
Abstract
Separation and divorce are known to be associated with increased risks of a range of mental health problems. Previous research has shown that those who experience a relationship separation or divorce have increased rates of depression, substance use disorders, and poorer general mental health [1–9]. Although the majority of previous studies in this area have focused on the effects of the divorce or separation of a marriage relationship, some recent studies have also reported that the separation of a non-marriage cohabiting relationship is associated with poorer mental health [2,10].
While the association between separation and mental health has been well established, there has been debate over the causal direction of the relationship. While it is possible that the stress and changes that accompany separation increase the risks of subsequent mental health problems, an alternative explanation is that mental health problems place strain on a relationship that increases the risk of separation or divorce. However, a limitation of many previous studies of separation and mental health is that they have used cross-sectional data and therefore have not been able to distinguish between these different causal pathways. A better approach to addressing issues of causality is to use longitudinal data measuring separation and mental health across several time periods. Studies using longitudinal data have reported that separation leads to increased rates of mental health problems [2,9], but also that mental health problems lead to increased risks of separation [2,10]. These findings suggest that the causal relationship between separation and mental health is complex and causal pathways may run in both directions. In support of this, Bulloch et al. [1] reported that the relationship between major depression and separation was bidirectional, with depressed individuals being more likely to experience a separation or divorce, and those who had separated or divorced being more likely to experience depression. Similarly, Wade and Pevalin [3] examined the association between overall mental health and separation and reported that separation resulted in decreased mental health, and that poor mental health also resulted in an increased likelihood of separation/divorce.
Another limitation of many studies in this area is that they have not adequately controlled for confounding. It is likely that there is a wide range of family background and individual factors that are associated with both separation and mental health problems and may explain the association between these variables. However, many studies have controlled for only a small number of potential covariates [1,2,4,5]. Where longitudinal data are available, another option for controlling for confounding is to use fixed effects approaches [11,12], which estimate the association between a time-dynamic exposure variable (such as separation) and a time-dynamic outcome measure (such as mental health problems) net of any non-observed fixed factors that are associated with the outcome and that may be correlated with the exposure variable. Using this method it is possible to eliminate confounding from non-observed fixed factors. This model can also be modified to include time-dynamic covariate factors in order to control for time-dynamic sources of confounding. Very few previous studies of the association between separation and mental health have used fixed effects methods. However, studies that have used fixed effects methods have reported that separation was associated with decreased scores on a general mental health measure, even after control for fixed and time-dynamic sources of confounding [3,13].
There has been some suggestion that the associations between separation and mental health may be different for men and women [4,14]. For example, Kolves et al. [14] reported that the risk of suicidal behaviour following separation was higher for men than for women. However, findings from other studies have been inconsistent, with some reporting that the effects of separation on mental health are greater for women than for men [15], or are the same for both genders [6,16].
Against this background this study examines the associations between separation and a range of mental health problems using longitudinal data from a birth cohort of individuals born in Christchurch, New Zealand in 1977 and followed to age 30. It will use standard covariate adjustment methods and also fixed effects approaches to adjust the associations between separation and mental health for confounding. The specific aims of the study are:
To examine the associations between the separation of a cohabiting relationship and mental health problems including depression, anxiety disorders, suicidal behaviour, alcohol abuse/dependence, and illicit drug abuse/dependence.
To adjust the associations between separation and mental health problems for a wide range of observed and non-observed confounding factors using both standard covariate adjustment and fixed effects approaches.
To examine whether the associations between separation and mental health are similar for men and women.
Methods
Sample
Data were collected as part of the Christchurch Health and Development Study, a longitudinal study of a birth cohort of 1265 individuals born in Christchurch, New Zealand in 1977 and followed to age 30. Participants were followed up at birth, 4 months, 1 year, yearly to age 16, then again at ages 18, 21, 25 and 30 using a combination of semi-structured interviews, standardized testing, and teacher reports. All information was collected on the basis of signed informed consent from study participants. The major findings of this study have been reviewed previously [17,18].
Measures
Mental health problems
At ages 21, 25 and 30 participants completed a comprehensive mental health interview that assessed the extent to which they had suffered from symptoms of depression, generalized anxiety disorder, panic disorder, social phobia, specific phobias, agoraphobia, and substance abuse and dependence during the period since the last interview. This interview was based on the Composite International Diagnostic Interview [19]. Responses to interview questions were used to determine the presence or absence of a series of psychiatric disorders in the 12 months preceding the interview based on DSM-IV [20] criteria (see Fergusson et al. [21] for a more detailed explanation of the criteria used). In addition, participants were questioned using custom written survey items about the occurrence of suicidal thoughts or suicide attempts over the preceding 12 months. Responses to the above questions were used to construct the following measures of mental health problems over the 12 months preceding the interview.
Depression
This measure represented the presence or absence of a diagnosis of major depression during the 12 months preceding the interview.
Anxiety disorder
This measure represented the presence or absence of any anxiety disorder diagnosis (generalized anxiety disorder, panic disorder, social phobia, agoraphobia, or specific phobia) during the 12 months preceding the interview.
Suicidal ideation/attempt
This measure represented whether or not participants reported either suicidal ideation (contemplating, considering, or planning suicide) or suicide attempt during the 12 months preceding the interview (see Fergusson and Lynskey [22] for a more detailed description of this measure).
Alcohol abuse/dependence
This measure represented the presence or absence of a diagnosis of either alcohol abuse or alcohol dependence during the 12 months preceding the interview.
Illicit drug abuse/dependence
This measure represented the presence or absence of a diagnosis of cannabis or other illicit drug abuse or dependence during the 12 months preceding the interview.
Total number of psychiatric disorders
A measure of the overall burden of mental health problems was based upon a count of the number of mental health problems reported by the participant at each age. This measure was the sum of the five dichotomous mental health problem measures described above.
Separation
At ages 21, 25 and 30, participants were asked whether they had experienced a separation from a cohabiting partner or spouse in the 12 months preceding the interview. Overall, 6.2% of participants reported a separation at age 20–21, 10.3% at age 24–25, and 6.7% at age 29–30.
Covariate factors
To control the associations between separation and mental health for confounding a range of potential covariate measures were selected from the study database.
Fixed measures
These included measures of: family background (parental history of offending, illicit drug use, and alcohol abuse; maternal age; maternal education; paternal education); childhood family functioning (family socioeconomic status at birth; parental changes to age 15; family living standards age 0–10; exposure to childhood adversity to age 15); child abuse (sexual abuse and physical punishment before age 16); cognitive ability and academic achievement (total IQ age 8/9; age left secondary school; Test of Scholastic Abilities score age 13; teacher-rated academic performance age 11–13); individual characteristics and behaviours (neuroticism age 14; novelty seeking age 16; deviant peer affiliations age 16; mother-rated conduct problems age 16; ethnicity; early sexual intercourse); religiosity (importance of religion in childhood home; importance of religion at age 30); and gender.
Time-dynamic measures
These included measures of: mental health problems in the previous interview period (depression, anxiety, suicidal ideation/attempt, alcohol abuse/dependence, illicit drug abuse/dependence in the preceding interview period); life events in the previous 12 months (employment problems; death of family/friend; family arguments; serious illness of self or family/friend; being a victim of burglary, robbery or assault); number of dependent children at the time of interview; and relationship factors (relationship separation during previous interview period, formation of a new cohabiting relationship within the previous 12 months; having a cohabiting partner at the time of interview).
Statistical methods
The associations between the repeated measures of separation and mental health were tested for statistical significance by fitting two types of regression model.
Generalized estimating equation model
The pooled data from the three time periods (ages 20–21, 24–25, and 29–30) were fitted with population averaged generalized estimating equation (GEE) models [23,24] in which the mental health problem was modelled as a function of separation and, where applicable, a series of potential covariate factors (see above for a list of these factors). All covariate factors were initially included in the model, and the model was then refined to include only those covariates that were significant (p < 0.05) predictors of the outcome.
For dichotomous outcomes the model fitted was of the form:


The GEE models were also fitted using separation as the dependent variable and the mental health problem measure as the independent variable.
To test the equivalence of the effect of separation on each outcome for men and women the fitted regression models were extended so that the effect of separation was nested within gender. The equality of the coefficients B1 for men and women was then tested using a Wald chi-squared test.
All GEE models were fitted using SAS 9.1 for Windows.
Fixed effects model
The pooled data from the three time periods were fitted with fixed effects logistic regression models (for the dichotomous outcomes) or fixed effects Poisson regression models (for the count outcome) in which the mental health problem was modelled as a function of separation, unobserved fixed and observed time-dynamic factors (see Covariate factors, above, for a list of these factors) [11,12]. For dichotomous outcomes the model fitted was of the form


The fixed effects models were also fitted using separation as the dependent variable and the mental health problem measures as the independent variables.
To test the equivalence of the effect of separation on each outcome for men and women the fitted regression models were extended so that the effect of separation was nested within gender. The equality of the coefficients B1 for men and women was then tested using a Wald chi-squared test.
Fixed effects models were fitted using STATA 10.0 for Windows.
In order to provide an estimate of effect size, rate ratios and corresponding 95% confidence intervals were calculated using the parameters B1 from the above models. For the total number of mental health problems outcome this ratio was the incident rate ratio (IRR), for all other outcomes it was the odds ratio (OR).
Results
Table 1 shows the associations between separation and a range of mental health problems, including depression, anxiety disorder, suicidal ideation/attempt, alcohol abuse/dependence, illicit drug abuse/dependence, and total number of mental health problems, pooled over the three time periods (age 20–21, 24–25, 29–30). For each mental health problem, the table shows the rate ratio and 95% confidence interval for the effect of separation, and the p value for significance from the GEE model. For the total number of mental health problems outcome the rate ratio was the incident rate ratio (IRR), for all other outcomes it was the odds ratio (OR). The table shows that separation was significantly associated with all of the mental health problem measures (p <.05). The size of the effect, as measured by the rate ratio, ranged from 1.5 to 3.6 with a median value of 2.0.
Unadjusted associations between separation and mental health problems
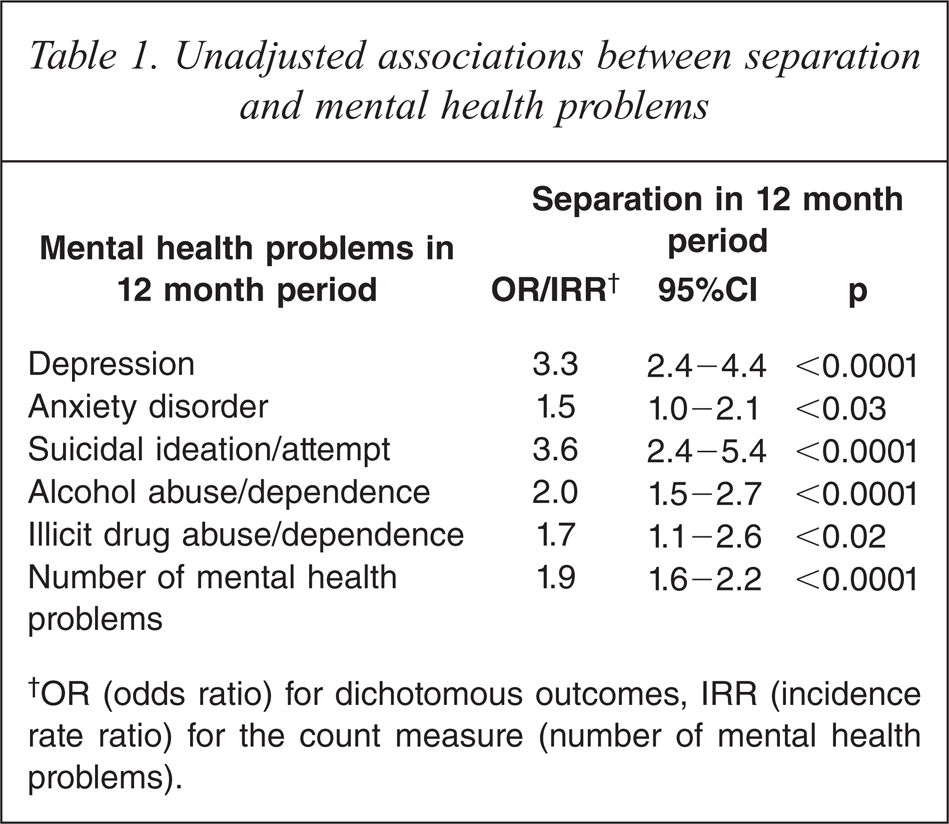
†OR (odds ratio) for dichotomous outcomes, IRR (incidence rate ratio) for the count measure (number of mental health problems).
Adjustment for confounding
In order to adjust the associations between separation and mental health problems for confounding, the data in Table 1 were fitted with two types of regression models: a GEE model, in which the mental health outcome was modelled as a function of separation and a series of fixed and time-dynamic covariate factors (see Methods for a full list of these factors), and a fixed effects model, in which the mental health outcome was modelled as a function of separation and a series of time-dynamic factors (see methods for details of the regression models). The models were also fitted using separation as the dependent variable and the mental health outcome as the independent variable. The models initially included all covariates and were gradually refined to include only those covariates that were significant (p < 0.05) predictors of the outcome measure.
Table 2 shows the results of the regression models. The results of the population-averaged GEE models are in the left panel of the table. When mental health problems were used as the dependent variables, in almost all cases there remained a significant association between separation and mental health problems after adjustment for covariate factors. The only exception was illicit drug abuse/dependence, where the association was marginally significant (p < 0.08). When separation was used as the dependent variable, in all cases there remained a significant association between separation and mental health problems (p < 0.05) after adjustment for covariate factors. The adjusted rate ratios for the association between separation and mental health problems were small and ranged from 1.5 to 4.0 with a median value of 1.8. The largest ratios were for depression and suicidal ideation/attempt, where the odds ratios were 3.5 or above.
Adjusted associations between separation and mental health problems
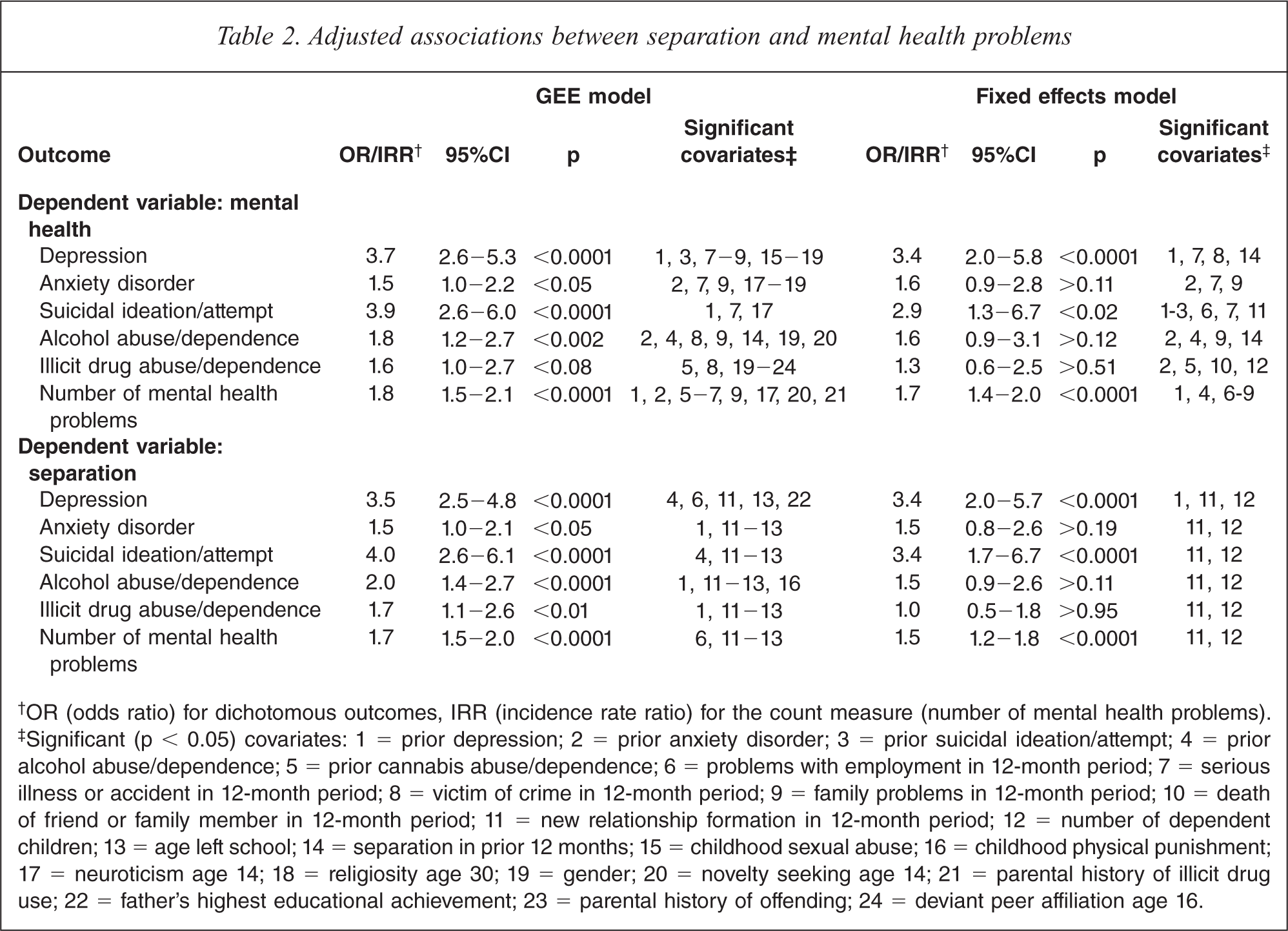
†OR (odds ratio) for dichotomous outcomes, IRR (incidence rate ratio) for the count measure (number of mental health problems).
‡Significant (p < 0.05) covariates: 1 = prior depression; 2 = prior anxiety disorder; 3 = prior suicidal ideation/attempt; 4 = prior alcohol abuse/dependence; 5 = prior cannabis abuse/dependence; 6 = problems with employment in 12-month period; 7 = serious illness or accident in 12-month period; 8 = victim of crime in 12-month period; 9 = family problems in 12-month period; 10 = death of friend or family member in 12-month period; 11 = new relationship formation in 12-month period; 12 = number of dependent children; 13 = age left school; 14 = separation in prior 12 months; 15 = childhood sexual abuse; 16 = childhood physical punishment; 17 = neuroticism age 14; 18 = religiosity age 30; 19 = gender; 20 = novelty seeking age 14; 21 = parental history of illicit drug use; 22 = father's highest educational achievement; 23 = parental history of offending; 24 = deviant peer affiliation age 16.
The results of the fixed effects models are in the right panel of the table. Overall, the adjusted odds ratios from the fixed effects models were smaller than those from the GEE models, and the associations were less likely to be significant. When mental health problems were used as the dependent variable, after adjustment for observed time-dynamic factors and non-observed fixed sources of confounding there remained a significant association between separation and three of the mental health problem measures (depression, p < 0.0001; suicidal ideation/attempt, p < 0.02; and number of mental health problems, p < 0.0001). However, after adjustment for observed and non-observed sources of confounding there was no longer any significant association between separation and anxiety disorder (p > 0.11), alcohol abuse/dependence (p > 0.12) or illicit drug abuse/dependence (p > 0.51). A similar pattern was apparent when separation was used as the dependent variable. After adjustment there remained significant associations between separation and depression (p < 0.0001), suicidal ideation/attempt (p < 0.0001), and number of mental health problems (p < 0.0001). However, there were no longer any significant associations between separation and anxiety disorder (p > 0.19), alcohol abuse/dependence (p > 0.11) or illicit drug use/dependence (p > 0.95). The adjusted rate ratios for the associations between separation and mental health problems were small and ranged from 1.3 to 3.4 with a median value of 1.6. The largest rate ratios were for depression and suicidal ideation/attempt, where rate ratios were 2.9 or larger.
Gender differences
In order to examine whether the adjusted associations between separation and mental health were different for men and women, the models in Table 2 were extended so that the effects of the main independent variable (separation or the mental health problem measure) were nested within gender. In each case the equality of the regression coefficients for men and women was tested for statistical significance using a chi-squared test. This analysis revealed no significant gender differences (all p > 0.10).
Discussion
This paper examined the associations between relationship separation and a range of mental health problems using longitudinal data from a birth cohort of individuals born in Christchurch, New Zealand in 1977 and followed for 30 years. The associations were adjusted for confounding using standard covariate adjustment methods and also fixed effects approaches. The major findings from this study were:
Before adjustment for covariates, separation was associated with a range of mental health problems including depression, anxiety disorders, suicidal ideation/attempt, alcohol abuse/dependence, illicit drug abuse/dependence, and total number of mental health problems.
After adjustment for fixed and time-dynamic sources of confounding using fixed effects models, there remained significant associations between separation and depression, suicidal ideation/attempt, and number of mental health problems. These associations were apparent both when separation was used as the dependent variable and when mental health problems were used as the dependent variable.
After adjustment for fixed and time-dynamic sources of confounding using fixed effects models, separation was not significantly associated with anxiety disorder, alcohol abuse/dependence, or illicit drug abuse/dependence
The associations between separation and mental health problems were similar for men and women.
These findings are consistent with previous research which has suggested that, when due allowance is made for confounding, separation is associated with increased rates of depression, suicidal behaviour, and overall higher levels of mental health problems [3,13]. However, the finding that the associations between separation and mental health were similar for men and women contrasts with some previous research which has reported that the effects of separation on mental health are different for men and women [4,14,15].
Adjusting for confounding in this study reduced, but did not eliminate, the significant associations between separation and depression, suicidal behaviour, and total number of mental health problems. The associations were reduced to a greater extent by the fixed effects model than the GEE model. This suggests that, in order to adequately control for confounding, it may be useful for future studies to employ fixed effects methods rather than standard covariate adjustment methods.
A range of covariate factors were significant predictors in the models. These spanned domains of prior mental health problems, negative life events, relationship history, number of children, and family and socioeconomic background. Although few previous studies have controlled for covariate factors, those that have done so have reported covariates that are consistent with those in the current study, including socioeconomic status, parental status, and number of children [3,10].
Although separation was significantly associated with mental health in the present study, the size of the effect, after adjustment for fixed and time-dynamic confounding factors, was small. Where there was a significant association between separation and mental health problems, adjusted rate ratios from the fixed effects model ranged from 1.5 to 3.4 with a median value of 3.2.
The results of the current study suggested that mental health problems are predictive of separation, but also that separation is predictive of mental health problems. This is consistent with previous studies which have also suggested that the relationship between separation and mental health problems may be bidirectional [1,3]. However, in the current study it was not possible to determine the precise causal relationship between mental health problems and separation. Previous research has suggested that the effects of separation on mental health problems may be short term [13], suggesting that it may be difficult to address issues of causality using longitudinal data sets where data is collected at intervals of several years. Therefore, the best approach to addressing the causal associations between separation and mental health problems may be to use randomized controlled trials to examine whether interventions for mental health problems reduce rates of subsequent relationship separation, and conversely, whether interventions for those experiencing a relationship separation reduce rates of subsequent mental health problems.
A limitation of this study is that the participants were relatively young (ages 21, 25 and 30) when data regarding relationship separation and mental health problems were collected. It is possible that many of the relationship separations at these ages may have lesser impacts on mental health than relationship separations at older ages, when relationships would be more established and would be more likely to involve dependent children.
This limitation notwithstanding, the results of the current study suggest that the separation of a cohabiting relationship is associated with significantly increased rates of depression, suicidal behaviour, and total mental health problems, even after due allowance has been made for confounding factors.
Footnotes
Acknowledgements