
Abstract
Suicide is a major cause of death among young Australians aged 15–24 years, second only to motor vehicle accidents in the proportion of deaths it causes [1]. A recent UNICEF study [2] comparing youth suicide rates of 32 countries from Europe, America, Asia and Oceania ranked Australia as having the ninth highest rate of male youth suicide, with mainly Eastern European (ex-Soviet Bloc) countries having higher rates. Norway, Finland and New Zealand were the only other developed countries to have higher rates. Australia also had the 11th highest rate of female youth suicide. However, female rates were more comparable for all the countries, with higher rates again occurring in Eastern European countries.
The rate of youth suicide has increased particularly among males in recent years, both in Australia [3–5] and overseas [5,6]. A detailed comparison of the epidemiology of youth suicide in Australia and overseas has been provided by Cantor et al. [5].
Against this background, this paper examines Australian trends in youth suicide for the period from 1964 to 1997. This period was selected for study, as this is the period for which comprehensive data on causes of death are available from the Australian Bureau of Statistics (ABS). Cantor et al. [4] have recently presented an examination of this data in which they present trends in the prevalence of suicide for 10-year age groups over the period 1964–1997. They also made comparisons between suicide rates of Australia and 22 other countries. In confirmation of the UNICEF study [2], their analyses indicated that there has been an increase in the suicide rate among youth, and particularly among males. In contrast, the suicide rate declined among older age groups for the period 1964–1997. Similarly to the UNICEF study, Cantor et al. [4] presented evidence that Australia has one of the highest youth suicide rates (particularly among males) but that Australian suicide rates among older adults are relatively modest.
Given findings of high and apparently increasing rates of suicide among Australian youth (15–24 years), the present paper concentrates on this age group. The analyses reported by Cantor et al. [4] will be extended by using methods of age-period-cohort analyses. These analyses provide a means to disentangle age, period and cohort effects on the rate of youth suicide.
Aims
The specific aims of the paper are to examine trends in suicide between 1964 and 1997 in eight five-year birth cohorts of Australians born between 1940 and 1979. This data will be used to:
Describe trends in suicide in Australians aged 15–24 years between 1964 and 1997.
Describe differences between birth cohorts in suicide mortality.
Distinguish between age, period and cohort contributions to the increase in the youth suicide rate over this period.
Method
Data were obtained from the ABS on gender and age at death for suicide deaths among Australians aged 15–24 years, between 1964 and 1997 inclusive. Data were also obtained from ABS on the total number of deaths. Population estimates were obtained from the ABS estimates of resident population in the mid-point of each calendar year.
Between 1964 and 1967 suicide deaths were defined as deaths due to ICD-7 codes E970–E979; between 1968 and 1978 they were defined as deaths due to ICD-8 codes E950–E959 and between 1979 and 1997 suicide deaths were defined as deaths due to ICD-9 codes E950–E959.
These data were used to estimate the rate per 100 000 males and females aged 15–24 years of deaths attributed to suicide in each year between 1964 and 1997. The rate of deaths attributed to suicide was also estimated for males and females in each of the following birth cohorts: 1940–1944, 1945–1949, 1950–1954, 1955–1959, 1960–1964, 1965–1969, 1970–1974, and 1975–1979. An age-period-cohort analysis [7] using Poisson Regression (as implemented in the
Results
Trends in suicide
The rate of suicide among Australian males aged 15–24 years increased from 8.7 per 100 000 in 1964 to 30.9 per 100 000 in 1997 (see Fig. 1). This represented a 3.5-fold increase (95% CI = 2.8–4.5) in the rate of suicide and is consistent with previous reports of a rising rate of suicide among young males [3,4]. In contrast, Figure 1 shows that the rate of increase in suicide among young females was much less marked: the rate among females aged 15–24 years was 5.2 per 100 000 in 1964 and 7.1 per 100 000 in 1997 (OR = 1.4, 95% CI = 1.0–2.0).
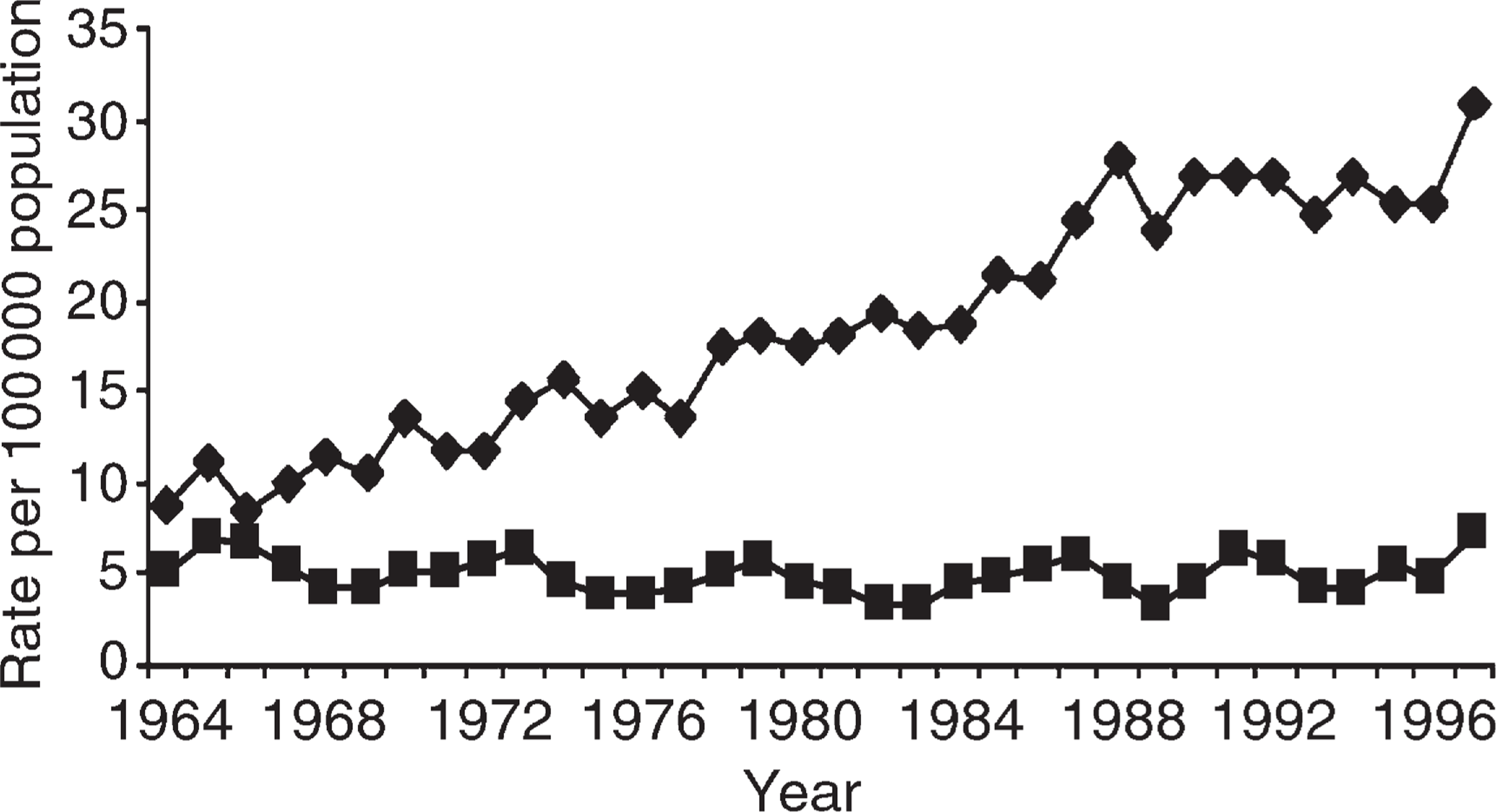
Rate (per 100 000) of suicide among males and females aged 15–24 years, 1964–1997. ♦, males; ▪, females.
The proportion of all deaths that were attributed to suicide in this age group clearly demonstrates that suicide is a leading cause of death among young Australians. The proportion of all deaths among males aged 15–24 years rose from 5.9% in 1964 to 29.2% in 1997. Among females, the proportion of all deaths attributed to suicide rose from 8.3% in 1964 to 18.4% in 1997.
Gender, cohort and period trends in suicide
Rates of suicide were significantly higher among males than among females, with male deaths accounting for 80.3% of all suicide deaths over the period from 1964 to 1997. Males made up a progressively higher proportion of all suicide victims over this period: from 64.1% of all youth suicides in 1964 to 82.8% by 1997. Males had a significantly higher risk of dying from this cause than had females in all birth cohorts [incidence rate ratio (IRR) = 4.04, 95% CI = 3.85–4.24].
The age-period-cohort analysis indicated that there were marked differences in rates of youth suicide between periods. Compared with the period from 1964 to 1969, the rate of youth suicide was 1.4 times higher in 1970–1984 (IRR = 1.40, 95% CI = 1.27–1.54), and approximately twice as high in 1985–1997 (IRR = 1.97, 95% CI = 1.77–2.20).
Rates of youth suicide also differed according to age. Rates of suicide were lowest for those aged 15–16 years. Compared with this group, the rate of suicide was around 2.6 times higher in those aged 17–18 years (IRR = 2.55, 95% CI = 2.31–2.81) and 4.3 times higher among those aged 19–24 years (IRR = 4.33, 95% CI = 3.97–4.71).
The rates among those from different birth cohorts did not differ dramatically after the effects of gender, age and period had been taken into account. There was a slightly lower risk of suicide among those in the 1945–1949 birth cohort compared to those born between 1940 and 1944, with no other significant differences between any of the cohorts and this reference group. These results indicate that the differences in rates of suicide over the period 1964–1997 can largely be attributed to period differences in rates of suicide. There was little evidence that suicide rates varied markedly between birth cohorts once these period effects had been taken into account.
Discussion
In confirmation of previous published research, this paper has documented a rise in both the number and rate of deaths attributed to suicide in Australia during the period from 1964 to 1997. The first explanation of the increase in the rate of suicide between 1964 and 1997 that needs to be excluded is the possibility that it is a result of changes in the way that causes of death have been coded. A detailed discussion of potential liabilities of national mortality data on suicides has been provided by Diekstra et al. [6]. On the basis of a review of studies of the reliability and validity of national suicide mortality data they concluded that there are likely to be few systematic errors in reporting of suicide deaths. This means that national statistics can be used to make valid comparisons of the suicide rate across time. A detailed discussion of case ascertainment, data collection practices and the reliability of suicide data in Australia has recently been published by Cantor et al. [5].
Further analysis indicated that the rise in youth suicide could largely be attributed to period effects, with little evidence of cohort effects. This suggests that societal and other changes may be responsible for the rise in youth suicide, implying that (assuming no substantial changes in these conditions) young people in subsequent cohorts will continue to be at elevated risks for suicide. The attribution of the rise in youth suicide mortality to a period effect suggests that as individuals mature into later adulthood, they should no longer be at increased risks of suicide. This is in contrast to what would be expected if a cohort effect existed. Specifically, in an earlier analysis of suicide trends Goldney and Katsikitis [9] noted that a cohort effect would be associated with increased risks of suicide throughout the life span.
Evidence of a period effect in suicide in Australia has been matched by a number of international studies that have indicated period effects on the rate of suicide in various countries including Spain [10], Italy [11], West Germany [12], Canada [13], England [14] and the USA [15]. Contrary to the findings reported in this study, however, a number of these studies have also reported the existence of cohort effects in the rate of suicide, although in these studies both period and cohort effects have been more apparent among males than among females. This may be a reflection of greater statistical precision in the estimation of these effects for males due to the higher base rate of suicide among males.
The finding that the rise in youth suicide can be attributed to a period effect is in contrast to the pattern of results seen in a similar age-period-cohort analysis of opioid overdose mortality in Australia [16]. The results of this analysis revealed strong cohort effects: the rate of overdose in the 1975–1979 cohort was approximately 20 times higher than the corresponding rate for the 1940–1944 cohort. This cohort effect was presumed to reflect historical changes in the cohorts' exposure to heroin use as it has only been relatively recently (since the late 1960s) that illicit heroin has been used in Australia.
In confirmation of previous research, there were marked gender differences in the rate of youth suicide, with males accounting for approximately 80% of all suicide deaths over the period from 1964 to 1997. Given that the rate of increase in the male suicide rate was also higher than that of females, the relative proportion of total suicides that occurred among males increased over the time period studied, from approximately 60% in 1964 to approximately 80% by 1997.
The rise in suicide over this period has been paralleled by a general rise in the rates of many psychosocial disorders among youth, including affective disorders [17,18] antisocial behaviours [19,20] and substance-use disorders [16,21]. Much of the evidence of rising rates of psychosocial disorders among youth is derived from overseas studies. However, given the broad similarities in many of the social conditions in Australia and these countries, coupled with local evidence of rising rates of suicide and substance-use disorders [16], it seems reasonable to conclude that rates of psychosocial disorders among Australia youth have risen in the past 50 years. Given continued findings that psychiatric disorders are a major risk factor for suicide [22,23], it is possible that at least some of the rise in youth suicide may be attributed to rising rates of psychiatric and psychosocial problems among youth.
However, there are two potential problems with attributing the rise in youth suicide merely to a corresponding rise in the rate of psychosocial disorders among youth. First, the mechanisms underlying the apparent increase in rates of psychosocial disorders remain largely unknown. In a comprehensive examination of possible causal mechanisms underlying this rise in psychosocial disorders Rutter and Smith [24] noted that this rise cannot simply be attributed to one specific social condition, such as unemployment or media influences. Rather, it reflects the combination of societal changes that have occurred in most developed societies since the end of the Second World War.
Second, the rise in these disorders, which has been more or less constant across males and females, cannot explain the apparent gender differences in the increase in youth suicide: there has been a substantial increase in the rate of suicide among young males but, in comparison, the suicide rate among young females has remained relatively static.
In conclusion, suicide is a major cause of mortality among young Australian adults. In 1997 it accounted for 29.2% of all deaths among males and 18.4% of all deaths among females aged 15–24 years. The rate of youth suicide has increased since 1964, particularly among males. Among those aged 15–24 there is a steady increase in risks of suicide with increasing age: rates of suicide are highest among those aged 19–24 years. During this period, there has been a corresponding rise among youth in the rate of a number of psychosocial problems including criminal activity, psychiatric disorder and substance-related problems. Given the multiple factors associated with the rising rate of youth suicide, it is clear that an effective response to reducing youth suicide must include a focus on identifying and treating psychiatric illness, as well as ameliorating the effects of disrupted and dysfunctional parenting, social disadvantage and life stress.