
Abstract
Suicide is an important cause of death in Australia, accounting for 3.2% of male and 0.9% of all female deaths in 1997 [1]. Indeed, more Australians die from suicide than in motor vehicle accidents [1]. Young Australians experience particularly high rates of suicide [1,2] and over the last 30 years these have almost doubled among males aged 15–34 years, from 16.8 per 100 000 in 1968 to 32.9 per 100 000 in 1997 [3]. In contrast, rates have changed little in young females. In both sexes the frequency of suicide by hanging has increased five- to sevenfold over this period, but in females the impact of this on the overall rate has been offset by a decline in suicide by drug overdose (previously the preferred method in females) [3].
Approximately 30% of the Australian population live in non-metropolitan areas and there is growing recognition that some aspects of their health are considerably worse than that of their metropolitan counterparts [4]. In particular, increased rates of suicide have been reported among non-metropolitan residents [4]. The most up-to-date comparative analysis of trends in non-metropolitan and metropolitan suicide refers to data up to 1993, and was largely restricted to 15–24-year-old males [5,6]. Dudley et al. [5,6] reported rates of male youth suicide to be higher among non-metropolitan than metropolitan residents, and showed that the recent rise in youth suicide was much greater in rural than more populous areas. They also noted a fall in firearm suicides in metropolitan areas, but an increase in non-metropolitan areas.
To further investigate recent secular trends and to provide an updated comparison of non-metropolitan and metropolitan suicides, we have analysed data for 1988–1997. As a recent analysis indicated that rises in suicide have occurred to a similar extent in 15–24 and 25–34-year-old males we have extended Dudley et al.'s analysis [5,6] to include both these age groups. Here we report overall and method-specific rates for males and females aged 15–24 and 25–34 years separately.
Method
Data sources
Data were obtained under a consultancy with the Australian Bureau of Statistics (ABS). Deaths classified as ICD codes E950–9 (suicide) and E980–9 except E988.8 (undetermined deaths) were identified from the ABS mortality file. We included both suicide and undetermined deaths in this non-metropolitan : metropolitan analysis as the preferred methods of suicide may differ in these two settings and the likelihood that a death is recorded as a suicide depends, in part, on the suicide method used [7]. The extent of underestimation of overall suicide rates by the coding of some probable suicides as ‘undetermined’ and others as ‘accidental’ is uncertain in Australia [8]. Some undetermined deaths are not due to suicide, but many probably are, and as coroners vary in the proportion of likely suicides to which they assign open, rather than suicide verdicts, this approach avoids underestimation. While underestimation may still occur by omitting ‘accidental’ overdoses or road traffic accidents that are in reality suicides, this effect is likely to be small in comparison with the alternative of excluding open verdicts. Undetermined deaths account for 15–20% of all deaths studied depending on age and sex.
Geographic classification of deaths is considered unreliable at sub-State level prior to the mid-1980s [ABS: personal communication] and so we limited our analysis to the last 10 years. We defined non-metropolitan as being a populated locality with ≤ 20 000 people and metropolitan as a populated locality with > 20 000 people. This decision was based on a number of factors. Firstly, analyses that use more levels of ‘rurality’ (large non-metropolitan, small non-metropolitan, remote and so on) have to exclude female suicide data as the number of cases becomes too small for analysis [5]. We felt it relevant to include all available data from both sexes. Second, there is no fully agreed definition of rurality in Australia: the widely used Rural-Remote Metropolitan Areas (RRMA) system is being replaced by the Accessibility-Remoteness Index of Australia (ARIA) based on geographical information system technology. Third, around 70% of Australians live in capital and other major cities with populations over 20 000 and the rest live in localities that are of population less than 20 000. Populated localities of less than 20 000 vary in population density from regional cities to small towns and villages. Hence, we do recognise that there is substantial heterogeneity in non-metropolitan Australia and note that our categorisation into metropolitan or non-metropolitan has some inherent limitations, as does any classification system.
Analysis
We initially compared overall population suicide rates in non-metropolitan and metropolitan areas, and then calculated all-cause and method-specific rates for 15–24 and 25–34-year-old males and females separately to identify any differences in patterns between these age/gender groups. To assess method-specific trends we focused on the main methods used in this age group: hanging, poisoning, firearms and gassing. Data are presented for the years between 1988 and 1997.
In the Tables we report annual rates per 100 000 population. The line graphs reflect 3-year moving averages, which were calculated to reduce annual variations and hence to ease identification of trends. When making statistical comparisons of rates we used the Poisson distribution to test differences.
Results
Overall suicide rates are approximately four times higher among males than females and the highest rates occur in non-metropolitan males (Table 1). Gender differences are greatest among non-metropolitan residents.
Suicide rate per 100 000 population for all ages by sex in metropolitan and non-metropolitan Australia 1988–1997 (annual rates)
Suicide rates among 15–34-year-olds
As seen for overall suicide rates, in both 15–24 and 25–34-year-olds gender difference in suicide rates are most striking in non-metropolitan areas (Table 2). For example, in 1995–1997 the rate for metropolitan males aged 15–24 years was 25.1 per 100 000 compared with 5.8 per 100 000 in females (a 4.3-fold increase). However, among non-metropolitan males of the same age group the rate was 38.2 and in females it was 6.4 per 100 000 (a 5.9-fold increase). There are similar differences in 25–34-year-olds.
Number and rate (per 100 000) of suicides by age group and sex in urban and rural Australia 1988–1997 (annual rates)
Over the years studied we found no clear evidence that suicide rates increased to a greater extent in rural than urban areas (Fig. 1). While overall suicide rates among males aged 15–24 and females aged 15–34 years show no clear secular trend (Fig. 1), there is a suggestion that rates in 25–34-year-old males in both non-metropolitan and metropolitan settings have increased in recent years. There is a striking difference between non-metropolitan and metropolitan suicide rates among 15–24-year-old males, that is not seen in 25–34-year-olds (Fig. 1). In 1995–1997 suicide among non-metropolitan males aged 15–24 years was 38.2 per 100 000 compared with 25.1 per 100 000 among metropolitan males of this age, a difference of over 50% (p < 0.0001). The opposite pattern was seen in 25–34-year-old females with higher rates in metropolitan areas, although this difference did not reach conventional levels of statistical significance (metropolitan rates in 1995–1997 were 7.5 per 100000 vs non-metropolitan rates of 6.1 per 100 000, p = 0.21).
Comparison of trends in age-specific rates of all cause suicide in non-metropolitan and metropolitan Australia, 1988–1997 for males (a) and females (b). -l-, age 15–24, metropolitan; -▴- age 25–34 metropolitan; …•…, age 15–24 non-metropolitan; …▪…, age 25–34 non-metropolitan.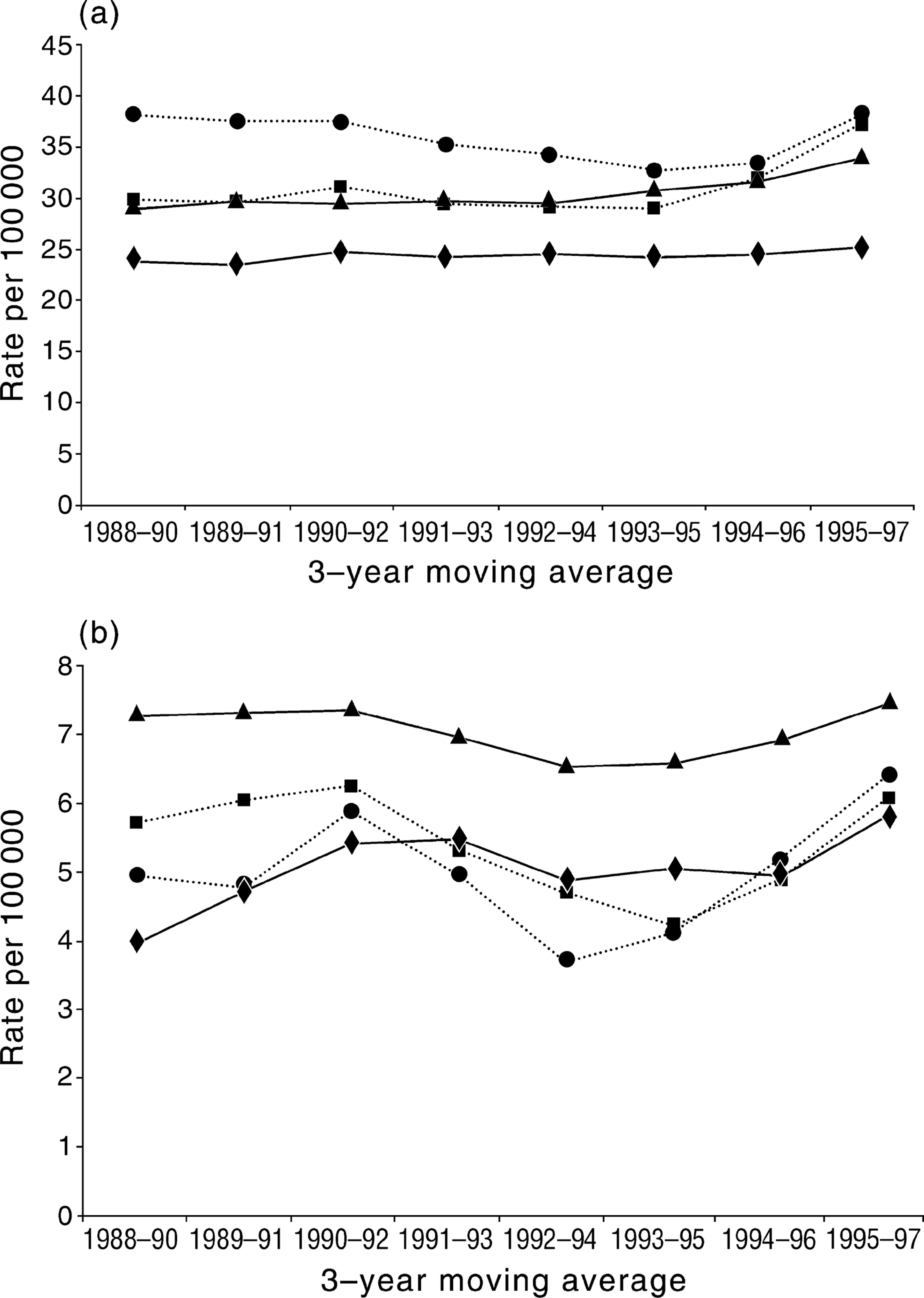
Suicide by hanging and firearms
Trends in method-specific suicide rates for males and females aged 15–24 and 25–34 years between 1988 and 1997 are shown in Table 3. There have been marked increases in hanging suicides in both age and sex groups in both metropolitan and non-metropolitan areas although among non-metropolitan females the smaller numbers preclude firm conclusions. Among non-metropolitan males, rates of suicide by hanging have approximately doubled, with the increase greatest among those aged 15–24 years.
Age and sex specific rates (per 100 000) of suicide by selected major causes in Australia 1998–1997 (annual rates)
Rates of firearm suicide have fallen two to threefold since 1988 among males and females (Table 3). These declines have been most marked in non-metropolitan settings. For example, among non-metropolitan males aged 15–24 years (who had the highest firearm suicide rate in 1988) rates have fallen from 22.9 in 1988 to 9.0 per 100 000 in 1997 (p < 0.0001). Despite these decreases, firearm suicide remains much more common among non-metropolitan than metropolitan males and females. In 1995–1997, firearm suicide was approximately three times as frequent among non-metropolitan than metropolitan residents.
Discussion
Our data demonstrate four important features in recent patterns of Australian youth suicide. First, 15–24-year-olds males living in non-metropolitan areas appear to be particularly vulnerable to suicide compared with their metropolitan counterparts; such effects of non-metropolitan living are not seen in older age groups or in females. Second, in contrast to the findings of Dudley et al. [5,6] for 1964–1993, we found no evidence that suicide rates have increased to a greater extent in rural than urban areas. This difference may have arisen because of the contrasting methods of geographical aggregation used in our analysis. Third, gender differences in suicide rates are more marked in non-metropolitan than metropolitan areas. Last, recent increases in the incidence of suicide by hanging [6] may represent method substitution away from firearms. These last two observations confirm those reported in other recent publications and so we will focus our discussion on the first main finding.
This study adds to previously published work on this issue [5,6] by providing updated and extended analyses for males and females aged 15–34 years. One possible weakness is that we have classified areas of residence simply as either non-metropolitan or metropolitan. This definition is pragmatic as most Australians do either live in large, metropolitan centres of over 20 000 people or in smaller, non-metropolitan localities and is in line with other work [4,5]. Analysis of small area data for relatively in frequent events such as suicide is potentially problematic. Indeed, Dudley et al., who used more levels of stratification [5,6], found it necessary to restrict almost all of their analysis to men for this reason. Ten years is a relatively small time to study trends, but we decided to limit our analysis because of ABS concerns over data quality prior to this period. It will be important to continue to monitor these trends prospectively.
We note that the rate of firearm suicide has fallen substantially in recent years probably due, in part, to the increasingly tight gun legislation in most of Australia [9,10]. While rates have fallen in both non-metropolitan and metropolitan settings and for both sexes, they remain higher among non-metropolitan residents, probably reflecting the higher levels of gun availability in these areas. These data suggest that, although the method of suicide used can be influenced by legislative intervention [11], as long as other effective means of suicide exist which are equally acceptable to suicidal individuals, method substitution may occur and overall suicide rates may not fall. Recent analysis of UK data has indicated that method substitution occurred (between non-violent methods) around the time that domestic gas supplies changed from coal (toxic) to natural (non-toxic) gas [Gunnel: unpublished data].
Despite the introduction in 1986 of regulations limiting the carbon monoxide content of car exhaust gases in Australia [12,13] rates of suicide due to car exhaust gassing have remained fairly stable over the past 10 years and are at similar levels in both non-metropolitan and metropolitan settings for both sexes. This probably reflects the ready availability of cars in both settings. In contrast, in the UK, recent analyses indicate that car exhaust gas legislation introduced in 1993 has resulted in reduction in overall and method-specific suicide rates in males [14]. Explanations for these differences in the effects of legislation in Britain and Australia are required.
Although our analysis makes no attempt to study the causes of suicide, the question of why young, non-metropolitan men may be at particular risk must be raised. Analyses of age-specific trends in suicide in relation to unemployment indicate that rises in suicide rates between 1966 and 1990 in 15–24-year-old males were associated with increases in youth unemployment [15]. Other research shows that non-metropolitan areas are characterised by high levels of unemployment and suicide [16]. Taken together these findings suggest that the excess of suicides in young men in non-metropolitan areas may be as a result of their specific increased sensitivity to unemployment, levels of which are higher in non-metropolitan areas. However, this possible association is contentious and requires further exploration.
Suicide is associated with a wide range of other individual risk factors including psychiatric illness and alcohol and substance abuse [17]. At a societal level it is likely to reflect levels of social fragmentation, alienation and division [18]. Non-metropolitan Australia is currently suffering increasing levels of economic hardship and a sense of separation or alienation from more affluent metropolitan settings. In its publication Bush talks the Human Rights and Equal Opportunity Commission (HREOC) notes ‘people in non-metropolitan Australia generally come off second best. Distance, isolation, lower incomes and minority status all exacerbate the experience of discrimination, harassment, and lack of services and participation’ [19]. Participants in the HREOC meetings in Albany, Western Australia noted that the ‘economic downturn with the resulting sense of hopelessness and despair is a major factor contributing to the high rate of non-metropolitan suicides. A lot of people who get put on the economic scrap heap through no fault of their own feel an enormous sense of worthlessness’. The rural disadvantage in terms of health status and access to health care has been well documented [4].
It is noteworthy that differences in suicide rates between metropolitan and non-metropolitan areas seem confined to 15–24-year-old men. This is despite rises in youth suicide occurring in 15–24 and 25–34-year-olds in both settings, suggesting different aetiology and need for different preventive strategies. It will be important to continue to monitor suicide rates in non-metropolitan Australia, to conduct more research to understand more about why young non-metropolitan men are especially vulnerable and to develop interventions to reduce non-metropolitan suicide.
Footnotes
Acknowledgements
This study was funded by the Commonwealth Department of Health and Aged Care, Australia and South and West National Health System Research and Development, England.