
Abstract
Keywords
Aggressive behaviour, non-compliance and rulebreaking are common during childhood and cause significant impairment [1]. More importantly, they are strongly associated with mental disorders and use of mental health services in adulthood [2]. There has been much progress in the understanding of these problems but experts agree that the classification of externalizing disorders is still unsatisfactory and there is a need to refine these constructs further [e.g. 1,3,4]. Moreover, rates, associations with age and gender, correlates, and comorbidity vary considerably among studies [5]. Categorical and dimensional approaches are used to classify these problems and the advantages and shortcomings of each have been highlighted [6–8]. Some studies have reported differences between aggressive and delinquent syndromes [9–11]. The aggressive syndrome comprises behaviours like destroying objects, bullying, fighting and vandalism, while stealing, lying and truancy are characteristic of the delinquent syndrome. There is growing evidence of a strong relationship between aggression in childhood and violent behaviour in adolescence [e.g. 12]. However, given the frequent co-occurrence of these behaviours, they have rarely been considered in their pure and combined forms.
These syndromes were examined in an unselected community sample of children and adolescents. The survey employed the Child Behaviour Checklist (CBCL) [13] to identify childhood mental health problems and structured diagnostic interviews to identify DSM-IV defined mental disorders [14]. In addition to global problem scores, the CBCL offers more detailed assessment in terms of eight empirically derived syndromes. Two of the syndromes are called delinquent (or rulebreaking) and aggressive. The former consists of items such as stealing, truancy, running away and use of alcohol or drugs. The latter includes behaviours like arguing, destroying objects, fighting, screaming, and temper tantrums. The empirically derived CBCL syndromes have good reliability, high cross-cultural consistency and can be obtained easily and at low cost [13], [15].
The primary aim was to ascertain whether there were differences in the correlates, comorbidity and use of services between children rated by parents as showing high levels of aggressive behaviour, high levels of delinquent behaviour, and those with high levels of both problems. The existence of differences would support the validity and usefulness of these syndromes. A second aim was to ascertain their overlap with DSM-IV diagnoses of conduct disorder, depression and the subtypes of attention deficit hyperactivity disorder (ADHD). Although the association between aggression and delinquency with ADHD is well established, little is known about whether associations vary according to ADHD subtypes.
Method
Design
Ethics approval was given by the Research Ethics Committee at the Women's and Children's Hospital, Adelaide. The survey method has been described elsewhere in detail [16]. In summary, multistage probability sampling of households with children younger than 18 years was used to obtain a representative sample of 4509 residents aged 4–17 years. There were no differences in the demographic characteristics of children, parents and families who participated and those of the population from which they were selected based on the 1996 Australian census, with the exception of age. Children aged 4 and 5 years were slightly over-sampled while those aged 16 and 17 years were slightly under-sampled. Age and gender distribution of participants as well as prevalence and correlates of disorder have been published elsewhere [17]. Unless otherwise specified, the word ‘children’ is used to design people younger than 18 years.
Instruments
Parents or main caregivers (henceforth described as ‘parent/s’) completed the CBCL [13] and a questionnaire asking about children's demographic characteristics and their use of services during the previous 6 months to obtain help for emotional and behavioural problems. Parents were also interviewed using the parent version of the Diagnostic Interview Schedule for Children Version IV (DISC-IV) [14]. All these instruments have been shown to have acceptable psychometric properties [13], [14].
Measures
Measures of children's aggressive and delinquent behaviour were derived from ratings on the parent-completed CBCL. Children who had scores in the top 5% in the aggressive scale (a score of 18 or above) were assigned to the ‘aggressive group’. Similarly, children who had scores in the top 5% in the delinquent scale (a score of 6 or higher) were assigned to the ‘delinquent group’. Children who scored in the top 5% on both scales were assigned to the ‘combined group’. The cut-off of 5% was selected because it broadly coincides with the cut-off score for clinical caseness on normative US data [13].
The DISC-IV [14] administered to parents was used to diagnose depression (including major depression and dysthymia – very few cases qualified for dysthymia) (n = 131, 3.7%), ADHD (inattentive, n = 165, 5.1%; impulsive-hyperactive, n = 53, 1.6%; combined, n = 103, 3.2%) and conduct disorder (n = 97, 3%). ADHD was diagnosed if there were symptoms and impairment in past year. No other diagnoses were considered in the survey. The DISC-IV was not administered to parents of 4 and 5 years old children; hence diagnoses were not available for this age group.
For the purpose of analyses, the following categories were created for the demographic variables (coded as yes = 1, no = 0):
Metropolitan residence (n = 2508, 61%).
Low income family (less than 480 Australian dollars per week, n = 625, 20%).
Family type, categorized as original two-parent (n = 3097, 76%), step-blended (n = 331, 8%) sole parent (n = 574, 14%) and other (n = 72, 2%). The ‘other’ group represented foster-care and other family arrangements. Due to the small number and the variety of family circumstance lumped together; the ‘other’ group was not included in analysis.
Parental education, whether father (n = 949, 29%) or mother (n = 1100, 28%) had left school before age 16.
Parental unemployment, whether neither parent was working full or part-time (n = 817, 22%). 368 AGGRESSIVE AND DELINQUENT CHILDREN
Use of services: school services (n = 171, 4%); GP or paediatrician (n = 156, 4%); mental health services (n = 125, 3%); medication (n = 83, 2%).
Parental perception that the child has significant emotional or behavioural problems and is in need of professional help (n = 366, 9%).
Statistical analysis
Alpha was set at 0.05. Variables describing demographic characteristics and service use were dichotomous or dichotomised for analysis and were examined using χ2. An initial analysis was performed according to whether participants were in the top 5% in the aggressive and delinquent scales, none or both. To identify relationships between group membership and demographic and other variables, three hierarchical multiple logistic regression models were fitted to the data. Whether children were in the aggressive or delinquent group or qualified for DISC-IV conduct disorder were the dependent variables. Predictor variables were those listed in Table 1, with the exception of metropolitan residence, which did not differ between the groups. Subsequently, variables not associated with any of the dependent variables were excluded and new logistic regressions performed; these results are reported in Table 2.
Participants in the aggressive and delinquent groups according to demographic variables, comorbid diagnosis and service use (percentages)
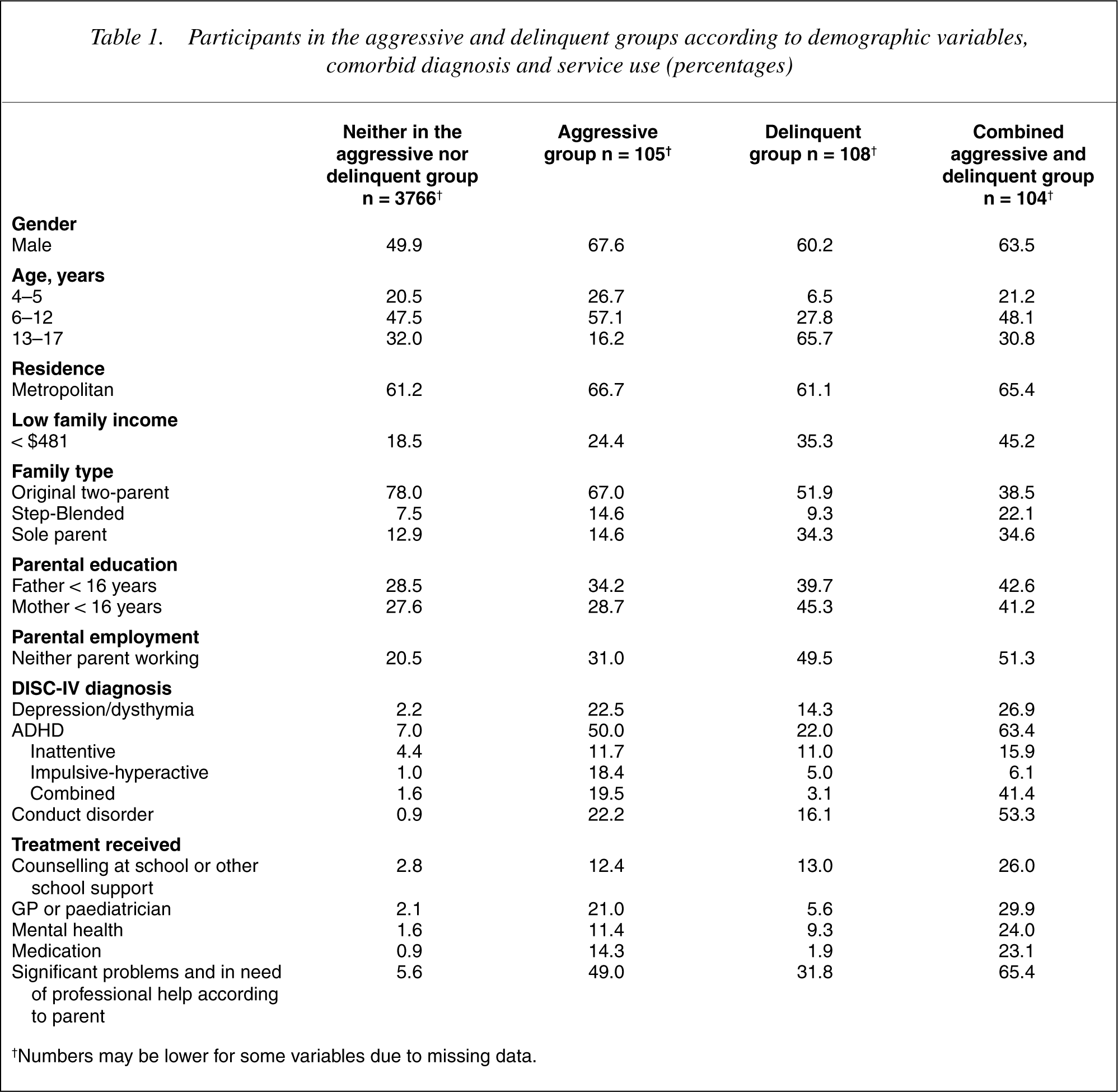
†Numbers may be lower for some variables due to missing data.
Variables associated with having scores in the top 5% in the delinquent scale, aggressive scale and with DISC-IV conduct disorder (OR, Odds Ratio; C.I., confidence interval. Boldface represents a significant association)
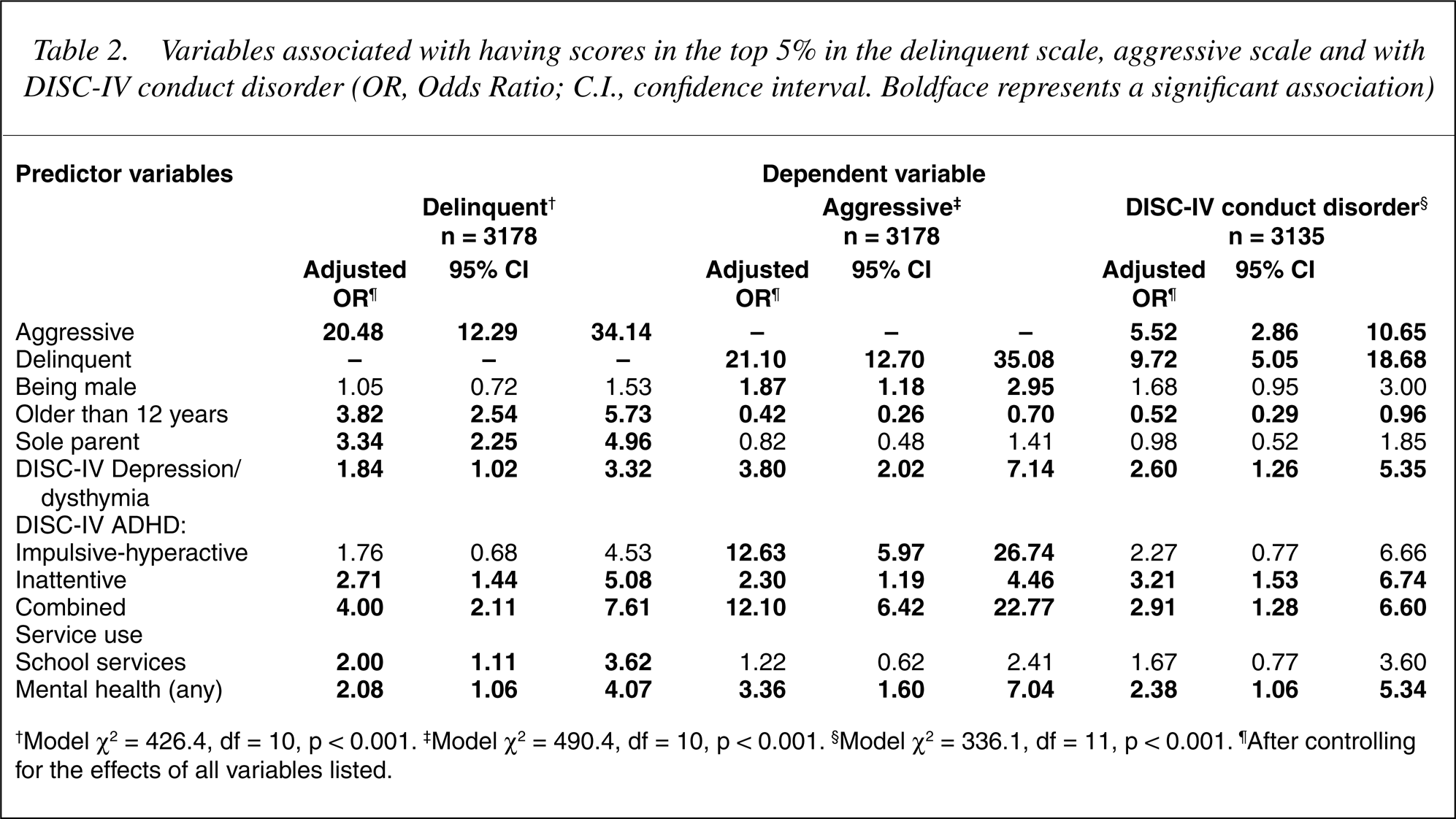
†Model χ2 = 426.4, df = 10, p < 0.001. ‡Model χ2 = 490.4, df = 10, p < 0.001. §Model χ2 = 336.1, df = 11, p < 0.001. ¶After controlling for the effects of all variables listed.
There was substantial data missing in some analyses. This was largely due to parents not answering all items in questionnaires. Lower response rates were large in the questions about income (n = 1356, 30%) and parental educational level (n = 1250, 28%). Analysis using the aggressive and delinquent syndromes, age and gender had fewer missing cases (n = 426, 9%). Because multivariate analysis included DISC-IV diagnosis, which were not obtained for children aged 4 and 5 years (n = 912, 20%), multivariate analyses refer only to participants aged 6–17 years.
Results
Of the 4083 participants who had data, 317 (7.8%) had high scores on these CBCL scales (2.6% aggressive only, 2.6% delinquent only, 2.5% both). Approximately half of the children with high scores on one scale also scored on the other, indicating considerable overlap/ comorbidity.
Table 1 summarizes the findings describing children in the aggressive, delinquent, and combined groups, along with those who were not assigned to any of these groups. There were statistically significant differences between the groups for all the variables with the exception of metropolitan residence. Differences usually followed a dose– response pattern with children in the neither group showing the lowest rate of negative characteristics, children in the combined group the highest and those in the aggressive and delinquent groups somewhere in between.
Figure 1 shows changes in the proportion of children in each group according to age. These can be summarized as follows:
Percent of participants in the aggressive, delinquent and combined groups according to age.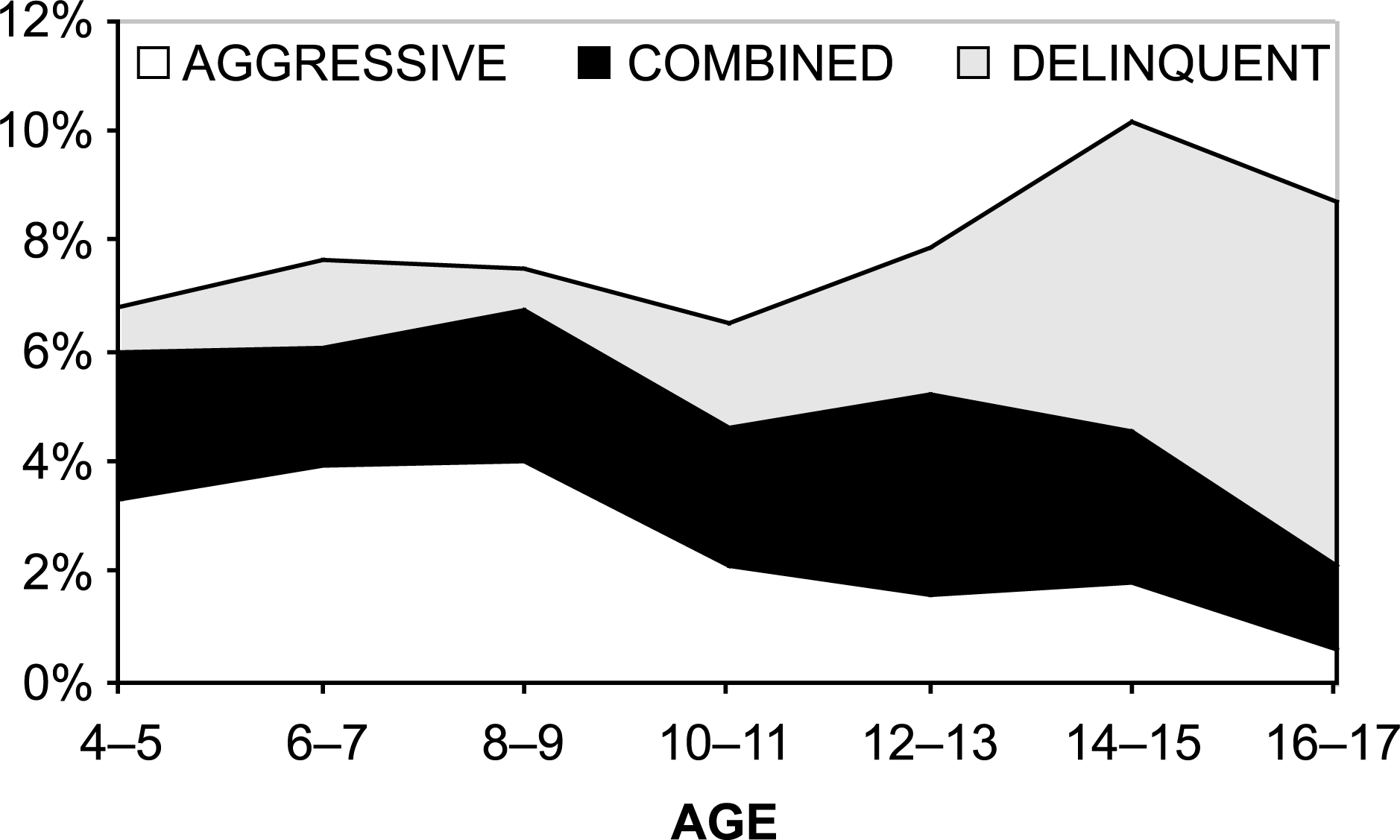
Overall the proportion of children who were assigned to any of the three groups was quite constant from 4 to 17 years (average 7.8%). Differences were not statistically significant overall and for boys and girls separately.
There was a gradual decrease in the proportion of children in the aggressive group with increasing age, the contrary occurred for the delinquent group. The proportion with both (combined) remained constant.
The rate in the aggressive and delinquent group was fairly constant between the ages of 4 and 9 years but there was a gradual decrease in the proportion of children in the aggressive group after the age of 9 years. The contrary occurred for the delinquent group (Table 1).
The results of the multivariate analysis (the dependent variable represents membership of that group versus all others) are summarized in Table 2. Only those predictors associated with at least one of the dependent variables are reported. Examination of the odds ratios shows similarities and differences in the pattern of associations. The strongest predictor of being in either the aggressive or delinquent group was membership of the alternative of these two groups. For example, children in the aggressive group were about 20 times more likely to also be in the delinquent group and vice-versa. Children in both groups were more likely to meet criteria for DISC-IV conduct disorder, those in the delinquent group twice as often as those in the aggressive group.
Male sex was associated with being in the aggressive but not with the delinquent group or DISC-IV conduct disorder group (Table 2). Although participants in the delinquent group were 1.6 times as likely to be males (95% CI = 1.2, 2.1), this association became nonsignificant when the gender association with aggressive behaviour was controlled statistically. For example, among aggressive females 53% were also in the delinquent group compared with 48% of males. This was similar for DISC-IV conduct disorder, but due to the association of male gender with ADHD combined subtype. Being older than 12 years was positively associated with the delinquent and negatively associated with the aggressive group and with DISC-IV conduct disorder. Living in a sole parent family was specifically associated with the delinquent group.
Service use and perceived need for professional help
Children in the three groups used mental health services more often but only those in the delinquent group used school services more often (Table 2). Parents believed that children in the aggressive, delinquent and conduct disorder groups needed professional help more often than those without these behaviours, even after taking into account the effect of confounding variables. This was particularly so for those in the aggressive group (adjusted OR = 9.40; 95% CI 5.60, 15.90), compared with the delinquent group (adjusted OR = 2.76; 95% CI 1.67, 4.58) and the conduct disorder group (adjusted OR = 1.97; 95% CI 1.01, 3.82).
Association with other disorders
This is also shown in Table 2. DISC-IV conduct disorder varied according to age; it was twice as common among 6–12 years olds as among 13–17 years olds. The combined and inattentive subtypes of ADHD were positively associated with the aggressive, delinquent and conduct disorder groups. However, the impulsive/hyperactive subtype was specifically associated with the aggressive group. Overall, comorbidity with ADHD was lower among aggressive and delinquent adolescents, with the exception of the predominantly inattentive subtype, in which comorbidity was higher. ADHD inattentive was about four times more prevalent among 13–17 years olds than in 6–12 years olds (12.2% versus 38.0%, χ2 = 14.5, df = 1, p < 0.001).
Comorbidity with depression was higher among adolescents in all groups, ranging from 11% in 6 to 12 years olds in the delinquent group to 36% among adolescents in the combined group. After controlling for the effect of gender and age, comorbidity with depression was similar across the groups.
Discussion
Both aggressive and delinquent youths used services more often, but parents perceived aggressive children as more in need of help than delinquent ones. Living in a sole parent family was specifically associated with the delinquent group, while the aggressive group was specifically associated with the impulsive-hyperactive subtype of ADHD. Also, comorbidity between ADHD and antisocial behaviour decreased when children were older with the exception of the inattentive subtype in which comorbidity was higher among adolescents. This highlights the existence of differences in the pattern of comorbidity between aggression, delinquency, and the various subtypes of ADHD. This differential association requires further examination and may help to understand better the nature of conduct disorder and of the subtypes of ADHD.
The importance of comorbid hyperactivity in the maintenance of antisocial behaviour has been emphasized [18], [19]. However, recent data suggest that aggressive delinquency in adolescents is largely the outcome of being aggressive in earlier years and not of ADHD as postulated in many studies [12]. The delinquent group did not show gender differences while the aggressive group was predominantly male. Other studies [e.g. 20] have reported no gender differences in nonaggressive conduct disorders also. This suggests that the male predominance among conduct disordered children is largely the result of aggressive children being mostly male.
Prevalence of aggressive and antisocial behaviour in this community sample remained quite constant from 4 to 17 years (at around 8%). This was due to a decrease in the proportion of children in the aggressive group with increasing age, which was compensated by an increase in the delinquent group (11], [21] and with the DSM-IV criterion of using 10 years of age as the threshold for diagnosis of conduct disorder of adolescent onset [22]. By contrast, a recent report [12] using data from six long-term prospective studies in three countries found that a small group of children exhibited notably more physically aggressive behaviour than their peers throughout. In these children, high levels of physical aggression were quite stable from childhood to adolescence. In particular, this and another study [23] did not show changes in antisocial behaviour consistent with an adolescent-onset group. However, they focused on aggressive behaviour and did not examine property (e.g. stealing) or status violations (e.g. truancy), which are rare before the age of 10 years [21].
The proportion of children in the combined aggressive and delinquent group was relatively constant throughout (between 2% and 3%). These children may be similar to the persistently physically aggressive participants identified in the long term prospective studies quoted [12]. In our survey this group was strongly associated with a DISC-IV diagnosis of conduct disorder (53% met criteria for conduct disorder, Table 1).
Prevalence of a DISC-IV diagnosis of conduct disorder in this study decreased with increasing age, contrary to most reports which show that conduct problems increase with increasing age [e.g. 21,24]. This may have several explanations. Firstly, diagnoses in this study are based on parent reports and parents may be unaware of their adolescent children's conduct problems [21]. Secondly, it may be an instrument-specific difficulty. That is, DISC-IV may give undue weight to aggressive, noncompliant symptoms in younger children resulting in over diagnosis of conduct disorder in the younger age group. Thirdly, the operationalization of the conduct disorder construct in DSM-IV (which includes aggressive symptoms, property violations and status violations) may have poor validity. In this regard, at least two studies have found that apart from oppositionality, DSM-IV conduct disorder symptoms have three distinct clusters: aggression, property violations (e.g. stealing) and status offences (e.g. truancy, running away) [25], [26], which have different age and gender associations [21].
Prospective studies [e.g. 12] suggest that children's tendencies to engage in early disruptive behaviours influence later delinquency, with different patterns of behaviour problems being associated with somewhat different delinquent outcomes. However, early physical aggression, in spite of decreasing as children grow older, is the most consistent predictor of both violent and nonviolent offending in adolescence. From the public health and clinical perspectives, these findings emphasize the importance of reducing social disadvantage (e.g. by providing better support to sole parents) and of treating early aggressive and non-compliant behaviour. Among others, parenting programs have been shown to be costeffective interventions in this regard [27].
While sharing many features, the results suggest that these empirically derived syndromes differ in important ways that need to be understood better if more effective prevention and treatment strategies are to be developed. There is a need to enhance convergence between empirically derived syndromes, which are reliable and easy to obtain, and clinical diagnosis. This should be a priority for DSM-V if we want to advance the understanding of these important conditions.
This study has some limitations which must be kept in mind when interpreting the results. The main one is that it is cross-sectional and does not provide information about behaviour changes over time. Other limitations are that group selection was based on parent reports alone and that other conditions, particularly anxiety and learning disorders were not assessed. The presence of comorbid anxiety disorders may have influenced the use of services.
Footnotes
Acknowledgements
We thank T.M. Achenbach for his comments to an earlier version of this paper.