
Abstract
Major depression is expected to become the second leading contributor to disease burden worldwide by 2020 [1]. A recent epidemiological study found a 12 month prevalence of mood disorder of 0.8–9.6% around the world [2]. In Japan, Kawakami et al. reported a corresponding prevalence rate of 3.1% [3].
Because of its chronic nature, the economic burden posed by depression on the health-care system is profound. But the burden may be even higher when it is evaluated from the societal perspective, because the indirect costs related to depression are also profound [4].
With respect to the total costs of dealing with depression, estimates have been reported from different settings. In the USA Greenberg et al. estimated a total cost of dealing with depression of USD 43.7bn in 1990 [5]. They also reported that 76% of the total cost was accounted for by indirect costs. In the UK, Kind and Sorensen found a total cost of dealing with depression of GBP 3.4bn in England and Wales in 1990, and that 86.7% of it was accounted for by indirect costs [6]. Thomas and Morris, who reassessed it in 2000, found that the total cost had climbed to GBP 9bn, with indirect costs accounting for 96% [4].
Even in Japan, although no precise epidemiologic or economic data are available, the rapid increase in the number of suicides, to more than 30 000 per year [7], and the escalation in absenteeism from the workplace due to depression imply rapid growth of the burden posed by depression.
In contrast, due to reasons such as the rapid aging of society and slow economic growth, more efficient use of the available resources in Japan has become critical even in the health-care setting, similar to the case in many other developed countries. This makes evaluation of the most cost-effective interventions for managing depressed patients a critical issue.
Since the 1980s, many cost–effectiveness analyses comparing selective serotonin re-uptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs) have been conducted [8–11]. A meta-analysis of these reports indicated that SSRIs are effective and more cost-effective as compared to TCAs for the treatment of depression [12].
Furthermore, many studies have found that cognitive behavioural therapy (CBT) is as effective as or more effective than antidepressant drug therapy for depression [13–15]. Thus, combined antidepressant therapy with CBT has come to be expected to be more effective than either antidepressant therapy or CBT alone. Several studies to date have ascertained the short-term effectiveness of combined therapy [16, 17], but the number of studies is limited as compared to the number of studies conducted to compare different antidepressants or antidepressant therapy alone with CBT alone. Moreover, in regard to the cost-effectiveness analysis, a literature review showed that only two cost-effectiveness analyses comparing combined therapy and antidepressant therapy alone have been performed [18, 19]. Also, no research has ever been conducted in the Japanese setting.
Therefore, in order to identify whether or not combination therapy is cost-effective compared to antidepressants therapy in Japan, cost-effectiveness and cost-utility were examined by constructing a decision analytical model that summarized the most reliable clinical evidence and combined it with relevant cost data.
Method
Model structure
In order to estimate the cost-effectiveness of combined therapy of CBT and antidepressant therapy (COMBI) versus antidepressant therapy (AD) alone, a formal decision analytical model with a summary of the clinical outcomes combined with the relevant cost data was constructed. Although it is technically possible to set the study period much longer, research review indicates that there is only one study with 26 samples that focused on clinical difference between COMBI and AD and which had a follow up >12 months [13]. We judged that the sample size was too small to use it in the present analysis, therefore, the study period was set at 12 months.
Perspective
The analysis was conducted from the health-care system perspective as well as from the societal perspective.
Clinical outcome and event probabilities
Clinical outcomes were measured primarily by the proportion of successfully treated patients and also by the gain in quality-adjusted life years (QALYs). Clinical probabilities were derived from meta-analyses, randomized controlled trials (RCTs) and reports of expert panels.
With regard to initial treatment, the clinical probabilities were based on the meta-analysis of eight RCTs in the guideline for depression established by National Institute for Clinical Excellence (NICE) [12].
The clinical parameters during maintenance therapy and the observation period were derived from the RCT conducted by Blackburn et al. [20] and Simons et al. [21].
Because of the absence of data regarding the relapse rate within 9 months after initiating therapy, in the present study this rate was assumed to be equal to the relapse rate within 12 months reported in the aforementioned studies.
Data regarding switching strategies from SSRIs to TCAs were collected from the RCT performed by Thase et al. [22].
In this analysis, the dichotomous outcome measure of ‘no response to treatments’ was defined as scores >6 on the 17-item HRSD, or >8 on the 24-item HRSD. To evaluate the benefit in terms of QALYs, utility data were obtained from a published study in which patient-assigned health state utilities were reported by depression severity and antidepressant medication [23].
Because no patient-level data were available to calculate the costs for the economic evaluation, deterministic costing of the different treatment strategies was carried out. The clinical parameters used in the analyses are shown in Table 1.
Clinical parameters
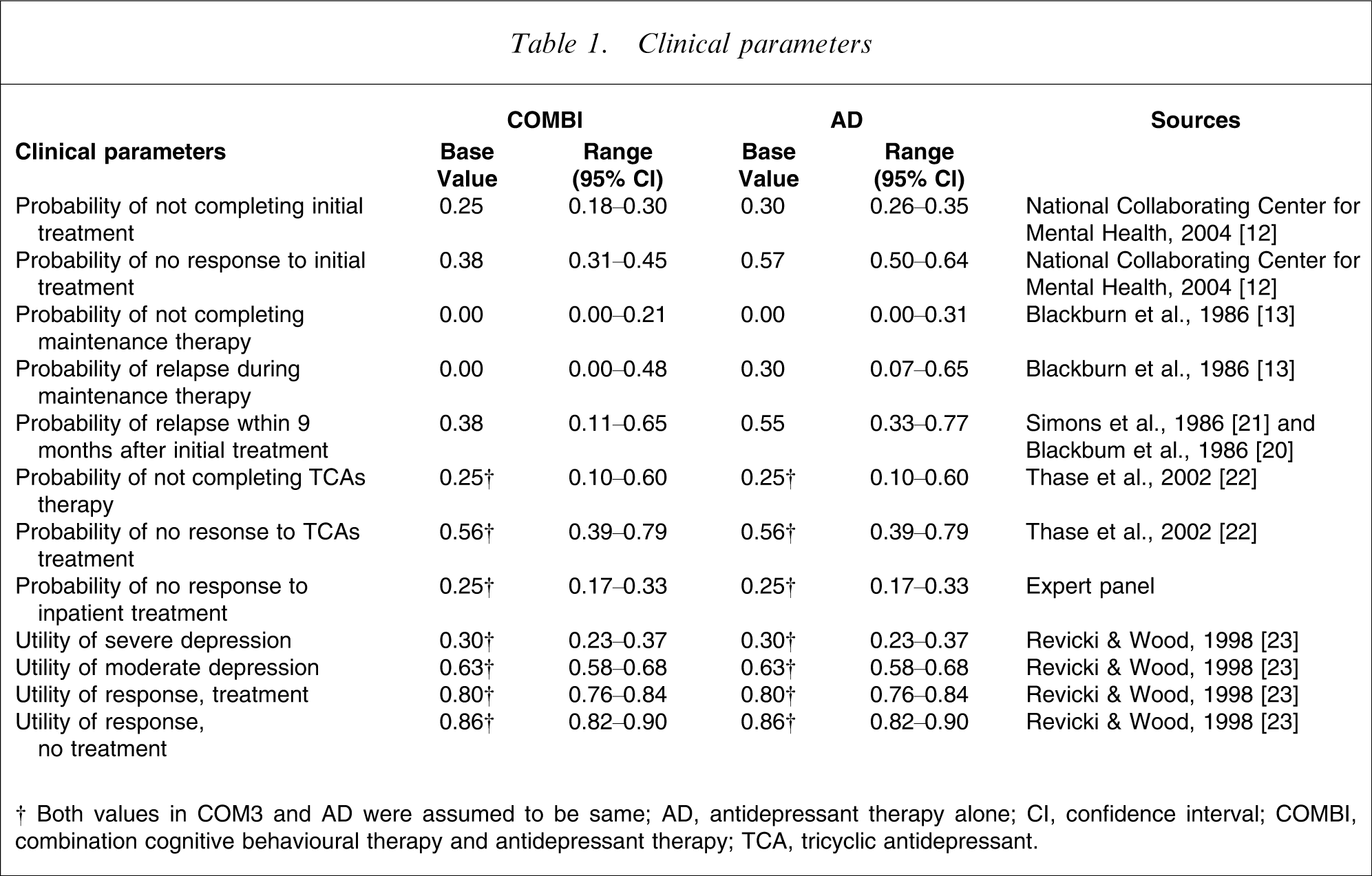
†Both values in COM3 and AD were assurred to be same; AD, antidepressant therapy alone; CI, confidence interval; COMBI, combination cognitive behavioural therapy and antidepressant therapy; TCA, tricyclic antidepressant.
Expert panels
A literature review found minimal information about resource use by patients who discontinue treatment. Therefore, we constructed an event tree (Figure 1) and constituted an expert panel composed of eight Japanese psychiatrists. Experts were asked about each probability relevant to the decision trees. Probabilities relating to discontinuation (2), (4) and (5) were treated as being equivalent, because all represented treatment discontinuation during maintenance therapy.
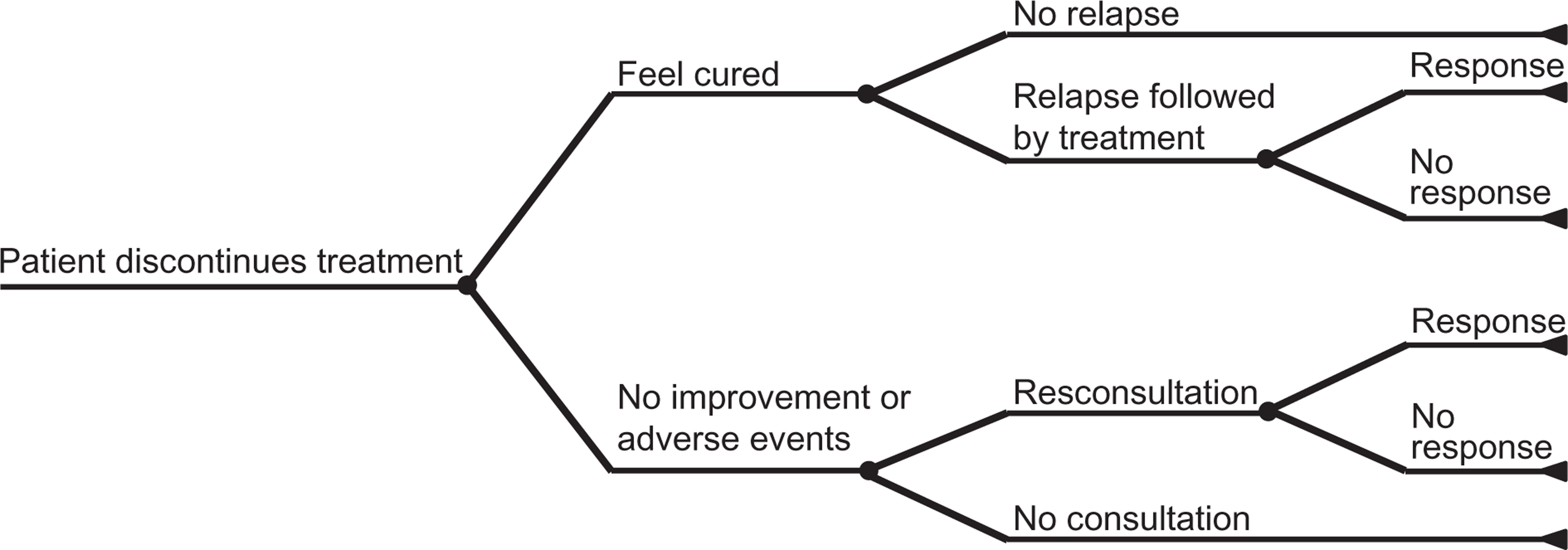
Decision analytical tree for management of patients who discontinue treatment.
The decision tree for the expert panel is shown in Figure 1 and the results are listed in Table 2.
Clinical parameters of patients who discontinued treatment
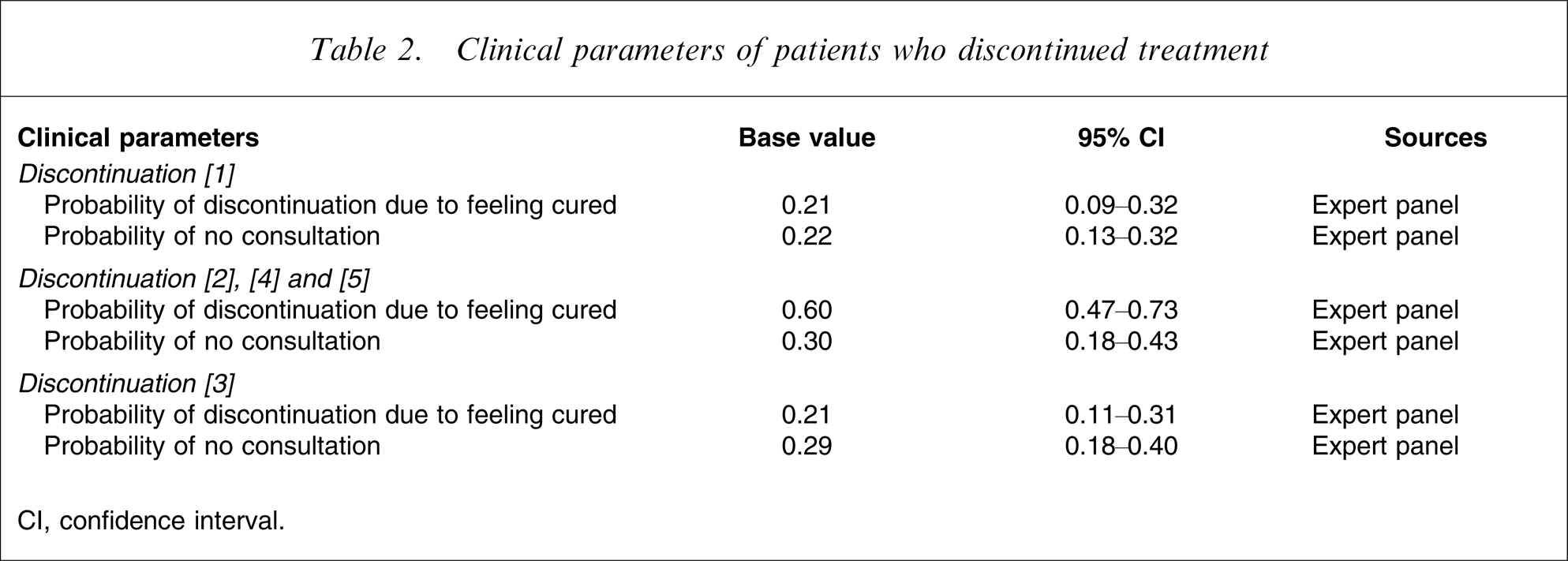
CI, confidence interval.
Direct and indirect costs
Costs were evaluated primarily from the health-care system perspective, and then from the societal perspective. Direct costs for the health-care system included medication costs, consultant fees, psychotherapy fees and inpatient treatment costs. Unit costs of health-care services were collected from the published data by the Japanese government [24, 25].
Total costs from the societal perspective involved both direct costs and indirect costs. Indirect costs here were assumed to be equal to productivity loss due to absence from work. The cost of individuals being absent from work was calculated by dividing the gross domestic product of Japan in 2005 [26] by the proportion of the population eligible to work and by a 12 month period. The details of the unit costs are listed in Table 3.
Unit costs
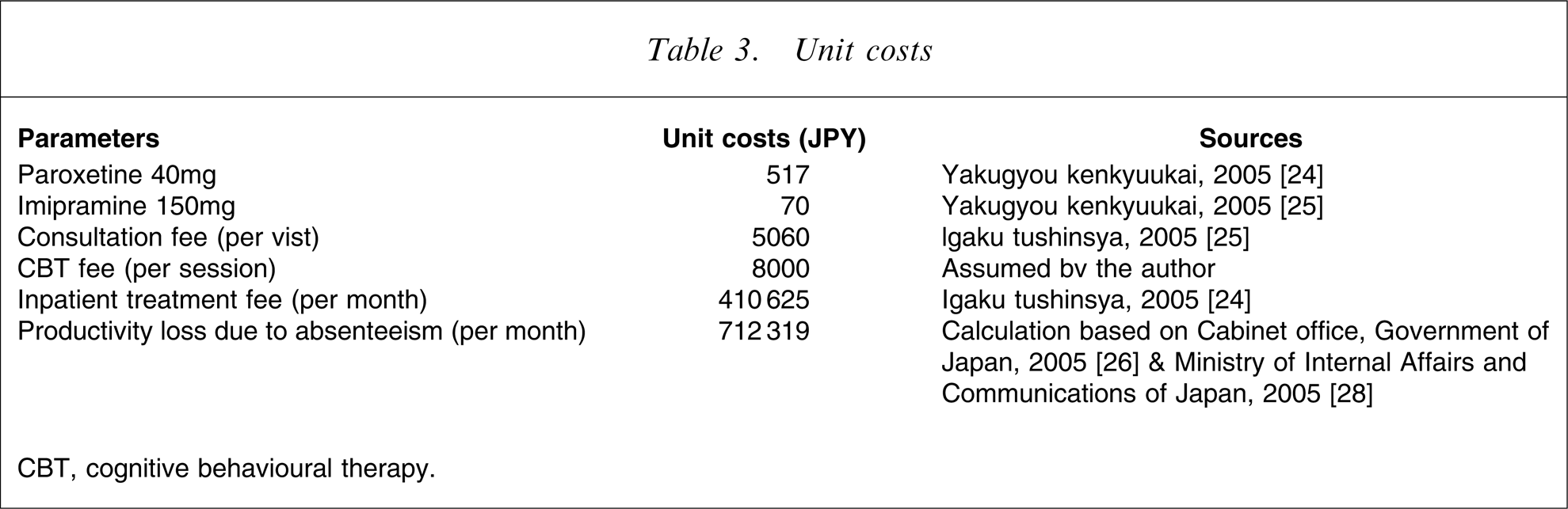
CBT, cognitive behavioural therapy.
Decision analytical models
The estimated resource use for health care was integrated with the clinical outcomes in order to assess the cost-effectiveness of COMBI as compared with that of AD alone. By assigning cost to health-care use, the models primarily estimated the expected total cost borne by the health-care system for treating patients with moderate or severe depression. In addition, this model also examined the total expected cost from the societal perspective by including indirect costs.
Assumptions of the model
COMBI and AD
We assumed that patients enrolled were ≥18 years. The patients allocated to COMBI had weekly consultations with a psychiatrist, 40 mg of paroxetine per day for 3 months, and 13 sessions of CBT over 3 months, while the patients allocated to AD had weekly consultations with a psychiatrist and 40 mg of paroxetine per day for 3 months. Patients who completed initial treatment and responded to it received maintenance therapy for 6 months. During maintenance therapy, patients were given half-dose medication as compared with that during initial treatment and had consultations with a psychiatrist every 2 weeks. The relapse period during maintenance therapy was set at 3 months. Patients who completed initial treatment but who did not respond to it received 150 mg of imipramine for 3 months. Patients who completed TCA therapy and responded to it received maintenance therapy for 6 months. Patients who completed TCA therapy but who did not respond to it were hospitalized for 93.6 days [27]. Patients who went into remission on inpatient treatment received maintenance therapy for 3 months. Patients who did not respond to inpatient treatment continued to receive TCA treatment after discharge for 3 months. All patients who discontinued the treatment before the end of the study were assumed to consume health-care resources even after discontinuation. A total of 58.4% of all patients were employed before they began to suffer from depression [28]. Patients were absent from work while they suffered from depression, irrespective of the severity, if they were employed before they began to suffer from depression. They were able to return to work, however, when they no longer suffered from depression. The cost of adverse events, such as patients taking an overdose of antidepressants, would not influence the cost difference between the two therapeutic arms because the drug protocols used in the two treatment strategies were identical.
Managing patients who discontinued the treatment
Each patient who discontinued the therapy (including maintenance therapy) discontinued it at the midpoint of the treatment. The reasons for the discontinuation fell into two groups: remission; and no response or development of adverse events. All patients who relapsed after discontinuation were assumed to consult physicians again. The relapse period was assumed to be the midpoint between the discontinuation and the end-point of the study. Those who consulted physicians again after discontinuation due to absence of response or development of adverse events were assumed to see them at the midpoint between the discontinuation and the study end-point. The patients who discontinued the treatment and never consulted physicians again regardless of the remission status were assumed to continue to suffer from depression until the end of the study.
Discount rate
When evaluating costs, no discount rate was considered because the study period was 12 months.
Economic evaluation
The economic evaluations were carried out primarily by determining the incremental cost-effectiveness ratios (ICERs) per successfully treated patient and second by the ICERs per QALY.
Sensitivity analysis
To explore the uncertainty around individual parameters, one-way sensitivity analyses were conducted for seven scenarios by varying each single parameter between its 95% confidence interval (CI) while other parameters remained at the base values. Probabilistic sensitivity analyses were also carried out in order to explore the impact of joint uncertainty.
Results
Clinical outcomes
Clinical outcomes were evaluated first by assessing the proportion of successfully treated patients and second by the QALY gain. The results indicate that COMBI, as compared to AD, increased the proportion of successfully treated patients by 0.15: the QALY gain was 0.08 in severe depression and 0.03 in moderate depression. The details are shown in Table 4.
Costs
Health-care system perspective
The total cost for COMBI was JPY 449 655 per patient, whereas that for AD was JPY 422 244 per patient. The result showed that COMBI costs more than AD by JPY 27 411 per patient. This implies that the higher acquisition cost of COMBI was almost offset by the lower cost of managing patients not responding to initial treatment and relapsing during maintenance therapy.
Societal perspective
The total costs from the societal perspective amounted to JPY 3 106 484 for COMBI and JPY 3 800 342 for AD. The higher direct cost of COMBI was completely offset by the reduction of productivity loss by COMBI as compared to that by AD.
Cost-effectiveness
The ICERs were calculated by dividing the difference in costs between COMBI and AD by the difference in effectiveness between them (first the proportion of successfully treated patients, and second the QALY gain). Analyses were carried out both from the health-care system perspective and the societal perspective.
Health-care system perspective
Successfully treated patients
Using a decision analytical model, treating depressive patients with COMBI appeared to increase the proportion of successfully treated patients by 15% as compared to that with AD (from 14% to 29%). At the same time, COMBI was found to be more costly by JPY 27 411 as compared with AD. Thus, the ICER was determined to be JPY 182 740 per successfully treated patient.
QALYs
The ICER per QALY gained for patients with severe depression was JPY 342 638, whereas that for patients with moderate depression was JPY 913 700 per QALY gained.
The results of the ICERs per QALY gained indicate that COMBI may be more cost-effective for both patients with severe and moderate depression as compared to the threshold, namely, GBP 20 000–30 000/QALY, adopted by NICE or maximum willingness to pay per QALY in Japan of JPY 6.75m [29].
Societal perspective
Successfully treated patients
The difference in the total costs between the two strategies was –JPY 693 858, whereas the difference in effectiveness was 0.15. Hence, the ICERs per successfully treated patient became negative, suggesting that COMBI is the dominant strategy over AD.
QALYs
The ICERs per QALY gained were negative both in patients with severe depression and in those with moderate depression. These results indicate that from the societal perspective, COMBI is highly dominant over AD in terms of both the ICER per successfully treated patient and the QALY. The results of the base value analyses are listed in Table 4.
Base value analyses
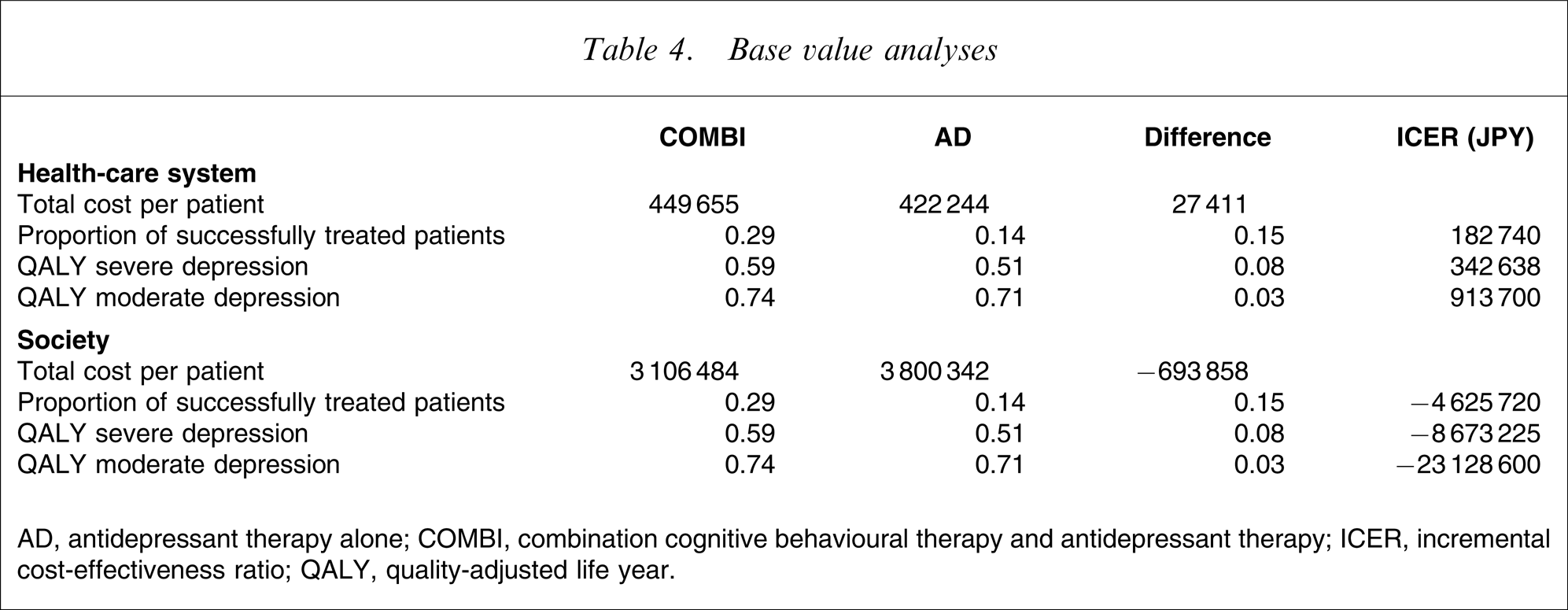
AD, antidepressant therapy alone; COMBI, combination cognitive behavioural therapy and antidepressant therapy; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year.
One-way sensitivity analysis
One-way sensitivity analyses were performed in order to ensure robustness of the results of the base value analyses. The analyses were performed using seven scenarios by changing one parameter over its 95%CI range while keeping the others constant.
Health-care system perspective
The results of the sensitivity analyses showed that the most significant components of the parameters of uncertainty affecting the robustness of the cost-effectiveness between the two treatment strategies were the non-response rate following completion of the initial treatment (scenario 2).
Patients with severe depression
In regard to the response rate to the initial treatment, the ICERs ranged from the negative to JPY 2 211 605 per successfully treated patient and from the negative to JPY 2 821 716 per QALY gained. This result included both negative and relatively high ICERs. The high average costs of the branch after non-response, because it included inpatient treatment, affected the aforementioned results.
With regard to the relapse rate within 9 months, the sample size of the original data was small (n = 44) [20, 21], yielding a broad range of 95%CI. This resulted in the relatively wide ICERs, but, as compared to the threshold ICERs adopted by NICE in England and Wales (GBP 25 000–30 000 per QALY), or maximum willingness to pay per QALY in Japan of JPY 6.75m [29], the higher ICER per QALY was below this threshold, and the treatment still appeared to be cost-effective. The results were less sensitive to the utility parameters as compared to aforementioned ones.
Patients with moderate depression
The results for patients with moderate depression were more complicated. Sensitivity analysis for non-response rate to the initial treatment (scenario 2) showed that the ICER per QALY ranged from the negative to JPY 7 648 345.
Similar to the case in severely depressed patients, the fact that the branch after non-response to initial treatment included costly inpatient treatment produced the high ICERs in scenario 2.
Also, similar to the case in severely depressed patients, the utility parameters had less influence as compared to the aforementioned factors.
Societal perspective
Sensitivity analysis from the societal perspective showed that all ICERs (whether per successfully treated patient or per QALY gained) were negative, meaning that COMBI was always dominant over AD. This implies that the superiority of COMBI was robust when the analysis was conducted from the societal perspective.
The results of the one-way sensitivity analyses from the health-care system perspective are listed in Table 5.
Sensitivity analysis from the health care system perspective
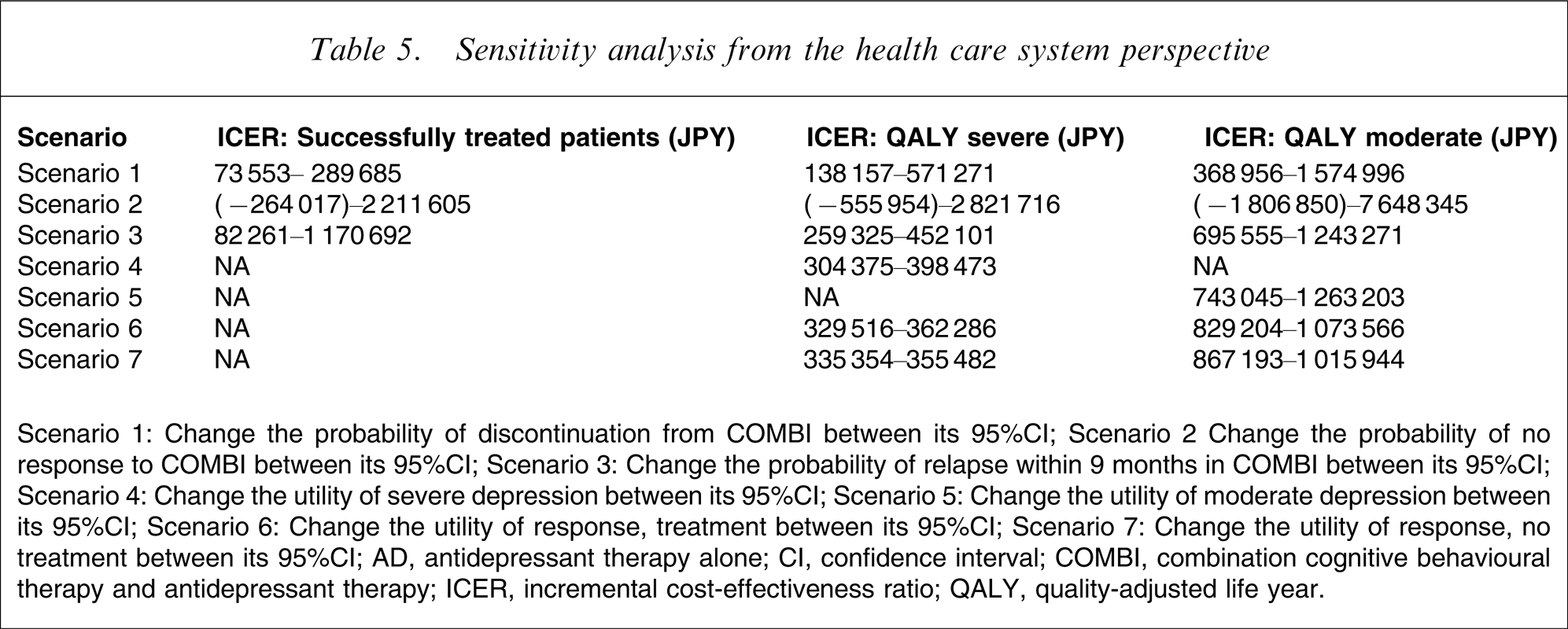
Scenario 1: Change the probability of discontinuation from COMBI between its 95%CI.
Scenario 2 Change the probability of no response to COMBI between its 95%CI.
Scenario 3: Change the probability of relapse within 9 months in COMBI between its 95%CI.
Scenario 4: Change the utility of severe depression between its 95%CI.
Scenario 5: Change the utility of moderate depression between its 95%CI.
Scenario 6: Change the utility of response, treatment between its 95%CI.
Scenario 7: Change the utility of response, no treatment between its 95%CI.
AD, antidepressant therapy alone; CI, confidence interval; COMBI, combination cognitive behavioural therapy and antidepressant therapy; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life year.
Probabilistic sensitivity analysis
The acceptability curves were constructed in order to show the results of probabilistic sensitivity analyses (Figure 2). In the interests of space we demonstrate this procedure only from a health-care system perspective. The curve illustrates the probability of COMBI being cost-effective compared with AD at different values for willingness to pay for an incremental outcome improvement. The results indicated that if the decision maker thinks that JPY 6.75m is an affordable threshold for each additional successfully treated patient, the probability of COMBI being cost-effective against AD would be 99.8%. When evaluated from the QALYs perspective, COMBI would be 94.2% likely to be viewed as cost-effective against AD alone for severe depression and 76.0% for moderate depression, respectively, at maximum willingness to pay per QALY in Japan of JPY 6.75m [29].
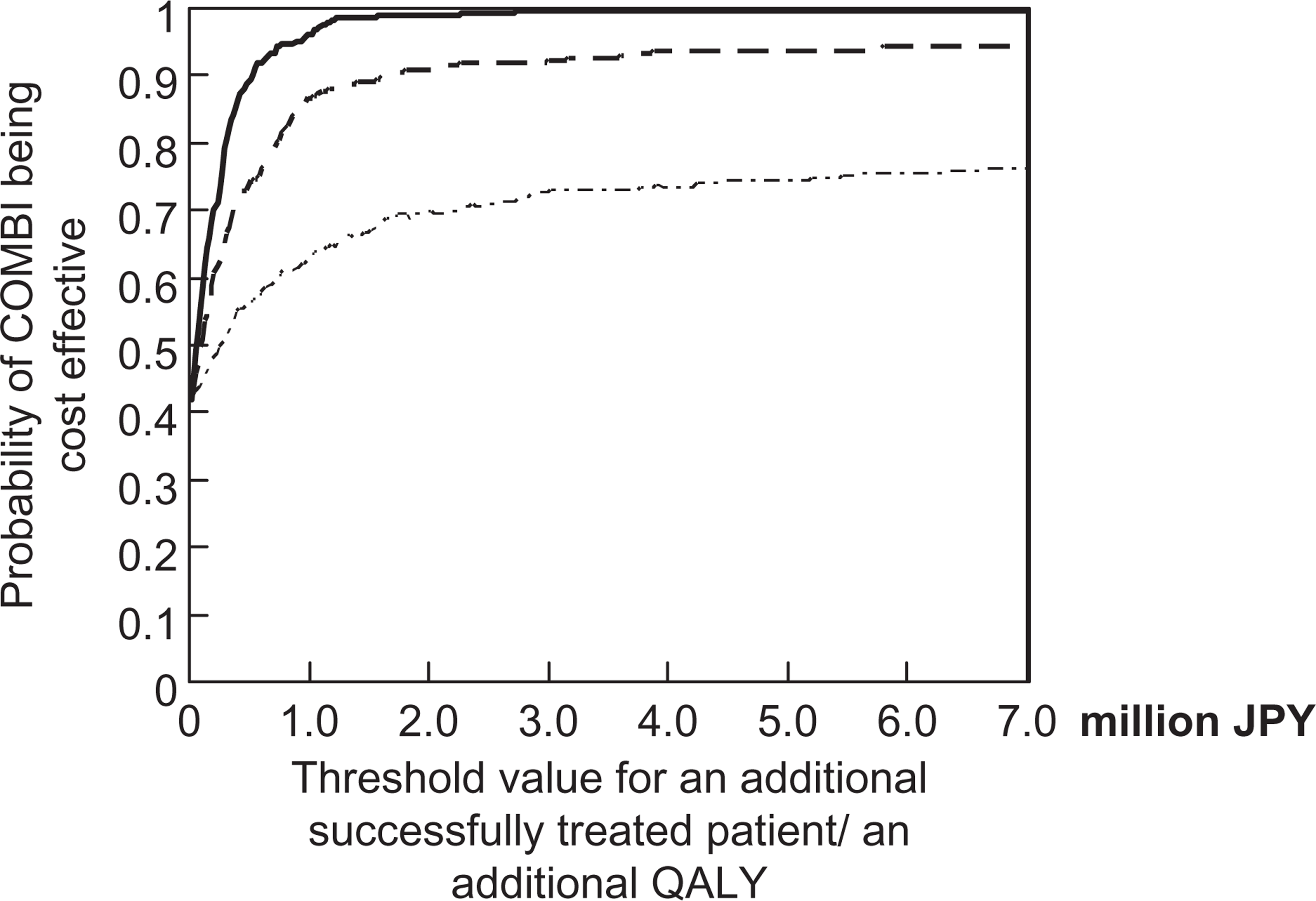
Cost-effectiveness acceptability curve of COMBI vs antidepressant therapy alone. (––), successfully treated; (
Discussion
Study limitations
Clinical parameters
Ideally, cost-effectiveness analysis should be carried out using data based on the country for which the analysis is intended. Search of the literature, however, found few reports of clinical data obtained in the Japanese setting, therefore it was necessary to adopt clinical parameters reported from elsewhere.
Cost data were gathered from unit cost data published by the government and interviews with expert psychiatrists who were familiar with the management of depressed patients. These could be limitations of the study but these disadvantages were not considered to be serious; also the benefits derived from interventions (especially psychotherapy) are expected to be similar in all high-income countries [19].
Cost assessment
We entered productivity loss due to absenteeism from work into the calculation. Still, as Kessler et al. have indicated, productivity loss due to presenteeism is also profound; this refers to the loss caused by patients suffering from symptoms of depression who continue to report to work [30]. Although measurement of the productivity loss due to presenteeism tends to be subjective, inclusion of this cost would be very important to avoid underestimation of the actual impact of this disorder. In addition, the results would become even more reliable if other costs such as those of social care, education, housing, criminal justice and social security were also considered, in order to reflect the whole range of impact of the disease [31].
Study strengths
Regardless of the limitations described in the previous section, this study is unique in several respects, as described in the following.
Comparison between combination therapy and antidepressant therapy
First, this study is unique in attempting to compare COMBI with AD. Although COMBI therapy is a significant alternative to AD, to date few studies have compared the cost-effectiveness between these two arms. Moreover, the model used in the present study took chronic patients into account, and this has not been done in many other studies. Approximately 30% of patients do not go into remission within 24 weeks [32], but in previous patient-level research the clinical course of such chronic patients has not been taken into consideration [18, 19]. In the present study those who did not respond to the initial and even the second antidepressant therapy were also considered. Therefore, this could contribute to improvement of knowledge in this area.
First study in the Japanese setting
The present study is also unique in that this is the first to compare COMBI and AD in the Japanese setting.
Numerous studies have confirmed the effectiveness of COMBI over AD [14, 16–18, 33]. In regard to cost-effectiveness analysis, however, although there are some population-level analyses [32, 34], only two patient-level studies comparing COMBI and AD have been performed [18, 19]. Also, no research has ever been conducted in the Japanese setting. Thus, the present study could provide useful information to resolve relevant problems in Japan.
Analysis from the societal perspective
Another strength of the study is that the analysis was conducted from the societal perspective. In contrast to other major diseases such as cancer or cardiovascular diseases, the impact of mental disorders tends to be underestimated if only the direct costs are evaluated. Thomas and Morris found that the proportion of the direct costs for managing patients with depression was <10% in the UK [4]. Similar results were also confirmed by Greenberg et al. in the USA [5].
These results imply that analysis from the health-care system perspective could fail to reflect the actual impact of the disease.
In the present study the comparison of the results from the health-care system perspective and that from the societal perspective showed that the incremental direct cost for COMBI was completely offset by the reduction of productivity loss. This indicates that it would be worthwhile to invest on the incremental costs for COMBI from the societal perspective.
Political implications
How should the results of the study be interpreted? The first implication is that inclusion of CBT into the health insurance system should be considered.
The present scheme of social health insurance in Japan does not include CBT. Therefore, many patients are not able to undergo CBT due to financial reasons. This situation is critical from the perspective of equity. As the present study indicates, COMBI is highly cost-effective from the health-care system perspective. Furthermore, the incremental costs were shown to be completely offset by the considerable reduction of productivity loss. This implies that COMBI is likely to be efficient as well.
Hence, it would be well worth including COMBI into the health insurance scheme, but the number of therapists who can provide CBT is severely limited in Japan. Therefore, the policy to improve the workforce for CBT is also critical issue as well.
Finally, these results were drawn from modelling-based analyses. Because cost-effectiveness analysis with modelling tends to make varying assumptions and collect the cost data retrospectively, the conclusions are likely to be affected by the quality of the study protocol [35, 36]. Thus, confirmation of the results in an RCT is necessary to validate the present results.
Footnotes
Acknowledgements
This study was in part supported by a grant from Pfizer Health Research Foundation