
Abstract
Attention-deficit–hyperactivity disorder (ADHD) is one of the common childhood neuropsychiatric disorders worldwide, with a DSM-IV [1] ADHD prevalence in the range of 5–10% in Western countries [2] and 7.5% in Taiwan [3], and a 5.29% worldwide-pooled prevalence [4], with a ratio of boys to girls of 3–8:1. The clinical and scientific significance of ADHD are not only in its high prevalence, but also in its high psychiatric comorbidity [5], and impairment of attention and executive functions [6], academic performance [7], and social adjustment [1], [8]. Individuals with ADHD have neuropsychological deficits, corresponding to the frontal cortical regions and interconnected subcortical structures [9], which are related to impulsivity, distractibility, and hyperactivity [10].
DSM-IV ADHD consists of three subtypes: predominantly inattentive (ADHD-I), predominantly hyperactive–impulsive (ADHD-HI), and a combined subtype (ADHD-C) [1]. Studies have indicated that the DSM-IV ADHD subtypes differ significantly in variables such as age of onset, gender ratio, and level of social and academic impairment [11], [12]. Despite the importance of neuropsychological validation of the ADHD subtypes [13], little has been addressed on this topic.
Recent studies of neuropsychological functioning on ADHD subtypes were conducted only in Western countries and have demonstrated inconsistent results [14]. Some reported differences between ADHD-C and ADHD-I in various cognitive tasks (e.g. Cancellation Test, Trail-Making Test (TMT), and Wisconsin Card Sorting Test (WCST)) that support neuroanatomical evidence, in variability using time reproduction tasks [15], and in commission errors using the Continuous Performance Test (CPT) [16]. But others did not find these differences using the Tower of London, Stroop Task, and WCST [17], [18]. The inconsistent findings call for in-depth investigation of this topic in different ADHD populations [19]. Although studies on ADHD prevalence and treatment effects have demonstrated similar results to Western studies [3], [20], addressing the differences between ADHD subtypes using neuropsychological assessment under a theoretical attentional framework has not yet been conducted in an ethnic Chinese population.
To our knowledge most studies have focused on the neuropsychological differences between ADHD-C and ADHD-I [21], [22]; only three studies included ADHD-HI samples in neuropsychologically discriminating ADHD subtypes [19], [23], and these offered limited evidence for differentiating ADHD-HI from ADHD-C and ADHD-I. But findings of substantial differences between ADHD-C and ADHD-I have suggested that they may best be characterized as distinct disorders [21]. Therefore, the current study focused on the neuropsychological discernment between these two subtypes.
An empirically derived neuropsychological model of attention delineated by Cohen et al. [24] offers a comprehensive theoretical framework for the component process of attention and proposes an organized set of associated neuropsychological tests for each component [25]. The Cohen et al. model encompasses four attention components: sensory selection, response selection, capacity/focus, and sustained attention [24]. Sensory selection refers to the discrimination of noise from actual information that permits further cognitive processing [26]. Response selection refers to active selection and inhibition of inappropriate responses during goal-directed activities [27]. Attentional capacity is determined by both attentional energetic and structural factors [28]. Sustained attention refers to the maintenance of attention over time, regardless of event probability [29]. Using the Cohen et al. attention model, Lockwood et al. reported significant differences in sensory selection and response selection components but no difference in capacity/focus and sustained attention components between ADHD-C and ADHD-I [30]. The Cohen et al. model offers a comprehensive theoretical framework for the attention process and proposes an organized set of associated neuropsychological tests for each component [24]. Despite lack of difference in the sustained attention component, Cohen et al. have suggested including CPT to assess sustained attention [24].
Due to inconsistent findings in neuropsychological functioning between ADHD subtypes and the lack of studies on neuropsychological functioning of children with ADHD in non-Western countries, we conducted the present study to test the following two hypotheses: (i) that children with ADHD perform worse on all neuropsychological tests; and (ii) that two ADHD subtypes have different neuropsychological portraits according to the Cohen et al. attention model, with better performance in children with ADHD-I than in those with ADHD-C on the four proposed attentional components.
Methods
Participants
Samples included 69 children with DSM-IV ADHD (17 ADHD-I and 52 ADHD-C) and 52 normal controls, grades 2–4, aged 7–10. Patients with a clinical diagnosis of DSM-IV ADHD were recruited consecutively from the Children's Mental Health Centre, National Taiwan University Hospital. Children with neuropsychological symptoms (e.g. brain injury, motor disorder, or epilepsy), visual/auditory deficit, mental retardation, pervasive developmental disorder, and any psychiatric disorders were excluded during the referring process to obtain a homogenous group with ADHD only. Normal controls were recruited from the local elementary school in the same geographical area. Controls were recruited based on the distribution of gender, age, and schools of the ADHD-C group suggested by the teachers, who recognized these controls as having the same performance as children with ADHD if the latter could concentrate on school work. Table 1 summarizes the demographic data for the two ADHD groups and control groups. The full-scale intelligence scores (FSIQ) of the participants ranged from 87 to 133. The ADHD group had significantly lower estimated FSIQ (p < 0.0001) and mother's educational level (p = 0.005) than the school controls. There was no group difference in age, sex, height, bodyweight, parental employment, or household status. The majority of children with ADHD (92.8%) were currently under medical treatment with immediate-release methylphenidate (IR-MPH), with an average daily dose of 23.65 mg.
Demographics and medication history
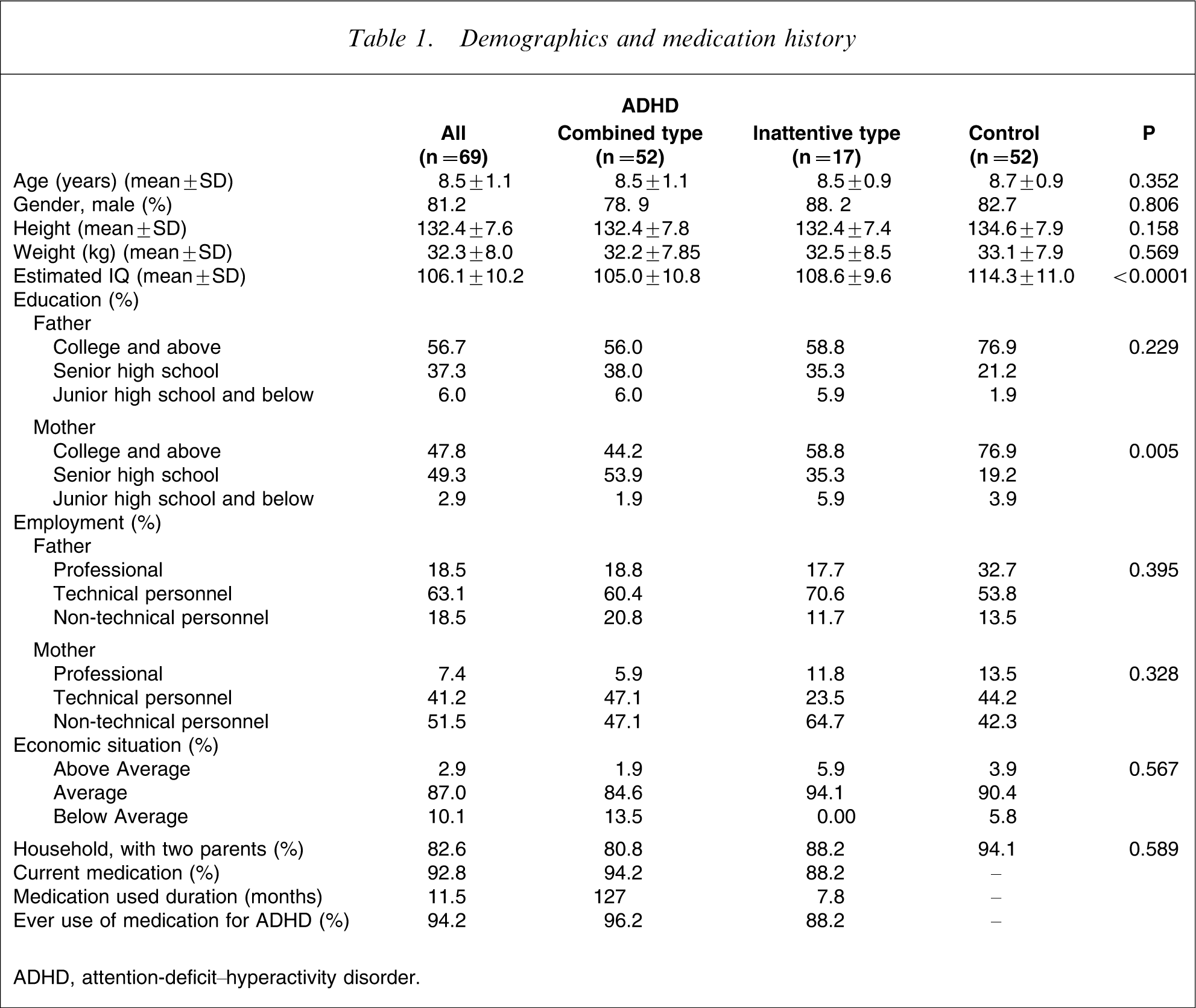
ADHD, attention-deficit–hyperactivity disorder.
Measures
Investigator-administered assessments
Chinese version of the Kiddie-Schedule for Affective Disorders and Schizophrenia–epidemiology version (K-SADS-E)
The Kiddie-Schedule for Affective Disorders and Schizophrenia–epidemiology version (K-SADS-E) is a semi-structured clinical interview for the systematic assessment of both past and current episodes of mental disorders in children and adolescents. Development of the Chinese version of the K-SADS-E was carried out by the Child Psychiatry Research Group in Taiwan [31], followed by modification for DSM-IV diagnosis [3]. The Chinese K-SADS-E has been extensively used in epidemiological studies in Taiwan [3], [31].
Clinical Global Impression–ADHD-Severity
The Clinical Global Impression–ADHD-Severity (CGI-ADHD-S), a single-item assessment of the global severity of ADHD symptoms in relation to the clinician's total experience with other ADHD patients, is rated on a 7-point scale, from 1 for ‘normal, not at all ill’ to 7 for ‘most extremely ill’.
Behaviour Observation Ratings
A three-item rating scale assessed the children's behaviours during the task including ‘fidgeting while being seated’, ‘murmuring during the task’, and ‘giving up easily’. Items were rated on a 4-point scale (0, not at all; 1, a little bit; 2, quite a bit; 3, very much) by MC Chiang, who conducted the neuropsychological tasks.
Parental self-administered assessments
Chinese version of the Swanson, Nolan, and Pelham, version IV scale
The Swanson, Nolan, and Pelham, version IV scale (SNAP-IV), a 26-item instrument using a 4-point scale (from 0, not at all; to 3, very much), uses the core symptoms defined in DSM-IV [1], [32]. The SNAP-IV consists of Inattention, Hyperactivity/Impulsivity and Oppositional subscales (items 1–9,10–18,19–26, respectively). The norm and psychometric properties of the Chinese version of the SNAP-IV (SNAP-IV-C) have been established in Taiwanese populations [33]. In addition to the mean score of each subscale, we also calculated the t-score based on the norm established in Taiwan [33].
Neuropsychological tests
Wechsler Intelligence Scale for Children
The Wechsler Intelligence Scale for Children (WISC) [34] is a well-established scale designed to assess the FSIQ of children aged 6–16. Thirteen subtests are grouped into two scores: the performance intelligence quotient (PIQ) score and the verbal IQ score (VIQ) with a mean of 100 and an SD of 15. The FSIQ of each subject was controlled in the statistical model.
Digit Span
The Digit Span, one of the subtests of the WISC-III, first requires repetition of orally presented digit strings (digit forward) and then requires recall of digits in a backward sequence (digit backward), which were used to represent the index of sensory selection and capacity/focus components, respectively.
Cancellation Test
The Cancellation Test is a two-part paper-and-pencil measure of visual scanning [35]. Number Cancellation requires the striking of a three-digit target (2, 5, and 7) intermittently placed in a large array of numbers; Shape Cancellation requires the striking of a target shape (star) intermittently placed in a file of other shapes. The total number of commission errors and time divided by correct hits were recorded for measuring response selection and sustained attention, respectively.
Trail-Making Test
This is a brief paper-and-pencil test involving numeric sequencing (TMT-A) followed by alphanumeric sequencing (TMT-B) in the original form [36]. The TMT-B was modified by using Chinese phonic symbols to replace the English alphabet [37]. Completed time and off-target errors on the tasks were oriented to the attentional components of sensory selection, response selection, and capacity/focus.
Behavioural symptoms rated by the parents and trained observers
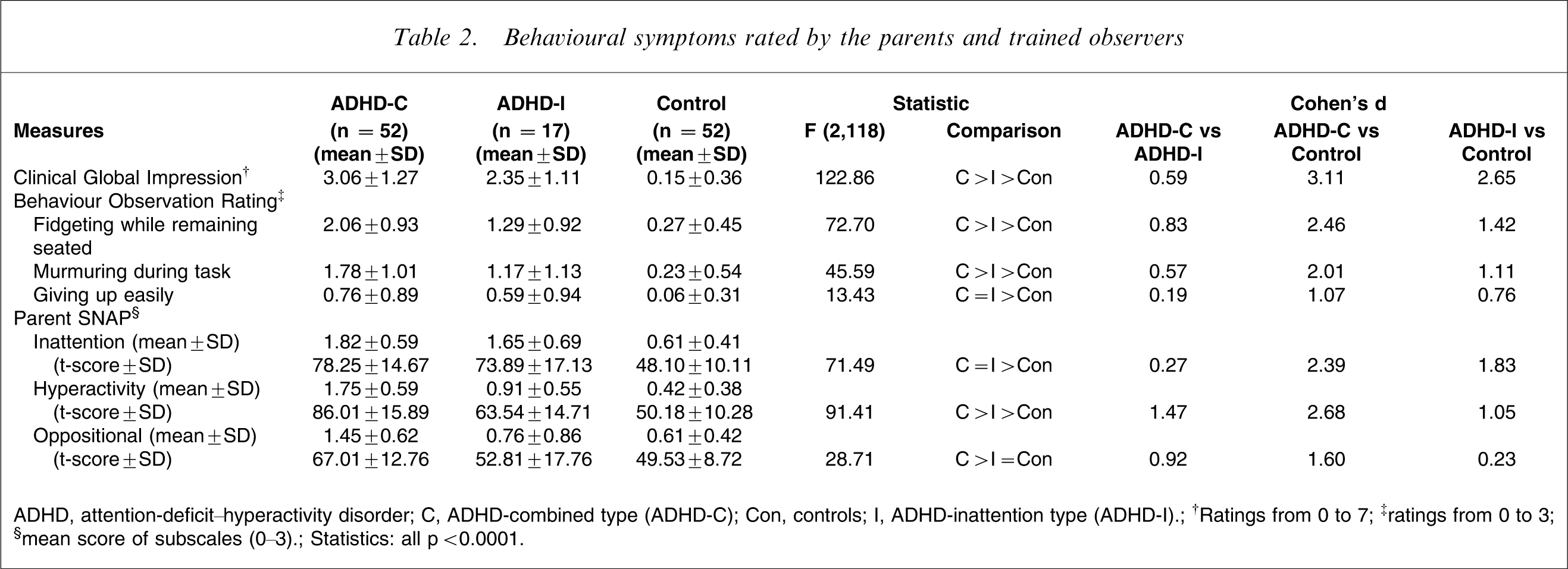
ADHD, attention-deficit–hyperactivity disorder; C, ADHD-combined type (ADHD-C); Con, controls; I, ADHD-inattention type (ADHD-I).
†Ratings from 0 to 7; ‡ratings from 0 to 3; §mean score of subscales (0–3).
Statistics: all p < 0.0001.
Continuous Performance Test
The CPT is a computerized task that requires pressing of the space key when any character besides X is shown on the screen [38]. There were in total six sets with 20 characters within each set. The Inter-Stimulus Intervals (ISIs) are 1, 2, and 4 s, and different ISIs vary between sets. Each character is maintained on the screen for 250 ms. Discriminative factor (d’), measuring the individual's ability to discriminate between targets and non-targets, was included in the sensory selection component. Reaction time, the mean response time (ms) for all target responses, was included in the response selection component. Commission errors, the number of times the individual responded to a non-target, were included in the capacity/focus component. The slope of changes in reaction time presented by Hit Reaction Time Block Change (HiRT) and Hit Standard Error Block Change (HiSE) are both vigilance measures that represent the sustained attention component. A positive slope indicates an inconsistent reaction time as time progresses, suggesting a possible loss of vigilance.
Circle-Tracing Test
The Circle-Tracing Test CTT) is a task that requires subjects, aged ≥6, to trace a large printed circle (50.8 cm; 20 in) with their index fingers, and is used to measure inhibition of an ongoing response [39]. The Chinese character ‘START’ (in green) and ‘STOP’ (in red) were printed to indicate the starting and finishing points of the circle, respectively. The task is administered first by neutral instruction (‘trace the circle’) followed by inhibition instruction (‘trace the circle again, but as slowly as you can this time’). The dependent variables consisted of ‘time 1’ under neutral instruction, ‘time 2’ under inhibition instruction, ‘time discrepancy’ computed by difference between time 2 and time 1, and a 3-point (0–2) ‘degree of deviation’ score. Greater time discrepancy indicates better participant inhibition (slowing down) of the continuous tracing response.
Procedure
The Institutional Review Board of National Taiwan University Hospital approved this study prior to its implementation in June 2005. We obtained written informed consent from the child participants and their parents. In order to minimize the influence of methylphenidate, children with ADHD were asked to halt medication 1 day before the tests.
Children with DSM-IV ADHD and the controls received the same assessments with psychiatric interviews, a parent-reported questionnaire, and neuropsychological tests. Parents of the children with ADHD and the controls were interviewed using the Chinese K-SADS-E to assist in making the DSM-IV diagnosis of ADHD and its comorbid conditions; and then filled out the SNAP-IV-C scale while the child participants were assessed using the WISC-III, a series of neuropsychological tasks, and behavioural observation during the tests. For all the subjects the first author (CM Chiang) rated the CGI-ADHD-S first, then SS Gau, a child psychiatrist with extensive experience of clinical work and research on ADHD, finalized the score of the CGI-ADHD-S at the clinic.
Statistical analysis
Statistical analyses were performed using SAS 9.1 (SAS Institute, Cary, NC, USA). One-way analyses of variance (ANOVA) were computed to address differences between children with and without ADHD. Duncan's new multiple range tests were used to adjust for multiple comparisons among the three groups.
We further conducted
Results
Behavioural symptoms
Children with ADHD-C significantly had the most severe symptoms of inattention, hyperactivity, and oppositional symptoms as measured on the SNAP-IV-C; overall ADHD symptoms as measured using CGI-ADHD-S; and the three behavioural items observed during the tests, followed by the ADHD-I group, and then the control group with the least (Table 2). There were some exceptions: the ADHD-C group did not differ from the ADHD-I group in the severity of inattention symptoms and the degree of giving up easily during the tests; and there was no difference between the ADHD-I and control groups in the oppositional symptoms.
Neuropsychological measures
Table 3 presents comparisons of the four components of attention tests and CTT among the three groups (ADHD-C, ADHD-I, and controls). In general, children with ADHD performed worse than children without ADHD in all the neuropsychological measures after adjustment for multiple comparisons and controlling for the confounding factors.
Neuropsychological findings
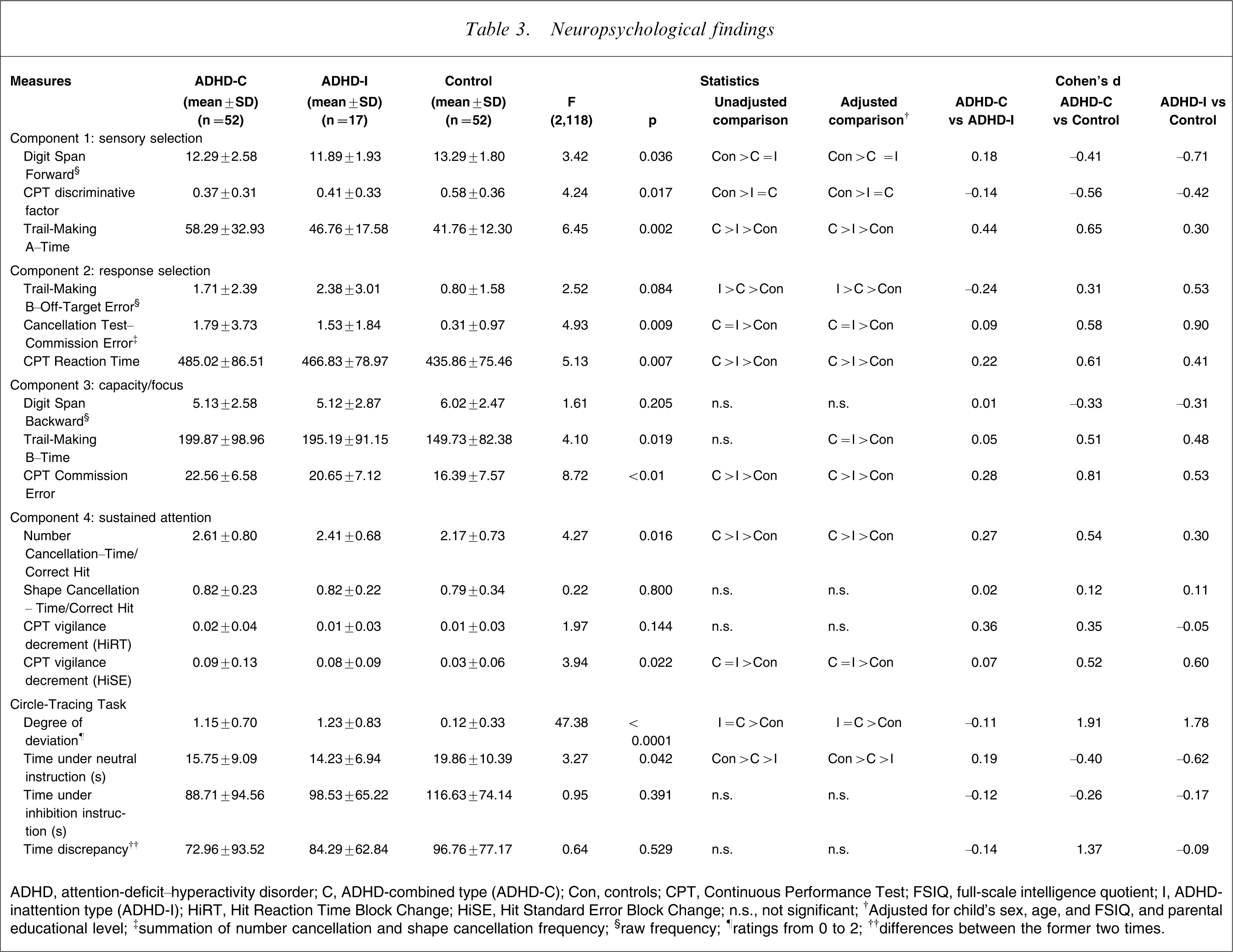
ADHD, attention-deficit–hyperactivity disorder; C, ADHD-combined type (ADHD-C); Con, controls; CPT, Continuous Performance Test; FSIQ, full-scale intelligence quotient; I, ADHD-inattention type (ADHD-I); HiRT, Hit Reaction Time Block Change; HiSE, Hit Standard Error Block Change; n.s., not significant;
Sensory selection
Both ADHD-C and ADHD-I groups had significantly lower scores on forward digit spans and CPT discriminative factors than the controls. The ADHD-C group had the longest time to complete the TMT-A, followed by the ADHD-I group, and then the controls, with the least.
Response Selection
The ADHD-C group had the longest CPT reaction time, followed by the ADHD-I group, and then the controls. Both ADHD groups had similar commission errors in the Cancellation test, significantly higher than the controls. In contrast, the ADHD-I group had the highest number of off-target errors on the TMT-B, followed by the ADHD-C group, and the controls, with the least.
Capacity/Focus
The ADHD-C group had the highest rates of CPT commission errors, followed by the ADHD-I group, and then the controls. Both ADHD groups had a longer time to complete the TMT-B than the controls. There was no difference in backward digit spans among the three groups.
Sustained attention
Compared with the controls, the two ADHD groups had higher ratios of time versus correct hits on the Number Cancellation Test (higher in the ADHD-C group), and had higher CPT vigilance decrements as measured by the HiSE (no difference between the two ADHD groups). There were no significant differences among the three groups in terms of the ratio of time/correct hits on the Shape Cancellation Test or CPT vigilance decrement measured by the HiRT.
Circle-Tracing Task
Both ADHD groups had similar degrees of deviation while tracing the circle, but it was higher than the controls. The ADHD-I group took the shortest time under neutral instruction to complete circle tracing, followed by the ADHD-C group, which had a shorter time than the controls. There was no significant difference among the three groups in terms of time under inhibition instruction and the time discrepancy between inhibition instruction and neutral instruction.
Discussion
As the first study examining the neuropsychological findings between two ADHD subtypes in an ethnic Chinese population, the present findings were similar to those of several Western studies. The major findings of the present study are that children with ADHD-C, compared to children with ADHD-I, had more severe ADHD-related symptoms, as rated by investigators and parents in clinical and daily settings, and more obvious behavioural symptoms during the neuropsychological assessments, except that children with ADHD-I had a similar severity of inattention and giving up easily during the tests to that of children with ADHD-C. Additionally, the present finding of no increase in oppositional symptoms in the ADHD-I group also contributed to the validity of ADHD subtypes using the clinical behavioural symptoms related to the diagnostic concept of ADHD. These findings lend evidence to support the validity of distinct ADHD-C and ADHD-I subtypes using the observed behavioural symptoms. Using the Cohen et al. model of attention [24] to distinguish ADHD from non-ADHD, and the ADHD-C and ADHD-I subtypes, the present findings strongly support the hypothesis that children with ADHD perform worse than normal controls in attentional tasks [41]. The present findings also provide evidence that the four attentional components assessed in the present study have discriminative validity in distinguishing ADHD-C from ADHD-I [15] in Taiwanese children.
The finding of a longer time to complete the TMT-A in children with ADHD-C than ADHD-I indicates increased difficulties in perceptual motor planning, and deficits in executive functions in the former [42]. The longer reaction time in ADHD-C than ADHD-I suggests that the deficits in the response re-engagement of ADHD-C lead to the failure of attention in response selection [32]. Consistent with the Kirlin study [43], the present findings also suggest that children with ADHD-C are more impulsive because of increased CPT commission errors and have greater difficulties maintaining attention because of increased Time/Correct Hit for the Number Cancellation Test in ADHD-C than ADHD-I.
In contrast, as in some studies, there were no subtype differences in the commission errors of the Cancellation Test, TMT-B time, HiRT of CPT, and degree of deviation in the CTT, and there were no group differences in backward digit span, Time/Correct Hit of the Shape Cancellation Test, HiRT of CPT, and time under inhibition instruction and time discrepancy of the CTT [17], [18], [30]. The negative results may be attributed to the immature development of attention capacity in the younger sample (grades 2–4), lack of ability of these measures to distinguish the two subtypes, and the small sample size. Because ADHD is a common neurodevelopmental disorder it is essential to take developmental cognitive ability into consideration while assessing a child's attention capability [44]. For example, the target shape (star) of the Shape Cancellation Test may be too easy to use to discriminate ADHD from non-ADHD. It is also worth noting that some had argued that CPT has a common problem of lacking specificity and sensitivity [45]. Future research in clarifying the specificity and sensitivity for different variables of CPT is required.
Contradictory to the Lockwood et al. study showing no subtype differences in commission errors [30], the current study demonstrates more CPT commission errors in the ADHD-C than ADHD-I group. Moreover, this kind of subtype difference was also found in CPT Reaction Time. While previous studies have also included CPT as a helpful tool in diagnosing attention deficit disorder in children and suggested further multivariate studies of CPT usage and implication [46], [47], the aforementioned findings support the present incorporation of the CPT as one of the neuropsychological measures in differentiating ADHD subtypes, as Cohen et al. suggested [24].
The present study yielded several unique findings. In the sensory selection component, the ADHD-I children scored lower than the ADHD-C children on forward digit span. This discordant result indicates that children with ADHD-I may have difficulty receiving a series of audio stimuli. Although no previous evidence indicated differences between ADHD-I and ADHD-C on forward digit span [30], similar findings were found for the Story Memory task [48], which also required an audio-sensory selection ability. This trend corresponds to the Fisher notion that children with ADHD-I tend to have perceptual failure or miscuing while receiving audio-social information [49]. Another inconsistent finding was that children with ADHD-I made more off-target errors on the TMT-B than children with ADHD-C [30].
Limitations
The strengths of the present study are that it is the first study to examine the differences between ADHD subtypes using neuropsychological tests in an ethnic Chinese population, and that it includes adequate neuropsychological tests for the four attention components of the Cohen model, particularly the CPT. But the present study was limited by potential selection bias of the controls, limited neuropsychological tests, small sample size, and lack of inclusion of children with ADHD-HI. Although we recruited controls based on the distribution of gender, age, and schools of the ADHD group, we also relied on school teachers to suggest controls as having the same performance as children with ADHD if the latter could concentrate on school work. We recognized that such a selection criterion is a subjective one that may affect the present results. Indeed, the higher IQ scores and parental educational levels were not correspondent with research hypothesis. Although some authors have suggested the inclusion of all the affected measures as covariates to ensure that deficits in association with ADHD can be explained by group differences [50], others have argued that ADHD may directly cause lower IQ assessments [8]. Moreover, the finding of different IQ scores between children with and without ADHD was similar to previous studies [23]. The present finding did not indicate any confounding effect from IQ and parental education.
Implications
The present findings imply that in addition to parent-rated and investigator-rated behavioural symptoms, children with ADHD-C and those with ADHD-I show different profiles of the four attentional components proposed by Cohen et al. [24], in this Taiwanese population. The results support the hypothesis that neuropsychological tests are suitable measurements in assessing different attention components in children with ADHD, and suggest that neuropsychological assessments, particularly CPT, can be included to assist the diagnosis of ADHD and delineate the profiles of different ADHD subtypes in clinical and research settings. Moreover, as the first study using neuropsychological assessment to compare differences and similarities among normal control and two ADHD subtypes in an ethnic Chinese population, the present study provides a foundation for future cross-cultural studies on ADHD [51]. The next step will be the recruitment of children with ADHD-HI, an increased sample size of children with ADHD-I, recruitment of a wide age range of children, and the inclusion of more domains of neuropsychological tests.
Footnotes
Acknowledgements
This work is supported by grants from National Science Council, Taiwan (NSC 94-2815-C-002-177-H) and National Health Research Institute, Taiwan (NHRI-EX94-9407PC). We would like to express our thanks to Ms Chi-Mei Lee for her assistance.