
Abstract
Increasing rates of hanging have been noted in many countries around the world in recent years, including Belgium, Canada, Denmark, Japan, the Netherlands, New Zealand, Scotland, and the United Kingdom [1–4]. In addition, a number of studies have claimed that hanging is now the leading method of suicide in a range of countries that vary greatly in terms of cultural and social features, for example, Ireland [5], Ethiopia [6], Hong Kong [7].
In Australia, rates of hanging among males have also been increasing for the past 20 years. Hanging suicides increased four-fold among Australian males during the period 1980–1997, from 2.1 to 8.8 per 100 000 [Australian Bureau of Statistics, unpublished data]. In each of Australia's five most populated states (New South Wales, Victoria, Queensland, South Australia and Western Australia), male hanging rates increased from 1980 (1.8 to 2.6 per 100 000) to 1997 (7.7–10.2 per 100 000) [Australian Bureau of Statistics, unpublished data], demonstrating that the increase in hanging rates is distributed evenly throughout Australia. The continued increase in hanging rates has made hanging the major method of suicide among Australian males, overtaking firearms, which had been the major method of suicide among males throughout the 1970s and 1980s.
With rising rates of hanging suicides in Australia and abroad, there is a need to gain insight into this particular method of suicide, independent of suicides by other methods. To date, most studies have considered hanging suicides in combination with suicides by all other methods.
One study that focused specifically on hanging was by Pounder, in which the association between hanging as a method of suicide and the increasing British suicide rate was examined [3]. He suggested that the increase in British hangings may be the result of increased acceptability of hanging following the elimination of hanging as a capital punishment in Britain in 1965. While this study offers a possible explanation for the increase in hanging rates, the hypothesis was not tested, nor were hanging suicides examined beyond an observation of trends across time.
In a recently published study of hanging suicides it was suggested that unemployment, experience of personal loss, psychiatric illness, and alcohol use were possible precipitating factors leading to hanging in people under the age of 25 [8]. This study, partly based on the same data as the current study, was limited as there were no comparisons made between hanging and suicides by other methods.
To the authors' knowledge, there are only two published reports of comparative studies between hanging and other methods of suicide. In a study of suicides in New York between 1984 and 1985, jumping suicides were compared with suicides by hanging, drug overdose, and shooting, the four major methods of suicide for this area [9]. This study provided limited information on hanging suicides as its focus was on jumping rather than hanging. Consequently, data were presented in such a way that hanging could be compared with jumping but not the other two methods. Hanging was less likely to have been used than jumping among by 24–64-year-olds. Hanging was significantly less likely than jumping among people who were unemployed or had a history of mental or emotional problems but significantly more likely than jumping among people with a history of personal or social problems.
In a later study, a comparison was made between hanging and cutting suicide attempts among a sample of 754 South Carolina jail inmates [10]. Again, this study provided limited information on hanging as it was specific to a prison population. In comparison with inmates who attempted cutting, inmates who attempted hanging were more likely to have been intoxicated at the time of arrest, to have been arrested on alcohol related charges and to have made their attempt within an hour of their arrest.
The current study aimed to provide a deeper understanding of hanging as a suicide method, by comparing hanging suicides with other common suicide methods in the general population. The characteristics of males who completed suicide by hanging in Queensland, Australia between 1994 and 1996, were compared with the characteristics of males who suicided by firearm or nondomestic gas over the same period.
Method
Data for the study were obtained from the Queensland Suicide Register (QSR), maintained by the Australian Institute for Suicide Research and Prevention (AISRAP). The data contained in the QSR are derived from several sources including a brief police report, a post-mortem examination report, a toxicology report, and a psychological autopsy report. The psychological autopsy report is designed by AISRAP and completed by a police officer based on information obtained from family and/or friends of the deceased and witnesses to the suicide incident. The report addresses a range of social, psychological, and health factors related to the deceased. Each case of suicide in the QSR is assigned an ICD-9 code for external cause of death. Detailed information about the QSR is provided by Baume et al. [11].
Cases of suicide in the QSR that met the following criteria were included in the current study: (i) deceased was male; (ii) death occurred between 1994 and 1996; (iii) usual place of residence was Queensland; and (iv) cause of death was classified as either hanging (ICD-9 code E953.0), firearm (ICD-9 code E955.0–E955.9), or nondomestic gas (ICD-9 code E952.0–E952.9). The current study was restricted to males as the small number of females who met criteria (i) through (iv) above was not suitable for statistical analysis. Nondomestic gas refers to a gas that is not in domestic use and in the majority of cases refers to motor vehicle exhaust gas.
Nine-hundred and fifty cases met the above criteria, representing 76% of suicides by males in Queensland for the 1994–1996 period. Of the 950 eligible cases, there were 401 by hanging, 316 by firearm, and 233 by non-domestic gas. As a proportion of all suicides by males in Queensland over the period, these methods represented 32%, 25%, and 19%, respectively. Hanging, firearms, and non-domestic gas, as proportion of all suicides among Queensland males, were consistent with proportions for all Australian males (32%, 22%, and 24%, respectively).
The characteristics of males who completed suicide using hanging, firearms and non-domestic gas were compared using a range of variables. The variables were grouped and results reported within the following themes: personal characteristics (age and ethnicity); social characteristics (geographical location of residence and household composition); suicide incident (suicide note, and suicide site); previous suicidal behaviour (prior suicide attempts); mental health (previous psychiatric treatment and psychiatric diagnoses); and legal history (prior legal trouble). Ethnicity was divided into three categories: ‘Caucasian’, ‘indigenous Australian’, and ‘other non-Caucasian’. The Caucasian and other non-Caucasian categories included people born outside Australia. Geographical location was divided into ‘metropolitan’, ‘provincial’, and ‘rural’ according to population size [12]. Metropolitan included Brisbane and some surrounding areas, provincial included any community with a population more than 20 000, and rural included any communities with a population under 20 000. Household composition was divided into ‘living alone’ or ‘not alone’. Suicide site was divided into ‘residence’ and ‘not at residence’. Psychiatric diagnoses refer to specific diagnostic categories. The remaining variables in the study had dichotomous (yes/no) categories.
Variables in the study differed in the proportion of cases with missing values. The primary cause of missing values in the data was that psychological autopsy reports were only obtained in approximately 70% of cases. An additional reason for missing values in the data was the occasional unavailability of suitable informants for the completion of psychological autopsies or the informant's genuine lack of knowledge about certain aspects of the deceased's life. Where missing values differed between methods, this is elaborated on in results. The proportion of each category of a variable is based on positive values only (i.e. excluding missing values). For previous psychiatric treatment, physical illness, and legal history, missing values are considered ‘no’ responses, as informants typically respond that the information is unknown where the presence of these circumstances is not apparent. As such, no missing values analyses were undertaken for these variables.
An ANOVA was used to compare methods for age; relative risks (RR) were used to compare methods for ethnicity and geographical location with 95% confidence intervals; and chi-squared statistics were used to compare methods for all other variables.
Results
Results are summarized in Table 1 with notable results mentioned in text.
Characteristics of suicides compared by method, and chi squared statistics
Personal characteristics
People who suicided by hanging were significantly younger (M = 35.72, SD = 17.02) than people who suicided by firearms (M = 42.78, SD = 19.04) and non-domestic gas (M = 40.79, SD = 15.18), F (2,946) = 15.83, p< 0.001. Figure 1 shows the proportions of each suicide method used by people in five-year age groups. Both hanging and firearm suicides peaked in the 20–30 years age groups. While the proportion of hanging suicides appeared to decrease in older age groups, the proportion of firearm deaths remained rather constant. Non-domestic gas suicides peaked in the 30–45 years age groups and decreased with increasing age. Nearly half of the males who used hanging were under 30 years of age, compared with only one third of the males who used firearms and a quarter of the males who used nondomestic gas.
Proportion of suicide methods; shown in 5-year age groups. ▴ Firearm; • hanging; ▪ non-domestic gas.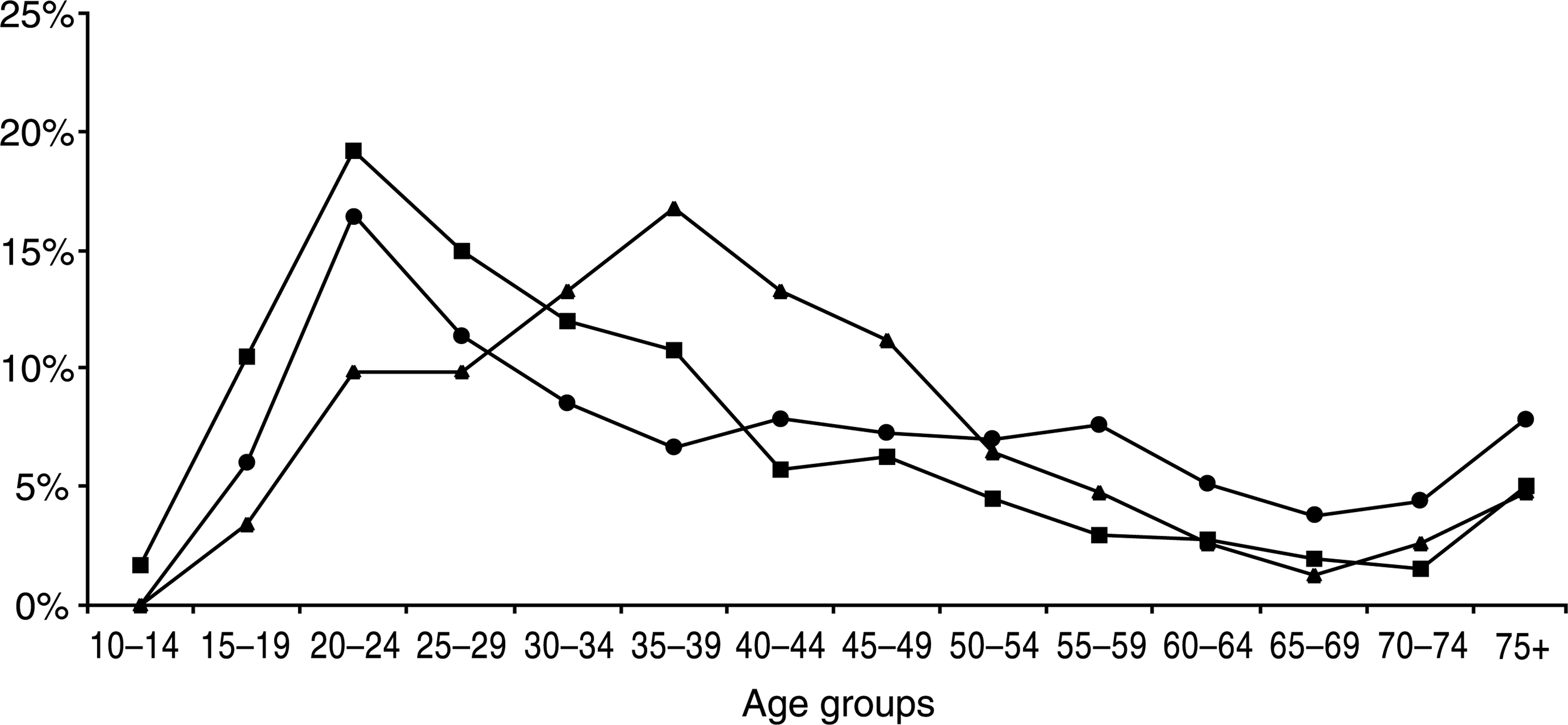
The ethnicity of the deceased was missing in 14% of cases (n = 137) but there were no differences between methods on missing values. Of the remaining 813 cases, 723 were Caucasian (89%), 73 were indigenous Australians (9%), and 17 were other non-Caucasians (2%). Differentiating by method, indigenous males represented 19% of hanging suicides (n = 65), 3% of firearm suicides (n = 7), and less than 1% (0.5%) of non-domestic gas suicides (n = 1). Hanging rates were significantly higher among indigenous males (RR = 7.65; 95% CI: 6.0–9.6) compared with the total male population (62.40 vs 8.15 per 100 000). Twelve per cent of hanging suicides by indigenous males occurred while in prison, compared to only 4% of hanging suicides by non-indigenous males, significantly different proportions (χ2 (1) = 6.53, p < 0.05). Firearm rates did not differ between indigenous males and the total male population (RR = 1.05; 95% CI: 0.8–1.3). A rate for non-domestic gas was not calculated for indigenous males, as there was only one such case.
Social characteristics
Rates of hanging and non-domestic gas did not differ significantly across the three geographical locations. The firearm rate in rural areas (13.41 per 100 000) was significantly greater than the firearm rate in metropolitan areas (4.91 per 100 000; RR = 2.73; 95% CI: 2.2–3.3) and provincial areas (5.88 per 100 000; RR = 2.28; 95% CI: 1.9–2.8). In metropolitan areas, the hanging suicide rate (8.00 per 100 000) was significantly greater than firearm rate (4.91 per 100 000; RR = 1.63; 95% CI: 1.32–1.98) and non-domestic gas rate (5.05 per 100,00; RR = 1.58; 95% CI:1.29–1.92). In provincial areas, the hanging rate (8.98 per 100 000) was also significantly greater than firearm rate (5.88 per 100 000; RR = 1.53; 95% CI:1.24–1.87) and non-domestic gas rate (4.89 per 100 000; RR = 1.84 95% CI:1.46–2.29). In rural areas, rates of firearm (13.41 per 100 000) and hanging (10.02 per 100 000) were significantly greater than the non-domestic gas rate (5.80 per 100 000; RR = 2.31; 95% CI:1.70–3.06; and RR = 1.73; 95% CI:1.28–2.29 respectively). There were no missing values for this variable.
The suicide victim lived alone in 20% of hanging suicides, 27% of firearm suicides, and 36% of non-domestic gas suicides. People who used hanging were significantly less likely to live alone than people who used non-domestic gas (χ2 (1) = 12.27, p < 0.001). Household composition was unknown in 31% of cases. Missing values differed significantly by method, with cases of hanging more likely to have missing values (36%) than firearm (27%) or non-domestic gas cases (28%; χ2 (2) = 8.77, p < 0.05).
Suicide incident
A suicide note was located at the scene in 34% of hanging suicides, 44% of firearm suicides, and 53% of non-domestic gas suicides. Each method differed significantly from the others for the presence of a suicide note (χ2 (2) = 22.35, p < 0.001). Missing values were present in only 3% of cases.
For both hanging and firearms, the greatest proportion of suicides occurred at the person's residence (73% and 71%, respectively) while just under half of the non-domestic gas suicides (49%) occurred at the person's residence. Non-domestic gas suicides were significantly less likely to occur at the person's residence compared with hanging suicides (χ2 (1) = 37.36, p < 0.001) and firearm suicides (χ2 (1) = 26.50, p < 0.001). There were missing values in less than 1% of cases.
Prior suicidal behaviour
Previous suicide attempts were evident in 34% of hanging suicides, 18% of firearm suicides, and 34% of non-domestic gas suicides. People who used firearms as a method of suicide were significantly less likely to have made a suicide attempt in the past, compared with people who used hanging (χ2 (1) = 14.74, p < 0.001) and non-domestic gas (χ2 (1) = 13.26, p < 0.001). Missing values for previous suicide attempts were present in 31% of cases. Cases of hanging were more likely to have missing values (35%) than non-domestic gas cases (24%; χ2 (1) = 9.22, p < 0.05) but not firearm cases (31%).
Mental health
There were no significant differences between methods for previous psychiatric treatment or diagnosis of depression. Depression (unipolar or bipolar) was the most commonly diagnosed disorder for all three methods, accounting for 61% of all diagnoses. Psychotic disorders, including schizophrenia, were the next most frequent diagnoses, accounting for a further 13% of all diagnoses. A significant difference was found between the three methods, with a diagnosis of a psychotic disorder being more likely in hanging suicides than firearm suicides (χ2 (1) = 4.17, p < 0.05) and non-domestic gas suicides (χ2 (1) = 9.72, p < 0.01). Among the males diagnosed with a psychotic disorder, 70% used hanging but only 20% used firearms, and 10% used non-domestic gas. Missing values for psychiatric diagnosis were present in 7% of cases.
Legal history
A history of legal trouble was reported in 21% of hanging suicides, 17% of firearm suicides, and 13% of non-domestic gas suicides. People who used hanging as a suicide method were significantly more likely to have had a history of legal trouble, compared with people who used non-domestic gas (χ2 (1) = 6.49, p < 0.05). After controlling for suicides in institutional care (i.e. hospitals and prisons), history of legal trouble was no longer significantly different between methods.
Discussion
The purpose of this study was to identify characteristics that could distinguish males who completed suicide by hanging from males who completed suicide by firearms and non-domestic gas. Researchers have suggested that availability and socio-cultural acceptability are both important influences on choice of suicide methods [13, 14]. Furthermore, particular suicide methods might be more acceptable to certain subgroups of individuals than other methods [9].
In the current study, differences between hanging, firearm, and non-domestic gas suicides on factors such as age, geographical location, and legal history may be explained by differential access to methods. The bulk of hanging suicides were found to be concentrated in the younger age groups, while non-domestic gas suicides were concentrated in the middle age groups, and firearms were more evenly distributed across age groups. It may be that hanging is more common in the younger age groups due to access issues, as young males may be less likely to own a car or a firearm. It has been shown that non-domestic gas suicide is uncommon when car ownership is low [15]. Easy access to firearms probably accounts for most of the elevated firearm rate found in rural areas. For a significant number of people living in rural areas, firearms are a normal part of life, being commonly used for pest control and recreational hunting. Numerous studies have demonstrated that when the availability of firearms is high, firearms are used more frequently as a suicide method [16–18]. Differential access to methods would also account for the higher proportion of people with legal trouble who use hanging compared with firearms and non-domestic gas. While legal trouble was significantly more common among people who used hanging as a method, this difference was no longer apparent after controlling for suicides within institutional settings. People who are institutionalized due to legal trouble are very limited in the methods of suicide that are available to them [19].
Differences between hanging, firearms, and nondomestic gas on most other variables under study may reflect different acceptability of methods by subgroups of individuals. Indigenous males may be one subgroup of individuals who have a greater acceptability of hanging. Indigenous males were over seven times more likely to hang themselves, compared with the whole male population. Indigenous males were also more likely to suicide within prison than non-indigenous males, however, this cannot account entirely for the elevated rates of hanging among indigenous males. Cultural identity may make an important contribution to the frequent use of hanging by indigenous males. By using hanging as a suicide method, indigenous males may be adhering to what has been established as a social norm among their people [20]. It may also be that indigenous males have limited access to methods, such as low gun and car ownership.
Individuals with poor impulse control may be a second subgroup that has a greater acceptability of hanging, particularly when compared to non-domestic gas. While impulsivity has been found to distinguish suicide attempters from non-attempters among clinical populations [21–23], research has yet to examine a possible association between impulsivity and specific suicide methods. The authors hypothesize that differences in planning and preparation required for each suicide method may make hanging the preferred method to impulsive individuals. Ligature for hanging is easy accessible and requires little preparation. In contrast, for use of motor vehicle exhaust gas, it is necessary to attach a hose to the car exhaust, block air vents and windows, and wait 15–20 minutes for the method of suicide to take effect.
There were features of hanging suicides in the current study which suggest that hanging may be preferred by more impulsive individuals. Suicide notes were less likely to be left at the scene in hanging suicides than the other two methods. Taking time to write a suicide note may indicate a higher degree of planning and forethought, and a less precipitate decision-making process [24]. This inference is supported by the finding that the method requiring the most preparation, non-domestic gas, is also the method that is most likely to have a suicide note left at the scene. In addition to being less likely to leave a suicide note, people who used hanging were far more likely to suicide at their residence compared with people who used non-domestic gas, despite being less likely to live alone. Non-domestic gas may be used by individuals because of the ability to travel away from the home and spare family or friends the trauma of finding their body. The tendency for people who use non-domestic gas to travel away from their residence to complete suicide again indicates a level of planning and preparation not present in hanging suicides.
People diagnosed with a psychotic disorder had a strong preference for hanging, possibly supporting the authors' hypothesized association between impulsivity and hanging. This preference for hanging among people with psychotic disorder may be associated with the characteristics of poor impulse control and acting-out, which are often manifest in these individuals [23, 25]. The present study is consistent with previous studies that have found people with schizophrenia typically use lethal and easily executed suicide methods [9, 26]. For people with a psychotic disorder, poor impulse control may render easily executed methods such as hanging more acceptable than methods such as firearms, which can be difficult to locate, and non-domestic gas, which requires detailed planning and preparation.
Inconsistent with the proposition that more impulsive individuals have a preference for hanging is the finding that prior attempts were more common among people who use hanging and non-domestic gas than people who use firearms. The presence of prior attempts may suggest that an individual's suicide is the result of intense and long-lasting psychological suffering rather than an impulsive reaction; however, recent research has shown that the suicidal crises experienced by multiple attempters are more intense but of no greater duration than crises experienced by first time-attempters [27, 28].
The findings in the current study support restriction of access to methods as a suicide prevention technique. As pointed out by Fisher et al. [9], where a subgroup of individuals have a preference for a particular method, they may be unlikely to substitute that method for another. Restricting access to methods has been shown to reduce overall suicide mortality from firearms and domestic gas in a number of well-documented studies [29, 30]. Restricting access to hanging may also be effective in preventing suicides but only in institutional settings [14, 31, 32].
Some alternative directions for suicide prevention techniques targeting hanging suicides are provided by the findings of the current study. Given that the bulk of hanging suicides were found to occur in people under 30 years of age, a focus should be placed on early intervention. School-based programmes that focus on enhancing adaptive coping strategies, have been used in the reduction of anxiety and depression in adolescents [33, 34]. If people who use hanging are more impulsive than people who use other methods, this type of strategy may be particularly beneficial in reducing hanging rates. Such a strategy may foster the development of skills to overcome short-term suicidal crises or avoid negative life events developing into suicidal crises. There has not been, however, a longitudinal evaluation of the ability of such programmes to reduce self-harm or completed suicides.
The current study shows that people who use hanging are often in high-risk groups – one-fifth had prior legal troubles, almost one-third had past or current psychiatric treatment and more than one third had made previous suicide attempts. Targeting high-risk groups may be one avenue for reducing hanging, along with suicides by other methods. In particular, attention should be paid to ensuring appropriate follow up for people discharged from hospital settings following an attempt or psychiatric treatment. Such individuals are at much higher risk of suiciding than people in the general community [35].
Limitations of the study
Psychological autopsies are retrospective reports from family, friends or acquaintances that are completed shortly after a suicide, and are therefore open to inaccuracies. Furthermore, in the process of investigating a death, police officers’ primary concern rests with legal issues rather than research issues. For these reasons, it is suggested that the hypotheses raised through this investigation be considered with caution. It is important that researchers continually explore avenues for improving data collection processes but in a controlled and systematic way. It is also suggested that greater efforts need to be made to create a positive attitude towards research in a variety of professional groups that have direct involvement with behaviours that are major public health concerns. Finally, in interpreting results from this study, it must be kept in mind that analyses were limited to associations. Therefore, the hypotheses should be tested further to establish causal relationships.
Footnotes
Acknowledgements
The authors would like to acknowledge Queensland Health for providing the resources and support for the maintenance of the Queensland suicide register.