive multidisciplinary study [10], [11]. The students were selected for relative physical and mental health. Interview of the students' parents provided an extensive social and family medical history. Every 5 years until age 80, an internist blind to the rest of each man's record rated a detailed physical examination on a three-point scale: no irreversible significant illness, irreversible illness without significant irreversible disability and irreversible disability [12]. Death certificates were obtained for all the men who had died. Of the original 268 men, 12 died before age 50 (six from combat; none from suicide), 20withdrew from the study and six had unknown MGFL, because of adoption or early proband death. The remaining 230 men are included in this report.
The men were followed young enough so that the age at death of short-lived grandparents could be determined with accuracy from the probands' parents and the men were followed long enough so that all their parents had died. Their ancestors were relatively socially privileged, minimizing adventitious death. As a result, the mean age of grandparents at death was 71 years and that of parents (a 1890 birth cohort) was 73 years for fathers and 79 years for mothers. (Such a long life expectancy for white 25-year-olds from US birth cohorts was not achieved until about 1970) [13]. Originally selected for health, the men's smoking, alcohol abuse, physical health and psychiatric treatment have been prospectively monitored for 60 years by interview and biennial questionnaires. Between 1940 and 2000 information regarding the adjustment of the men's siblings was sought at interviews on four occasions. All variables in this report were assessed by raters blind to ancestral longevity.
Method and results
Replication study: brothers of probands
In an effort to replicate the original results, we selected the full brothers of probands with the shortest and longest MGFL −30–55 years (n=41) and 81–103 years (n=42). Of these 83 probands, 34 had no brothers, 33 had one, 12 had two and four had three brothers – a total of 69 brothers. A physician trained in epidemiology and blind to the study hypothesis abstracted each probands' case records (300–600 pages) to create a 100–400-word life history for each brother. She recorded evidence for affective stability, psychiatric care and depression. Each of three raters including the abstractor, all blind to the study hypothesis, then rated each brother's life history for evidence of affective illness: 1–2=top fifth in ‘stability, cheerfulness, resilience, unlikely to seek tranquilizers or psychotherapy’; 3=unratable (alcoholic, or inadequate data), 4–5=‘evidence of anxiety, depression and psychiatric treatment’. Thirty-one of the 69 brothers had very short and 38 had very long MGFL. Depending on the rater (Fig. 1) out of the 69 brothers 10–25 brothers were rated 1–2 and 11–18 brothers were rated 4–5. Depending on the rater, 26–48 brothers were deemed unratable and assigned a 3. Rater agreement was modest. The weighted kappa was 0.36 [0.21, 0.51] for rater 1 versus 2. It was 0.43 [0.28, 0.58] for rater 1 versus 3 and 0.58 [0.41, 0.74] for rater 2 versus 3. However, as Fig. 1 illustrates for each rater, the classifications were in the predicted direction although the numbers were too small to permit a convincing test of statistical significance.
Association between raters' estimates of affective distress in the probands' brothers and maternal grandfather's longevity (MGFL).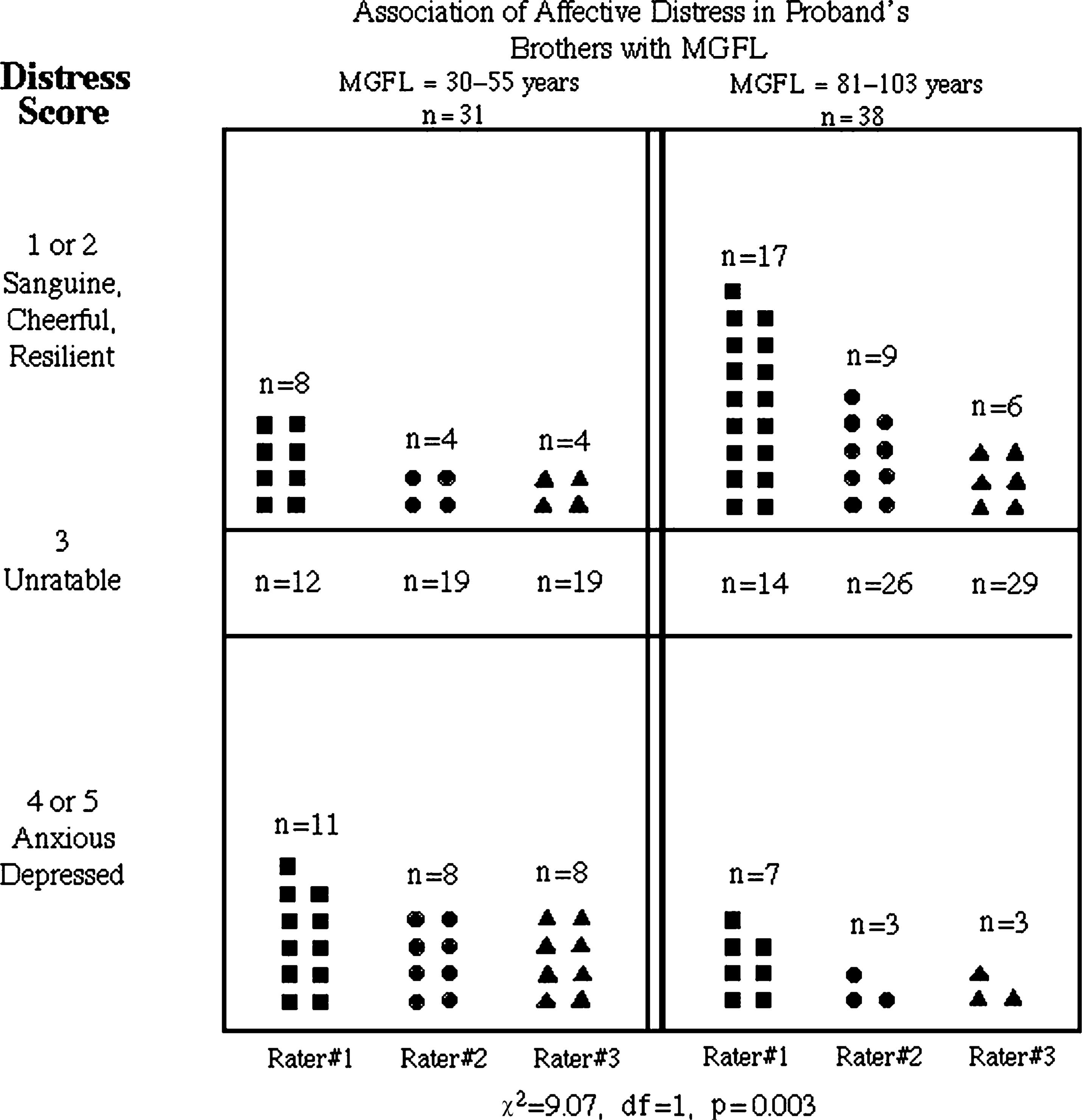
Association of maternal grandfather longevity with multiple diagnoses of affective distress
Table 1 presents the association of MGFL and the proband's own categorical diagnosis of depression at 50 with three operational classifications of affective distress: emotional lability at age 50; objective distress at age 50; and subjective distress (neuroticism) at age 68.
Association of affective distress with maternal grandfather longevity (MGFL)
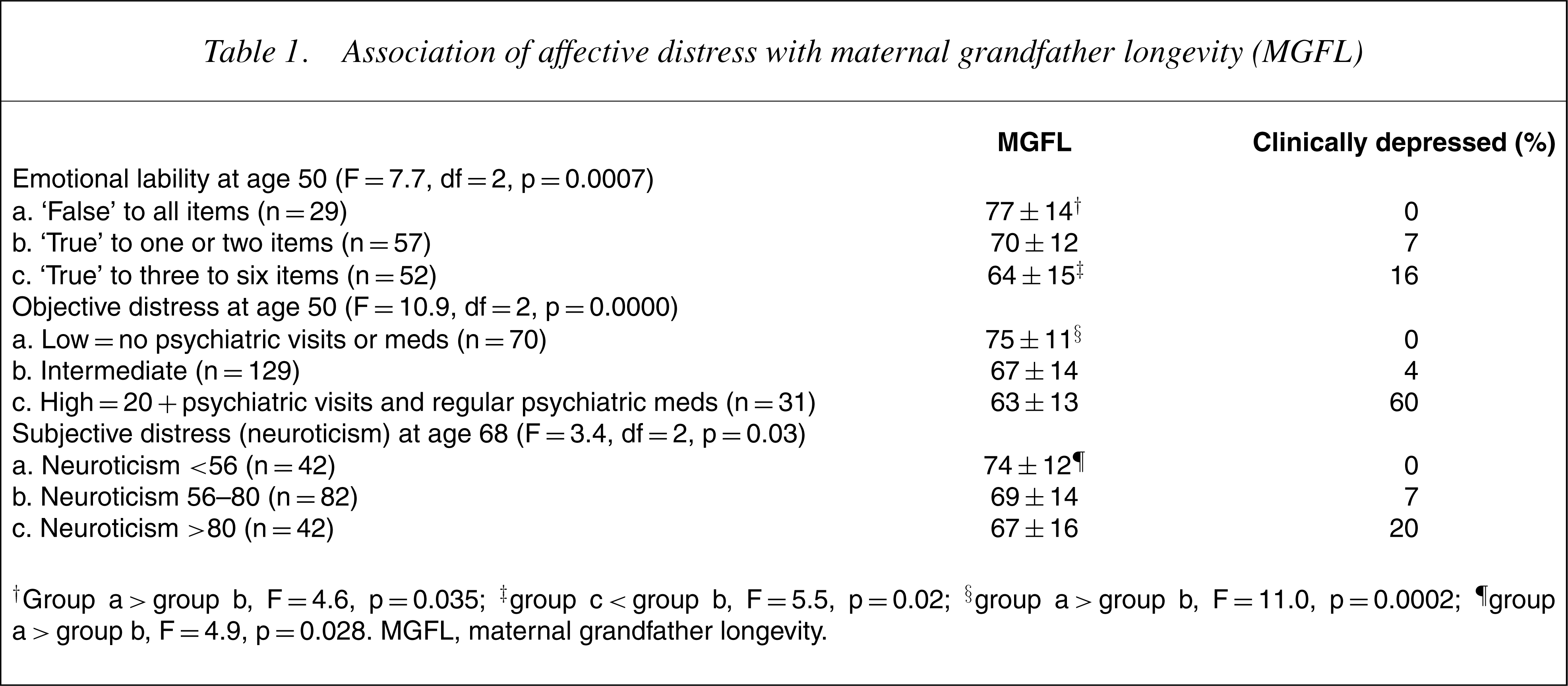
†Group a<group b, F=4.6, p=0.035; ‡group c<group b, F=5.5, p=0.02; §group a<group b, F=11.0, p=0.0002; ¶group a<group b, F=4.9, p=0.028. MGFL, maternal grandfather longevity.
Categorical diagnosis of depression was assessed by two clinically experienced psychiatrists who reviewed the men's 300–600-page records (consisting of multiple interviews and biennial questionnaires over 60 years) for the presence or absence of affective spectrum disorder between ages 20 and 50 [14]. Because the DSM-III criteria for major depressive disorder were not published until the sample was age 60, depressive disorder had to be inferred from data prospectively gathered before age 50. If alcoholism could have caused the depressive symptomatology, the case was excluded. Twenty-three men were defined as clinically depressed at some point between ages 20 and 50. For 13 men both raters agreed, in 10 cases only one rater believed that clinically significant affective illness was present.
The Lazare Personality Inventory (LPI) [15] was administered at age 50. The trait on the LPI, subsequently most highly associated with neuroticism (subjective distress), was the subscale for emotional lability. The individual items for this scale are displayed in Table 2. Four items were significantly associated with MGFL and five (items) with neuroticism assessed 18 years later. Categorically depressed men were twice as likely as men who were not depressed to endorse as ‘true’ items on the scale of emotional lability (F=12.3, p<0.001). As illustrated in Table 1, the 29 men who answered ‘false’ to all the items in Table 2 had unusually long MGFL.
Six-item emotional lability scale (age 50)
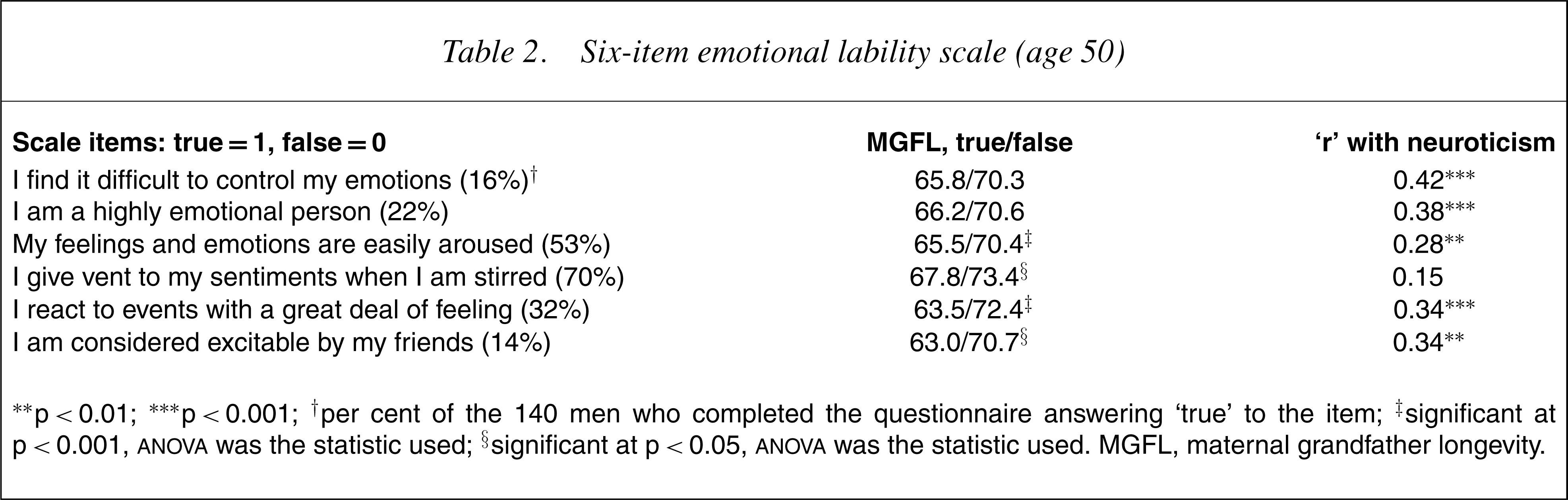
∗p<0.01; ∗∗∗p<0.001; †per cent of the 140 men who completed the questionnaire answering ‘true’ to the item; ‡significant at p<0.001, ANOVA was the statistic used; §significant at p<0.05, ANOVA was the statistic used. MGFL, maternal grandfather longevity.
At age 50, objective distress was defined as ‘low’ (n=70) if men showed a stable personality at age 21 and no visits to a psychiatrist and no use of psychotropic medication by age 50. The presence or absence of a stable personality (steady, stable, dependable and well integrated) had been assessed at age 21 by staff consensus on the basis of 3 years of observation [16]. (Rater reliability was not obtained.) Again, in Table 1, as in Fig. 1, marked absence of objective distress was associated with prolonged MGFL. Objective distress was defined as ‘high’ (n=31) if men had made more than 20 visits to a psychiatrist and had used psychotropic medications (usually antidepressants) for at least a month. This definition encompassed 19 (83%) of the 23 clinically depressed men. The 129 remaining men who did not meet criteria for either the high or low objective distress categories included the other four depressed men.
At age 69±2, subjective distress (neuroticism) was assessed by the NEO Personality Inventory [9], a scale very similar to neuroticism as assessed by the Maudsley Personality Questionnaire [17], [18] The top quartile were contrasted with the middle half and bottom quartile. High scores on trait neuroticism correlate highly with chronic depression. Low scores correlated positively with MGFL. Indeed, an intriguing facet of Table 1 is that the association of MGFL with positive mental health (absence of affective distress) was possibly stronger than with affective illness. For example, the mean MGFL of the 21 men with the very lowest scores on the anxiety subscale of the neuroticism scale was 78±11 years (F=7.4, df=1, p=0.007) when contrasted with the rest of the sample.
Evidence maternal grandfather longevity independent of maternal depression
The mothers were interviewed when the men were in college and family psychiatric problems were recorded in the serial interviews and questionnaires with themen. According to their sons, 24mothers (10%) probably or definitely manifested clinical depression. Maternal depression was positively associated with categorical depression and psychiatric treatment in their sons, but unlike MGFL maternal depression was not correlated with scaled measures of the men's distress or their college personality stability (Table 3). Like low MGFL the number of depressed relatives with depression was positively associated with risk of proband depression (r=0.24, p<0.001), but MGFL was not associated with the number of depressed relatives. If the number of depressed relatives were controlled, all six affective distress variables remained significantly correlated with MGFL. If MGFL was controlled, the number of depressed relatives correlated only with clinical depression and the use of psychiatric medication and psychiatrists.
Correlation between the men's affective distress and maternal depression and longevity
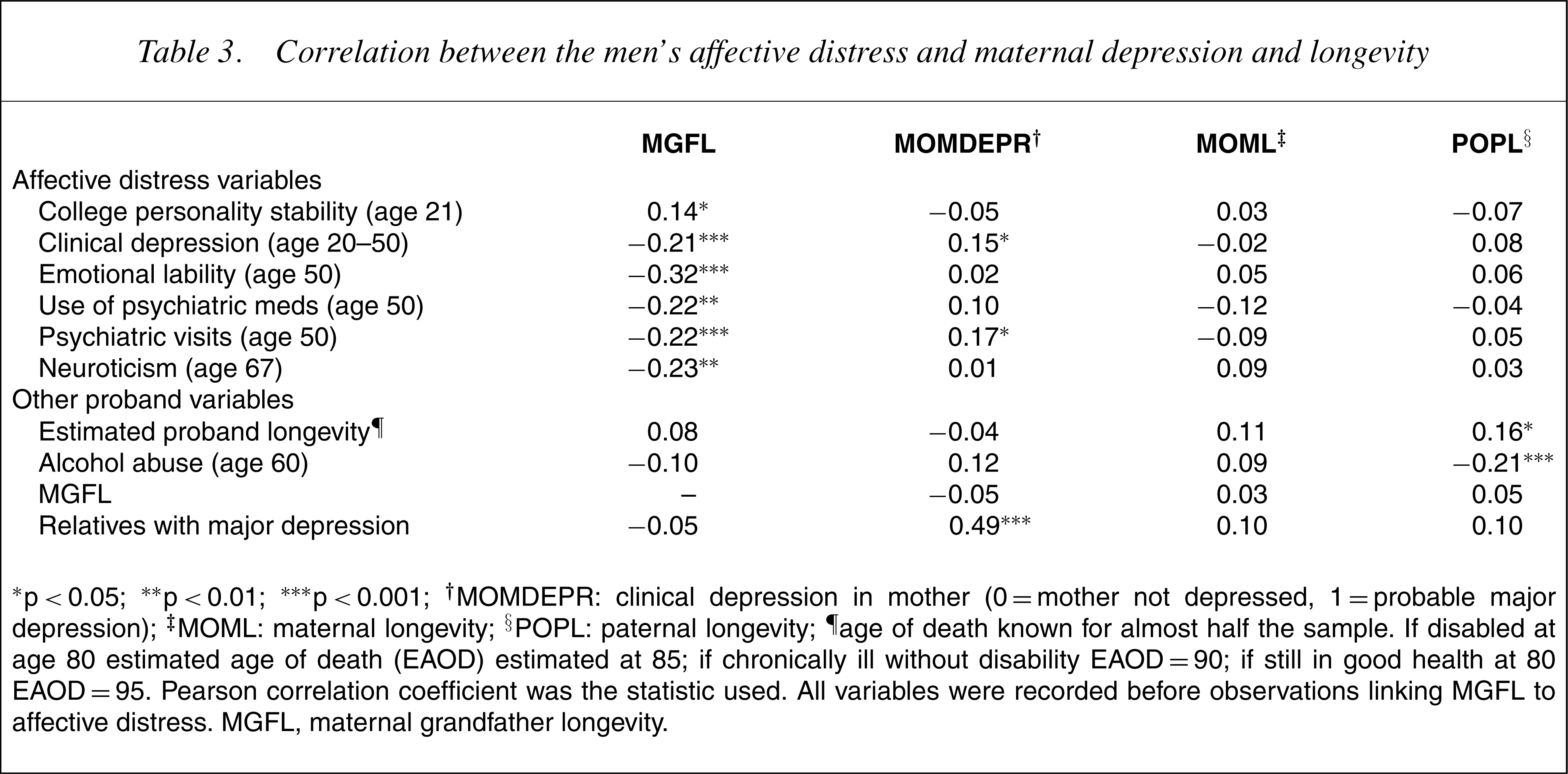
∗p<0.05; ∗∗p<0.01; ∗∗∗p<0.001; †MOMDEPR: clinical depression in mother (0=mother not depressed, 1=probable major depression); ‡MOML: maternal longevity; §POPL: paternal longevity; ¶age of death known for almost half the sample. If disabled at age 80 estimated age of death (EAOD) estimated at 85; if chronically ill without disability EAOD=90; if still in good health at 80 EAOD=95. Pearson correlation coefficient was the statistic used. All variables were recorded before observations linking MGFL to affective distress. MGFL, maternal grandfather longevity.
7].) The expected positive correlation of ancestral longevity with proband longevity and the negative association with alcohol abuse (Table 3) was somewhat stronger for the other ancestors than for the maternal grandfather, especially with the longevity of the proband's father.
Evidence for the association of longevity and affective distress
That MGFL should be a marker for a hereditary facet of affective disorder is not as surprising as it initially might appear. Many other well-controlled studies have linked affective disorder with a twofold increase in premature mortality [19–21]. In our study only seven (10%) of the 70 men, classified before age 50, with the least objective distress had died by age 75 (13]. For each of the three overlapping categories – depressed men, men with the shortest MGFL and men with high objective distress – death from both heart disease and unnatural causes was twice as high as for the rest of the sample. (The numbers of deaths, however, were too small for meaningful statistical test.) This mortality is congruent with the fact that twice as many of the early deaths among MGF with depressed grandsons (7/16, 44%) compared to those of MGF who died early without depressed grandsons (8/36, 22%) were from accident, suicide or alcohol abuse [7].
Association of probands' ‘objective distress’ with mortality. The p values (Pearson's chi-square was the statistic used) contrast mortality of the men with high affective distress and then those with low affective distress with the rest of the entire sample.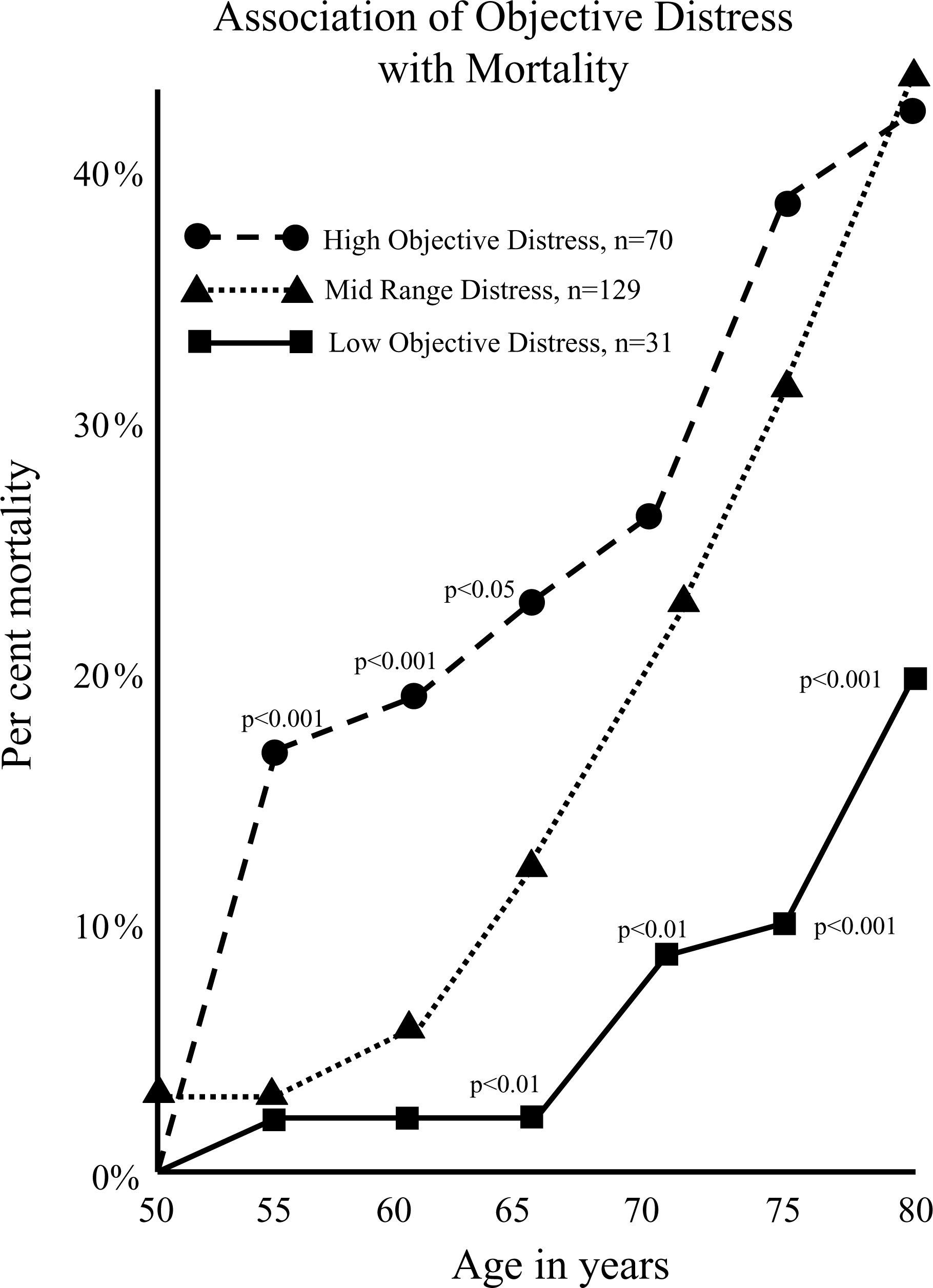
Discussion
Recessive X-linked transmission (e.g. as in the inheritance of hemophilia and colour blindness) would be a possible but speculative explanation for the earlier findings. This explanation is strengthened by the absence in Table 2 of maternal association with key variables. Thus, although the numbers are small, the genetic mechanism identified by MGFL appears different and additive to those reflected by number of depressed relatives. The two measures were essentially uncorrelated with each other (r=−0.05, Table 2) and appeared additive. Four per cent of the 129 men without either short MGFL or definitely depressed relatives were depressed, as were 21% of the 19 men with just depressed relatives and 11% of the 61 men with short MGFL. Thirty-five per cent of the 20 men with both risk factors present were depressed.
Analogous to mental retardation [22], psychiatric vulnerability to depression appears linked to multiple genes [3], [23], [24] and possibly multiple genes on the X-chromosome. If X-chromosome transmission in affective illness also involves a dominant gene, one might expect low rates of father/son transmission and high rates of father/daughter transmission of depression. This has been observed [25]. In addition, the hypothesis that a gene for bipolar disorder is associated with Xq28 phenotypic markers remains plausible if unproven [26]. Several genes from the pseudoautosomal region of the short arm of the X-chromosome [27–29] may make small additional contributions. However, in a recent study a genomic scan of major depressive disorder found no evidence for a gene for depression on X, even when the sexes were analysed separately [30].
To establish firm evidence that a recessive X-linked transmission is involved in an affective illness will require more sophisticated analysis than is possible from our dataset. However, as with the initial discovery of the still unseen planet Neptune by John Couch Adams in 1846 by predictable perturbations in the orbit of Uranus, sometimes we can only first identify important entities in our universe by their systematic distortions of the world around them. Our data point to a new genetic mechanism in affective illness and to one possibly influencing positive mental health as well.
Footnotes
Acknowledgements
This work was supported by research grants KO5-MH00364 and MH42248 from the National Institute of Mental Health.