
Abstract
Over the last 20 years clear evidence has emerged of poorer health among M
M
Patterns of mental health service use by M
Social deprivation is associated with poorer health [11], and higher rates of psychiatric hospitalization, especially for severe and enduring mental illnesses (such as schizophrenia and bipolar disorder) [12–15] both in New Zealand and elsewhere. This study examines the extent to which high rates of common mental disorders among M
Methods
This paper uses data from the MaGPIe study, which is described in detail elsewhere [16].
Setting and sampling
Participants were 70 randomly selected General Practitioners in the lower North Island of New Zealand. General Practice in New Zealand is a partially state-subsidized health system, that is predominantly funded by fee-for-services, financed by a combination of patient payments, tax funding and less frequently, insurance.
Fifty consecutively attending eligible adult patients were recruited from each general practitioner's practice. Stratified sampling identified a primary sample of 1151 patients, of whom 788 were interviewed.
Measures
The measures of mental disorder used were based on the World Health Organization's Collaborative Study of Psychological Problems in General Health Care [17].
Social and material deprivation was assessed in two ways. The first method used the 2001 census Deprivation Index (NZDep). NZDep is a census-based index of deprivation based on the geographical area of residence. NZDep consists of nine age and gender standardized variables that identify a standardized proportion of people with a lack of a defined material or social resource who reside in a small census-based geographical area [18].
An individualized study-specific index of social and material deprivation was also created using similar constructs as NZDep2001, using the general methodology developed for such indicators [19], but using available deprivation data for each participant in the study. Participants were scored 1 for each of the following: if they were unemployed, had no educational qualifications, held a Community Services Card, had no car, or had no telephone. The count of these attributes was then used as the individualized social and material deprivation index.
Ethnicity was determined by self-identification using the Statistics New Zealand question used in the 1996 census [20]. M
Procedures
Ethics approval
This study was approved by the Wellington and Manawatu-Whanganui Ethics Committees.
Recruitment of general practitioners
General practitioners were selected randomly from 299 eligible GPs in two health districts in New Zealand (see [16] for detail).
Recruitment of patients/index consultation
Patients were eligible for screening if they were 18 years old or over, read English well enough to understand and complete the 12 item General Health Questionnaire (GHQ) screening instrument [21], and were about to consult with the general practitioner for their own health concerns.
GHQ score was used to select the primary sample for detailed interviews. The doctor completed an Encounter Form that included an assessment of psychological health for every patient aged 18 or over who was seen that day. For those patients selected and consenting, the general practitioner completed a more detailed Patient Management Questionnaire on the patient's condition/s and treatment/ s implemented.
The patient interview
The patient interview consisted mainly of the Composite International Diagnostic Interview (CIDI) [22], computerized using the World Health Organization's ISHELL software. Patients were interviewed, usually in their own homes, within days of the index consultation.
Data scoring and statistical methods
CIDI v2.1 data were scored using algorithms to produce DSM-IV diagnoses. Statistical analyses were carried out using Statistical Analysis Software (SAS) version 8.2. Data were weighted to adjust for differences in probability of being sampled using the method of Kish [23]. Weighted prevalence estimates were derived using the SAS procedure SURVEYMEANS, which also adjusted confidence intervals for the effects of clustering within general practitioner. Relative Risks were estimated from a generalized regression, accounting for both weighting and clustering [24], using the statistical programme STATA.
Results
Ninety per cent of eligible randomly selected GPs participated, and 70 per cent of eligible patients completed interviews. Of participants, 10.3% were M
Demographic characteristics of general practice attenders by ethnicity
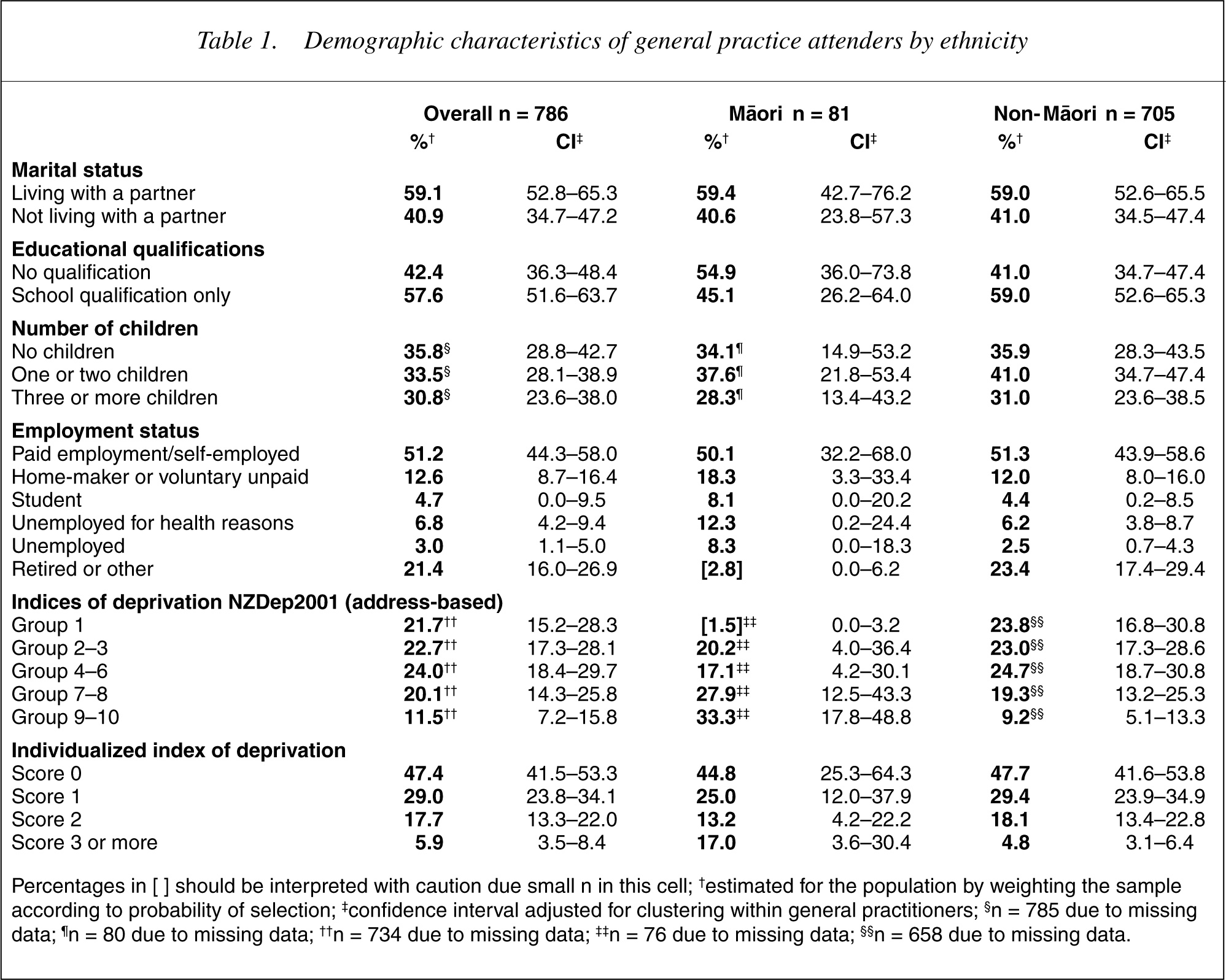
Percentages in [] should be interpreted with caution due small n in this cell; †estimated for the population by weighting the sample according to probability of selection; ‡confidence interval adjusted for clustering within general practitioners; §n = 785 due to missing data; ¶n = 80 due to missing data; † †n = 734 due to missing data; ‡ ‡n = 76 due to missing data; § §n = 658 due to missing data.
Table 2 shows higher rates of disorder among M
Twelve month prevalence of CIDI-DSM-IV mental disorder among general practice attenders by gender and ethnicity
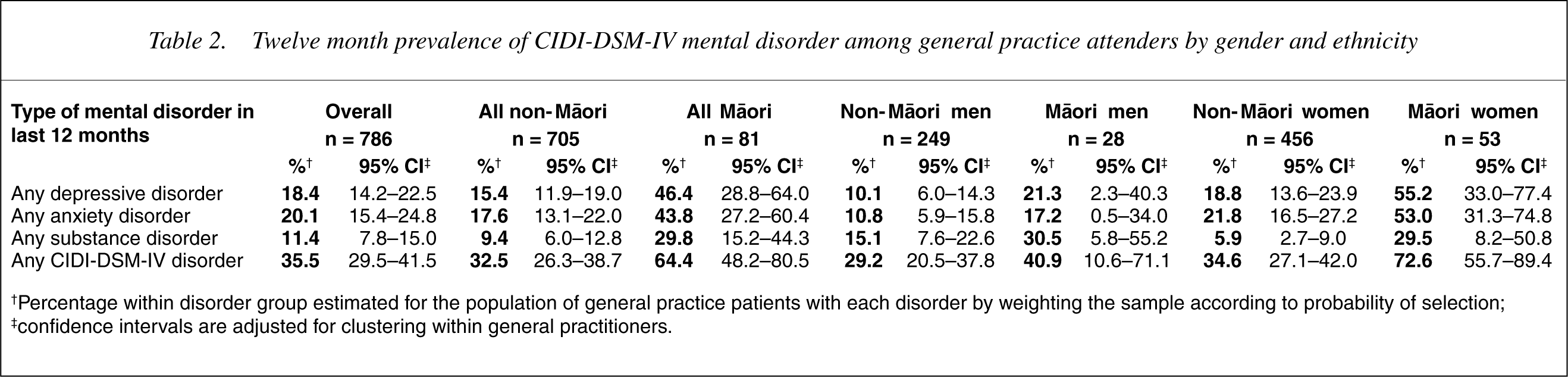
†Percentage within disorder group estimated for the population of general practice patients with each disorder by weighting the sample according to probability of selection; ‡confidence intervals are adjusted for clustering within general practitioners.
Mental disorder and social and material deprivation amongst M
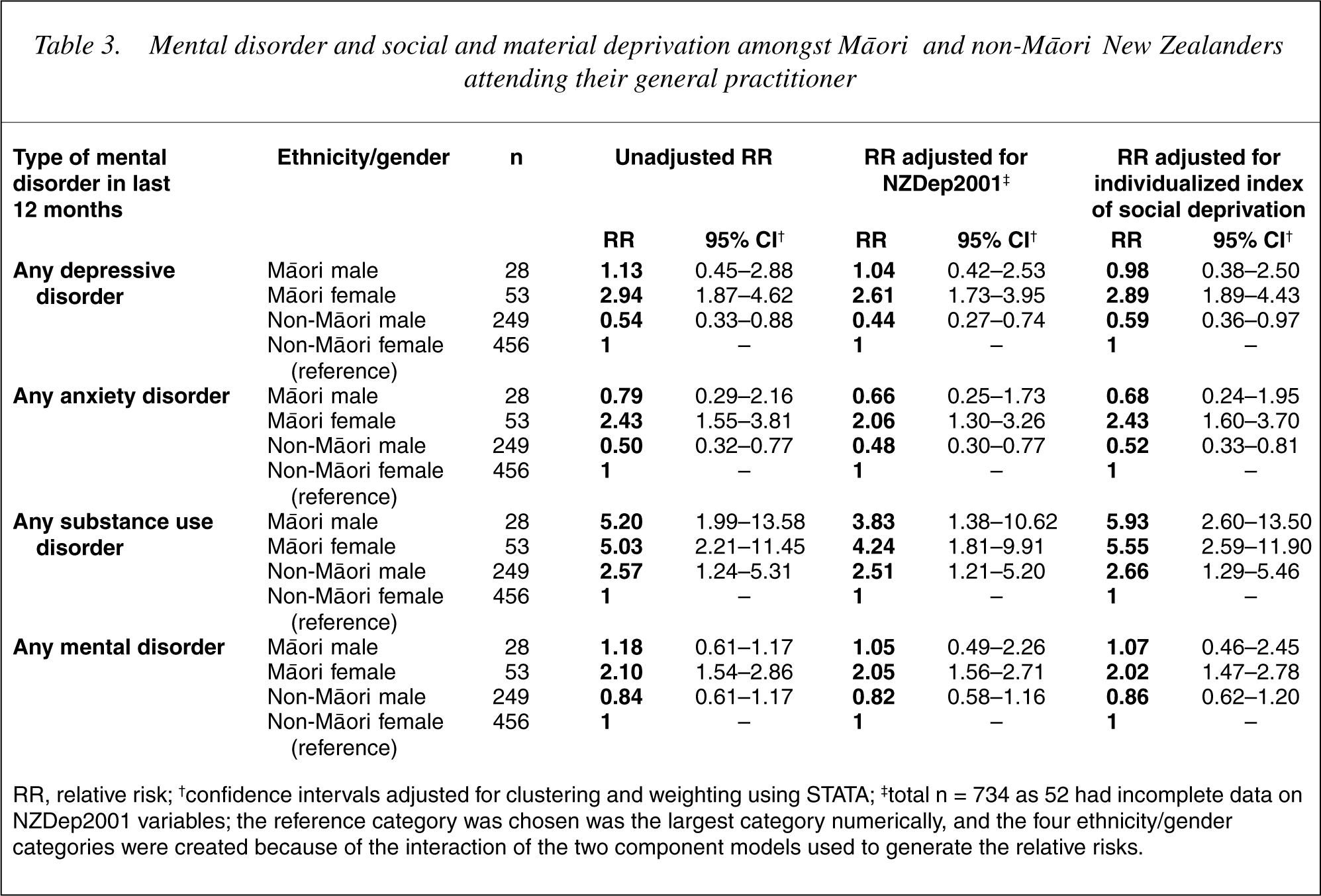
RR, relative risk; †confidence intervals adjusted for clustering and weighting using STATA; ‡total n = 734 as 52 had incomplete data on NZDep2001 variables; the reference category was chosen was the largest category numerically, and the four ethnicity/gender categories were created because of the interaction of the two component models used to generate the relative risks.
Treatment for psychological problems was offered by the GP at similar rates to both M
Discussion
This study of the patients of randomly selected general practitioners is likely to closely represent the experience of typical general practices in New Zealand. The study is limited because of the low, although proportionate, number of M
This study suggests that rates of mental disorder among M
Although rates of mental disorder were higher among M
The higher rates of disorder among M
Currently there is considerable debate in New Zealand about the need for services, remedial interventions or other initiatives that specifically target M
Footnotes
Acknowledgements
We are grateful to Mason Durie and Joanne Baxter for reviewing a draft of this paper. We would like to thank the participating general practitioners and other practice staff, the patients who participated, and our research staff. The Health Research Council of New Zealand funded the project (grant 99/065), with supplementary funds also contributed by the Alcohol Advisory Council (ALAC).